📋 Key Information Summary
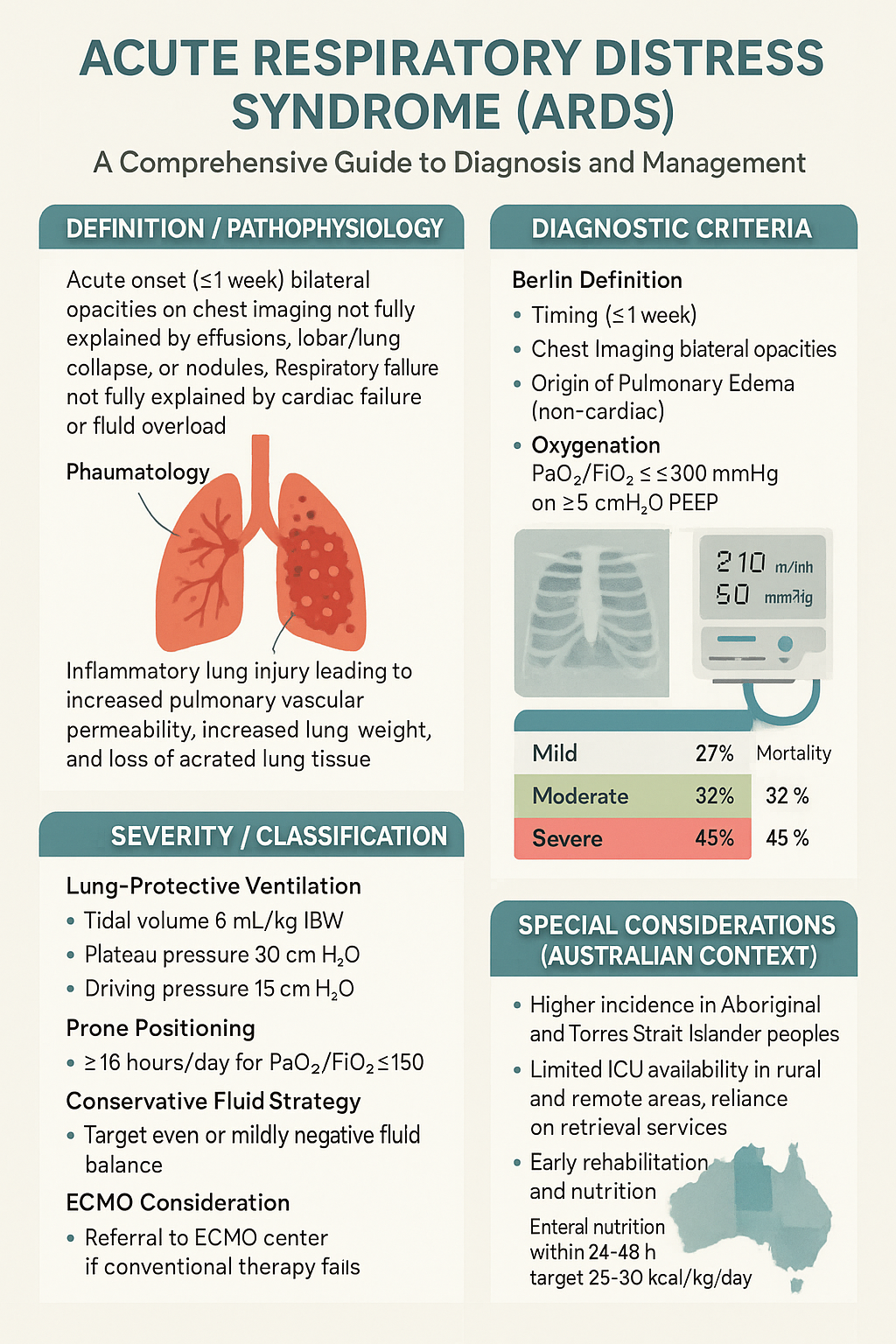
- ARDS definition: Acute onset (≤1 week) bilateral opacities on chest imaging not fully explained by effusions, lobar/lung collapse, or nodules, with respiratory failure not fully explained by cardiac failure or fluid overload, with a PaO2/FiO2 ratio ≤300 mmHg on ≥5 cmH2O PEEP.
- Berlin severity classification: Mild (200 < PaO2/FiO2 ≤300), Moderate (100 < PaO2/FiO2 ≤200), and Severe (PaO2/FiO2 ≤100) — all measured on ≥5 cmH2O PEEP.
- Leading causes in Australia: Pneumonia (most common), sepsis (non-pulmonary), aspiration, trauma, massive transfusion, pancreatitis, and near-drowning.
- Lung-protective ventilation is the cornerstone of management: Tidal volume 6 mL/kg IBW, plateau pressure (Pplat) <30 cmH2O, and driving pressure <15 cmH2O.
- Prone positioning for ≥16 hours/day is mandatory for all patients with moderate-to-severe ARDS (PaO2/FiO2 ≤150) and strongly recommended for mild ARDS with refractory hypoxaemia.
- Conservative fluid strategy after initial resuscitation — target even or mildly negative cumulative fluid balance to reduce ventilator days and ICU length of stay.
- Neuromuscular blockade (cisatracurium) may be considered in the first 48 hours for severe ARDS with refractory hypoxia or dyssynchrony, though routine use for 48-hour infusions is no longer standard after the ROSE trial.
- ECMO (VV-ECMO) should be considered when conventional therapy fails — refer to a designated ECMO centre (Melbourne, Sydney, Brisbane, Adelaide, Perth). EOLIA criteria: PaO2/FiO2 <50 for >3 hours or <80 for >6 hours despite optimal therapy.
- Venous thromboembolism prophylaxis is essential — use enoxaparin 40 mg SC daily (renal-adjusted) or unfractionated heparin 5,000 units SC BD unless contraindicated.
- Aboriginal and Torres Strait Islander peoples experience higher rates of pneumonia, sepsis, and delayed access to critical care — rural and remote communities face significant barriers to ECMO and specialist retrieval services.
- Early rehabilitation (within 72 hours of ICU stabilisation) reduces post-intensive care syndrome, ICU-acquired weakness, and improves functional recovery at 6 months.
- Nutrition targets: Commence enteral nutrition within 24–48 hours, target 25–30 kcal/kg/day and 1.2–2.0 g protein/kg/day; avoid parenteral nutrition in the first 7 days unless enteral route is contraindicated.
- In-hospital mortality remains 35–45% for severe ARDS in Australian ICUs. Early recognition, protocolised lung-protective ventilation, and escalation to specialist centres improve outcomes.
🎧 Audio Brief
Introduction & Australian Epidemiology
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening form of respiratory failure characterised by acute, diffuse, inflammatory lung injury leading to increased pulmonary vascular permeability, increased lung weight, and loss of aerated lung tissue. ARDS represents a spectrum of severity and is a common reason for ICU admission in Australian hospitals, accounting for approximately 10–15% of all ICU admissions and up to 23% of mechanically ventilated patients.
The landmark ARDSNet trial (2000) demonstrated a 22% relative reduction in mortality with low tidal volume ventilation (6 mL/kg IBW versus 12 mL/kg IBW), establishing lung-protective ventilation as the standard of care. Despite advances, ARDS remains under-recognised globally — the LUNG SAFE study found that 40% of ARDS cases were not identified by clinicians.
Australian Incidence and Burden
- The incidence of ARDS in Australian and New Zealand ICUs is estimated at 82–95 cases per 100,000 population per year (ANZICS data).
- In-hospital mortality: mild ARDS ~27%, moderate ARDS ~32%, severe ARDS ~45%.
- The COVID-19 pandemic significantly increased ARDS presentations, with Victorian and NSW ICUs managing surge capacity during 2020–2022.
- Aboriginal and Torres Strait Islander Australians have a 1.5–2× higher incidence of severe pneumonia and sepsis (the leading triggers of ARDS) compared with non-Indigenous Australians.
- ICU bed availability in rural and remote Australia is limited — retrieval services (e.g., Royal Flying Doctor Service, NSW Air Ambulance, QGAP) are critical for timely escalation.
Common Aetiological Triggers
| Pulmonary (Direct) | Extrapulmonary (Indirect) |
|---|---|
| Community-acquired pneumonia (bacterial, viral including SARS-CoV-2, influenza) | Non-pulmonary sepsis (e.g., intra-abdominal, urinary) |
| Aspiration of gastric contents | Major trauma / burns |
| Inhalational injury (smoke, toxic gas) | Massive transfusion (≥10 units pRBCs in 24 hours) |
| Pneumocystis jirovecii pneumonia (immunocompromised) | Acute pancreatitis |
| Pulmonary contusion | Drug overdose (opioids, salicylates, tricyclics) |
| Near-drowning | Cardiopulmonary bypass (post-cardiac surgery) |
Berlin Definition — Diagnostic Criteria & Severity Classification
The Berlin Definition (2012) replaced the earlier American–European Consensus Conference (AECC) criteria and provides a more reliable framework for ARDS diagnosis and severity stratification. The definition has four required components and three severity categories.
Required Criteria (All Four Must Be Met)
Berlin Severity Classification
Risk Factors for ARDS
| Direct Lung Injury | Indirect Lung Injury | Patient-Related Risk Factors |
|---|---|---|
| Pneumonia (most common) | Sepsis (non-pulmonary) | Chronic alcohol abuse (3× increased risk) |
| Aspiration | Polytrauma / burns | Smoking (current) |
| Inhalation injury | Massive transfusion | Obesity (BMI >30) |
| Pulmonary contusion | Pancreatitis | Diabetes mellitus (type 2) |
| Near-drowning | Cardiopulmonary bypass | Immunosuppression |
Mechanical Ventilation — Lung-Protective Strategy
Lung-protective ventilation is the single most important intervention that improves survival in ARDS. The strategy centres on low tidal volumes, limited plateau pressures, and appropriate PEEP to prevent both ventilator-induced lung injury (VILI) from volutrauma/barotrauma and atelectrauma from cyclic alveolar collapse.
Ideal Body Weight (IBW) Calculation
Tidal volume is set according to ideal body weight (IBW), not actual body weight, to avoid volutrauma in obese patients and underventilation in underweight patients.
| Parameter | Formula (Males) | Formula (Females) |
|---|---|---|
| IBW (kg) | 50 + 0.91 × (height in cm − 152.4) | 45.5 + 0.91 × (height in cm − 152.4) |
Ventilator Settings — Step-by-Step Protocol
ARDSNet PEEP / FiO2 Titration Table
| FiO2 | 0.3 | 0.4 | 0.4 | 0.5 | 0.5 | 0.6 | 0.7 | 0.7 | 0.8 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PEEP (cmH2O) | 5 | 5 | 8 | 8 | 10 | 10 | 10 | 12 | 14 | 14 | 14–18 |
Non-Invasive Ventilation (NIV) in ARDS
- NIV (BiPAP/CPAP) may be trialled in mild ARDS only (PaO2/FiO2 200–300) in patients without haemodynamic instability, multi-organ failure, or altered consciousness.
- HFNO (high-flow nasal oxygen) at up to 60 L/min may be used in mild ARDS, particularly in immunocompromised patients where intubation risk is high (FLORALI trial).
- Failure criteria: If PaO2/FiO2 <150 after 1–2 hours of NIV/HFNO, or RR >30, or haemodynamic instability, proceed to invasive ventilation. Delayed intubation increases mortality.
Rescue Oxygenation — Apnoeic Oxygenation
- During intubation of ARDS patients, use apnoeic oxygenation (15 L/min via nasal prongs + 15 L/min via ETT in pharynx) to extend safe apnoea time.
- Pre-oxygenate with 100% FiO2 for ≥3 minutes in a semi-recumbent position, or use NIV/CPAP for pre-oxygenation.
- Have a failed intubation plan — video laryngoscope as first-line device in ICU intubations (difficult airway more likely in critically ill, obese, or oedematous patients).
Advanced Therapies — Prone Positioning, Neuromuscular Blockade, Recruitment, ECMO
Prone Positioning
Prone positioning is one of the most effective interventions for moderate-to-severe ARDS. The PROSEVA trial (2013) demonstrated an absolute mortality reduction of 16.8% (28-day mortality 16% vs 32.8%) in patients with PaO2/FiO2 <150 when prone sessions lasted ≥16 hours per day.
- Technique: Minimum 3–5 staff required. Use a prone positioning bed or mattress overlay. Secure ETT, central lines, chest drains, and urinary catheter. Pad pressure points (face, shoulders, pelvis, knees). Reposition arms every 2 hours.
- Duration: ≥16 hours per session (20 hours preferred). Typically 1–2 sessions may be required; some patients need prolonged prone ventilation over days.
- Monitoring: Continuous SpO2, ETCO2, arterial line BP. Check ETT position after each turn. Monitor for ETT displacement, loss of IV access, brachial plexus injury, and pressure injuries.
- Contraindications: Unstable spinal fracture, open abdomen, haemodynamic instability requiring escalating vasopressors (relative), severe facial/neck burns, recent sternotomy (relative — discuss with cardiac surgery).
Neuromuscular Blocking Agents (NMBAs)
The role of NMBAs in ARDS has evolved. The ACURASYS trial (2010) showed benefit with 48-hour cisatracurium infusion in severe ARDS, but the larger ROSE trial (2019) found no difference in 90-day mortality with routine NMBA use. Current practice favours early, short-term use for specific indications rather than a blanket 48-hour protocol.
Recruitment Manoeuvres
Recruitment manoeuvres (RMs) aim to reopen collapsed alveoli. The ART trial (2017) showed that a staircase recruitment manoeuvre with PEEP titration did not reduce mortality and may have caused harm (barotrauma, haemodynamic compromise). Current recommendations are cautious.
- Sustained inflation: CPAP 35–40 cmH2O for 30–40 seconds. Simple but may cause haemodynamic compromise and barotrauma. Not routinely recommended.
- Staircase / incremental PEEP recruitment: Increase PEEP in steps of 5 cmH2O (with constant driving pressure) while monitoring compliance. Not recommended as a routine strategy (ART trial).
- Practical approach: A single brief sustained inflation (30 cmH2O for 30 seconds) may be used transiently after disconnect events (suctioning, prone turn) to restore oxygenation. Titrate PEEP using a decremental PEEP trial after recruitment if attempted.
- Contraindications: Barotrauma (pneumothorax), haemodynamic instability, bullous lung disease, raised intracranial pressure.
Extracorporeal Membrane Oxygenation (ECMO)
Venovenous ECMO (VV-ECMO) provides gas exchange when the lungs are unable to maintain adequate oxygenation and/or ventilation despite maximal conventional therapy. The EOLIA trial (2018) showed a trend towards improved survival with early ECMO in severe ARDS, though the crossover rate complicates interpretation. Meta-analyses suggest a significant mortality benefit.
• PaO2/FiO2 <50 mmHg for >3 hours OR PaO2/FiO2 <80 mmHg for >6 hours despite optimal therapy (including prone positioning)
• Uncompensated hypercapnia with pH <7.20 despite maximising ventilation
• Excessive plateau pressures (>30 cmH2O despite VT 4 mL/kg IBW)
• Murray Lung Injury Score ≥2.5–3.0
• Reversible underlying cause (avoid ECMO in irreversible multi-organ failure)
Australian ECMO Centres
- Victoria: The Alfred Hospital, Royal Melbourne Hospital
- New South Wales: Royal Prince Alfred Hospital, St Vincent's Hospital, Westmead Hospital
- Queensland: Prince Charles Hospital, Royal Brisbane and Women's Hospital
- South Australia: Royal Adelaide Hospital
- Western Australia: Royal Perth Hospital, Fiona Stanley Hospital
- Tasmania, NT, ACT: Retrieval and transfer to mainland ECMO centres via RFDS, NETS, or state retrieval services.
Adjunctive Pharmacotherapies
Supportive Care — Fluid Management, Nutrition, Sedation, Complications, Rehabilitation
Fluid Management
The FACTT trial demonstrated that a conservative fluid strategy (targeting even or mildly negative cumulative fluid balance after initial resuscitation) reduced ventilator days and ICU length of stay without increasing non-pulmonary organ failure. Liberal fluid administration worsens pulmonary oedema and prolongs mechanical ventilation.
Nutrition
Early enteral nutrition (EN) within 24–48 hours of ICU admission reduces infectious complications, maintains gut mucosal integrity, and may reduce duration of mechanical ventilation. Parenteral nutrition (PN) should be avoided in the first 7 days unless the enteral route is contraindicated (ESPEN/ANZICS guidelines).
| Parameter | Recommendation |
|---|---|
| Timing | Commence EN within 24–48 hours (if haemodynamically stable on low-dose vasopressors, EN can proceed) |
| Route | Nasoenteric (post-pyloric/nasojejunal preferred if gastric residual >250 mL repeatedly). Nasogastric acceptable as first-line. |
| Caloric target | Indirect calorimetry where available. Otherwise: 25–30 kcal/kg/day (use IBW). In acute phase (first 7 days), consider permissive underfeeding (up to 70% of target). |
| Protein target | 1.2–2.0 g protein/kg/day (IBW). Higher protein intake (≥1.5 g/kg) is associated with reduced mortality in ARDS. |
| Monitoring | Gastric residual volumes (GRV) every 4–6 hours; hold EN if GRV >500 mL. Monitor phosphate, magnesium, potassium (refeeding risk). |
| Omega-3 fatty acids | Not routinely recommended. The OMEGA trial and subsequent meta-analyses showed no benefit from EPA/DHA supplementation in ARDS. |
Sedation and Analgesia
ARDS patients require deeper sedation than general ICU patients, particularly during prone positioning and when using NMBAs. However, daily sedation interruption and minimising sedation depth when safe reduces ventilator days, delirium, and ICU length of stay (eCASH concept: early Comfort using Analgesia, minimal Sedation, and maximal Humane care).
Delirium Prevention and Management
- Assess using CAM-ICU (Confusion Assessment Method for ICU) twice daily.
- Non-pharmacological strategies: lightening sedation daily, early mobilisation, sleep hygiene (reducing noise and light at night), reorientation, family presence, hearing aids and glasses where applicable.
- Avoid antipsychotics routinely. Haloperidol 2.5–5 mg IV/IM may be used for acute agitation with safety risk. Quetiapine 12.5–25 mg PO/NG BD may be considered for hypoactive delirium (limited evidence).
- Avoid benzodiazepines as primary sedative — associated with increased delirium, longer ventilation, and worse outcomes (MIDEX/PRODEX trials).
Venous Thromboembolism (VTE) Prophylaxis
- First-line: Enoxaparin 40 mg SC once daily (adjust for weight: 0.5 mg/kg if >100 kg; 30 mg daily if <50 kg or eGFR <30 mL/min/1.73 m²).
- Renal impairment (eGFR <30): Unfractionated heparin (UFH) 5,000 units SC BD, or enoxaparin 30 mg SC daily with anti-Xa level monitoring (target 0.2–0.5 IU/mL).
- Mechanical prophylaxis: Intermittent pneumatic compression (IPC) devices on lower limbs. Use in combination with pharmacological prophylaxis or as sole method if anticoagulation contraindicated.
Prevention of Stress Ulceration
- Stress ulcer prophylaxis with a proton pump inhibitor (PPI) is recommended for mechanically ventilated patients >48 hours with additional risk factors (coagulopathy, shock, corticosteroids).
- Pantoprazole 40 mg IV/PO daily (PBS General Benefit). Omeprazole 20 mg PO/NG is an alternative.
- The PEPTIC trial (2020) showed no significant difference in 90-day mortality between PPI and H2RA; PPI remains preferred due to superior acid suppression.
Ventilator-Associated Pneumonia (VAP) Prevention
- Elevate head of bed to 30–45° (except during prone positioning).
- Daily oral care with chlorhexidine 0.12% solution (evidence is mixed; many Australian ICUs use it per NSQHS Standards).
- Subglottic suctioning ETT where available.
- Daily sedation interruption and spontaneous breathing trials to assess readiness for extubation.
- Closed suction systems, heat-movent exchangers (HME) with filter, and minimising circuit disconnections.
Early Rehabilitation in ARDS
ICU-acquired weakness (ICU-AW) affects up to 40–50% of ARDS patients and is the strongest predictor of poor functional outcome at 6–12 months. Early rehabilitation, commencing within 72 hours of ICU stabilisation, is a key component of the recovery bundle.
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. ARDS Definition Task Force; Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533.
- 2. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308.
- 3. Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-2168.
- 4. Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107-1116.
- 5. National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss M, Huang DT, Brower RG, et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl J Med. 2019;380(21):1997-2008.
- 6. Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome (EOLIA). N Engl J Med. 2018;378(21):1965-1975.
- 7. Amato MB, Meade MO, Slutsky AS, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747-755.
- 8. National Heart, Lung, and Blood Institute ARDS Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564-2575.
- 9. Cavalcanti AB, Suzumura ÉA, Laranjeira LN, et al. Effect of lung recruitment and titrated PEEP (ART) vs low PEEP on mortality in patients with ARDS: a randomized clinical trial (ART). JAMA. 2017;318(14):1335-1345.
- 10. Villar J, Ferrando C, Martínez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial (Dexa-ARDS). Lancet Respir Med. 2020;8(3):267-276.
- 11. RECOVERY Collaborative Group; Horby P, Lim WS, Emberson JR, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384(8):693-704.
- 12. Australian and New Zealand Intensive Care Society (ANZICS). ANZICS COVID-19 Guidelines. Melbourne: ANZICS; 2022.
- 13. Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries (LUNG SAFE). JAMA. 2016;315(8):788-800.
- 14. Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults (SMART trial). N Engl J Med. 2018;378(9):829-839.
- 15. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 16. Centre for Remote Health / CARPA. Central Australian Rural Practitioners Association Standard Treatment Manual. 8th ed. Alice Springs: Centre for Remote Health; 2022.
- 17. Fan E, Del Sorbo L, Goligher EC, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-1263.
- 18. Griffiths MJD, McAuley DF, Perkins GD, et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir Res. 2019;6(1):e000420.
- 19. National Health and Medical Research Council (NHMRC). Australian Clinical Practice Guidelines for the Management of Acute Respiratory Distress Syndrome. Canberra: NHMRC; 2021.
- 20. Hodgson CL, Capellier DM, Davies AR, et al. Early mobilisation in Australian and New Zealand intensive care units: a point prevalence study. Crit Care Resusc. 2019;21(4):270-275.