📋 Key Information Summary
- Definition: COPD is a progressive, largely irreversible airflow limitation characterised by persistent respiratory symptoms and airflow obstruction; post-bronchodilator FEV1/FVC <0.70 confirms diagnosis.
- Prevalence: Approximately 7.5% of Australians aged ≥40 years have COPD; it is the fifth leading cause of death nationally and disproportionately affects Aboriginal and Torres Strait Islander peoples.
- GOLD Classification: The GOLD 2024 ABCD framework classifies patients by spirometric severity (GOLD 1–4), exacerbation history (≥2 moderate or ≥1 hospitalised in past year), and symptom burden (mMRC ≥2 or CAT ≥10).
- First-line pharmacotherapy: LAMA (e.g. tiotropium) monotherapy for most initial presentations; LABA+LAMA combination for persistent dyspnoea or higher symptom burden (Group B/E).
- ICS use: Inhaled corticosteroids are indicated only for patients with elevated eosinophils (≥300 cells/µL) or frequent exacerbations despite LABA+LAMA; never as monotherapy in COPD.
- Triple therapy (ICS+LABA+LAMA): Reserved for patients with persistent exacerbations on dual bronchodilation with eosinophil ≥100 cells/µL; evidence from IMPACT and ETHOS trials demonstrates mortality benefit.
- Acute exacerbations: Managed with short-acting bronchodilators (SABA ± SAMA), systemic corticosteroids (prednisolone 40 mg for 5 days), and antibiotics if Anthonisen Type 1 or purulent sputum; NIV for acute hypercapnic respiratory failure.
- Pulmonary rehabilitation: Strongly recommended for all symptomatic COPD patients; reduces hospital admissions, improves exercise capacity and quality of life; available through many Australian public hospitals and community programmes.
- Smoking cessation: The single most effective intervention to slow FEV1 decline; pharmacotherapy (varenicline, NRT) combined with behavioural support achieves the highest quit rates.
- Long-term oxygen therapy (LTOT): Improves survival when PaO2 ≤55 mmHg (or ≤59 mmHg with cor pulmonale/polycythaemia); prescribed ≥15 hours/day via concentrator or cylinder — funded through the Australian Integrated Aids and Equipment Programme.
- Alpha-1 antitrypsin deficiency: Screen all COPD patients aged <45 years, those with a strong family history, or with predominantly basal emphysema on CT.
- Vaccinations: Annual influenza, pneumococcal (PCV20 or PCV15+PPV23), COVID-19, and zoster (≥50 years) — all funded under the National Immunisation Programme for eligible patients.
- ATSI considerations: COPD prevalence in First Nations Australians is 2.5 times higher; earlier onset, greater severity, and higher mortality. Culturally safe spirometry, smoking cessation, and pulmonary rehabilitation access in remote communities are essential.
Introduction & Australian Epidemiology
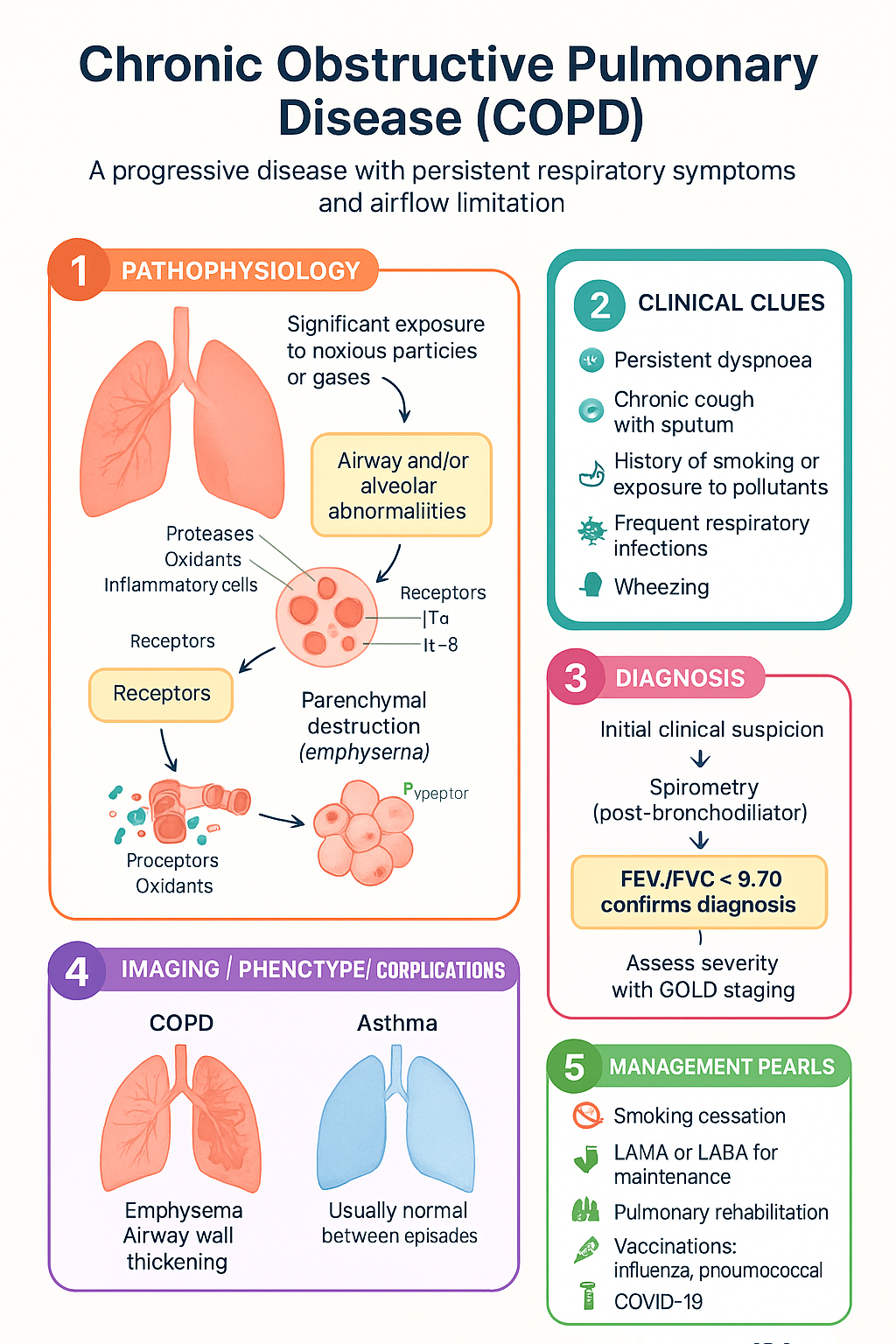
Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable, and treatable disease characterised by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases. The chronic airflow limitation is caused by a combination of small airway disease (obstructive bronchiolitis) and parenchymal destruction (emphysema), the relative contributions of which vary between individuals.
Australian Burden of Disease
- COPD affects approximately 1 in 13 Australians aged ≥40 years (BOLD-Australia study), with many cases remaining undiagnosed.
- It is the fifth leading cause of death in Australia and the third leading cause of disease burden in males (AIHW Burden of Disease, 2023).
- In 2021–22, COPD accounted for over 230,000 hospitalisations nationally, with a mean length of stay of 5.3 days — significantly longer than the all-cause average.
- The total economic cost of COPD in Australia is estimated at $8.9 billion annually, including direct healthcare costs, productivity losses, and informal carer burden.
- Aboriginal and Torres Strait Islander peoples experience 2.5 times the prevalence and 3 times the mortality rate of non-Indigenous Australians for COPD.
- COPD is over-represented in lower socioeconomic groups, rural and remote populations, and among current and former smokers.
Aetiology & Risk Factors
| Risk Factor | Details | Australian Context |
|---|---|---|
| Tobacco smoking | Accounts for ~70–80% of COPD cases; dose-dependent risk (pack-years) | 11.6% of Australian adults smoke daily (2022); higher in ATSI populations (~37%) |
| Occupational exposure | Dust, fumes, chemicals (10–20% of COPD) | Mining, agriculture, construction workers at elevated risk |
| Indoor air pollution | Biomass fuel combustion in poorly ventilated settings | Significant contributor in remote Indigenous communities using wood fires |
| Genetic predisposition | Alpha-1 antitrypsin deficiency (AATD) — PiZZ genotype | Estimated 1 in 2,500 Australians carry the PiZZ phenotype; under-diagnosed |
| Childhood respiratory illness | Severe childhood asthma, recurrent lower respiratory tract infections | Contributes to fixed airflow obstruction in younger adults |
| Asthma with persistent airflow limitation | Asthma–COPD overlap (ACO) phenotype | Common in Australian primary care; requires tailored management |
Diagnosis & Spirometry
The diagnosis of COPD requires a clinical history of chronic respiratory symptoms (dyspnoea, cough, sputum production) plus confirmation of persistent airflow obstruction by spirometry. Spirometry should be performed after administration of a short-acting bronchodilator (e.g. salbutamol 400 µg) to confirm that the obstruction is not fully reversible.
Spirometric Severity — GOLD Staging
| GOLD Stage | Severity | Post-BD FEV1 (% Predicted) | Clinical Implications |
|---|---|---|---|
| GOLD 1 | Mild | ≥80% | Often unrecognised; mild symptoms; may not seek medical attention |
| GOLD 2 | Moderate | 50–79% | Most commonly diagnosed stage; exertional dyspnoea; usual presentation in primary care |
| GOLD 3 | Severe | 30–49% | Significant functional limitation; frequent exacerbations; specialist referral warranted |
| GOLD 4 | Very Severe | <30% | Quality of life markedly impaired; may need long-term oxygen therapy; evaluate for advanced therapies |
Differential Diagnosis: COPD vs Asthma
| Feature | COPD | Asthma |
|---|---|---|
| Age of onset | Typically >40 years | Often childhood or early adulthood |
| Smoking history | Usually ≥10 pack-years | May or may not be present |
| Symptom pattern | Persistent, progressive; morning cough productive | Episodic, nocturnal, variable; triggers identifiable |
| Airflow obstruction | Partially or not reversible | Usually fully reversible (post-BD FEV1 improves ≥200 mL and ≥12%) |
| Atopy / Eosinophilia | Variable; eosinophils may guide ICS use | Common; elevated IgE, blood eosinophils |
| HRCT chest | Emphysema, airway wall thickening | Usually normal between episodes |
Alpha-1 Antitrypsin Screening
- Indications for screening: All patients diagnosed with COPD aged <45 years; any age if emphysema is predominantly basal (lower lobe predominant on CT); strong family history of COPD or liver disease; or unexplained liver disease in neonates/children.
- Initial test: Serum alpha-1 antitrypsin (AAT) level — if below 1.13 g/L (lower limit of normal), proceed to phenotyping by isoelectric focusing.
- Diagnosis confirmed: PiZZ, PiSZ, or PiNull phenotypes with AAT level <0.57 g/L (11 µM) confer significant risk for early emphysema.
- Management: Augmentation therapy (IV pooled AAT — available via Special Access Scheme in Australia) considered in PiZZ patients with established emphysema and FEV1 35–60% predicted; smoking cessation and vaccination are paramount.
- Family screening: First-degree relatives of confirmed AATD patients should be offered targeted testing (serum level + phenotyping).
Investigations — Diagnostic Workup
Risk Assessment & Classification
The GOLD 2024 report simplifies the previous ABCD tool into an ABE framework, emphasising the importance of both exacerbation risk and symptom burden in guiding initial and follow-up pharmacotherapy decisions.
Symptom Assessment Tools
Modified Medical Research Council (mMRC) Dyspnoea Scale
| Grade | Description | Significance |
|---|---|---|
| 0 | Breathless only with strenuous exercise | Low symptom burden |
| 1 | Short of breath when hurrying on level or walking up a slight hill | Low symptom burden |
| 2 | Walks slower than people of same age on level due to breathlessness, or stops for breath at own pace | Symptomatic — threshold for treatment escalation |
| 3 | Stops for breath after walking ~100 metres or after a few minutes on level | High symptom burden |
| 4 | Too breathless to leave house, or breathless when dressing/undressing | Very high symptom burden |
COPD Assessment Test (CAT)
- Eight-item questionnaire scored 0–40; assesses cough, phlegm, chest tightness, breathlessness, activity limitation, confidence leaving home, sleep, and energy.
- CAT <10 = low symptom burden; CAT ≥10 = high symptom burden.
- Use either mMRC or CAT — CAT is preferred as it captures a broader symptom profile.
GOLD 2024 ABE Classification
Exacerbation Risk Assessment
- Moderate exacerbation: Requires treatment with systemic corticosteroids and/or antibiotics but not hospitalisation.
- Severe exacerbation: Requires hospitalisation or presents to the emergency department.
- Very severe exacerbation: Requires ICU admission, may involve NIV or mechanical ventilation.
- Blood eosinophil count is now a key biomarker: ≥300 cells/µL predicts ICS benefit in reducing exacerbations; <100 cells/µL suggests ICS is unlikely to be helpful and may increase pneumonia risk.
Additional Prognostic Tools
| Tool | Components | Use |
|---|---|---|
| BODE Index | BMI, Obstruction (FEV1), Dyspnoea (mMRC), Exercise (6MWD) | Composite mortality predictor; score 0–10; ≥7 indicates high risk |
| DEOSS | Dyspnoea, Eosinophils, Obstruction, Smoking status, Severity of exacerbations | Australian-developed tool for exacerbation risk prediction |
| DOSE Index | Dyspnoea (mMRC), Obstruction (FEV1), Smoking status, Exacerbation frequency | Primary care screening; score ≥4 warrants specialist review |
Pharmacologic Management
Pharmacotherapy for COPD aims to reduce symptoms, improve exercise tolerance and quality of life, and reduce exacerbation frequency and severity. The GOLD 2024 strategy recommends a stepwise approach based on the ABE classification, with escalation and de-escalation guided by symptom response, exacerbation history, eosinophil count, and adverse effects.
Bronchodilator Therapy — Initial Approach
LAMA (Long-Acting Muscarinic Antagonist) Monotherapy
LABA + LAMA Dual Bronchodilation
Inhaled Corticosteroids (ICS) — Indications & Prescribing
Triple Therapy — ICS + LABA + LAMA
Triple therapy is indicated for patients with persistent exacerbations (≥2 moderate or ≥1 hospitalised) despite LABA+LAMA dual therapy AND eosinophil count ≥100 cells/µL. Landmark trials (IMPACT, ETHOS) demonstrated significant reductions in exacerbations and all-cause mortality with single-inhaler triple therapy.
PDE4 Inhibitors
Pharmacotherapy Escalation & De-escalation Summary
| Scenario | Action | Key Considerations |
|---|---|---|
| Persistent dyspnoea on LAMA monotherapy | Escalate to LABA + LAMA | Check inhaler technique and adherence first |
| Exacerbations on LABA+LAMA, eosinophils ≥300 | Add ICS → triple therapy | Single-inhaler preferred for adherence; assess pneumonia risk |
| Exacerbations on LABA+LAMA, eosinophils 100–299 | Consider adding ICS or roflumilast | Chronic bronchitis phenotype favours roflumilast |
| Exacerbations on LABA+LAMA, eosinophils <100 | Consider roflumilast or azithromycin prophylaxis | ICS unlikely to be beneficial; macrolide via specialist |
| Pneumonia on triple therapy | Withdraw ICS; continue LABA+LAMA | Gradual withdrawal recommended; monitor for recurrence of exacerbations |
Acute Exacerbations
An acute exacerbation of COPD (AECOPD) is defined as an acute worsening of respiratory symptoms beyond normal day-to-day variation that necessitates a change in therapy. Exacerbations accelerate lung function decline, impair quality of life, and are the leading cause of COPD-related hospitalisation and mortality in Australia.
Anthonisen Criteria
Antibiotic Therapy for AECOPD
Systemic Corticosteroids in AECOPD
Short-Acting Bronchodilators (Acute Setting)
Non-Invasive Ventilation (NIV)
- Mode: Bilevel positive airway pressure (BiPAP) — initial settings IPAP 10–12 cmH2O, EPAP 4–5 cmH2O; titrate to achieve tidal volume 6–8 mL/kg and target SpO2 88–92%.
- Monitoring: ABG at 1–2 hours; if pH remains <7.25 or deteriorating, escalate to ICU for intubation consideration.
- Contraindications: Cardiac/respiratory arrest, inability to protect airway, undrained pneumothorax, severe haemodynamic instability, facial burns/trauma, uncooperative patient.
- Post-acute: Continue NIV for ≥4 hours initially, then wean as tolerated; aim for ≥16 hours/day until respiratory acidosis resolves.
Hospitalisation Decision Framework
| Manage in Community | Admit to Ward | Admit to HDU/ICU |
|---|---|---|
| Mild exacerbation (Type 3) | Type 1–2 exacerbation not responding to initial therapy | Severe respiratory acidosis (pH <7.25) |
| Adequate SpO2 ≥92% on room air | SpO2 <92% requiring supplemental O2 | NIV failure or need for invasive ventilation |
| Good home support and monitoring | Significant comorbidities (heart failure, diabetes) | Haemodynamic instability / shock |
| Previously mild COPD, stable baseline | Previous ICU admissions or mechanical ventilation | Altered consciousness / respiratory arrest |
Hospital in the Home (HITH) — Australian Model
- Several Australian health services offer Hospital in the Home for selected AECOPD, with IV antibiotics, nebulised bronchodilators, and daily nursing visits.
- Eligible patients: stable on initial treatment, able to manage at home with support, no requirement for continuous monitoring or NIV, adequate oxygen saturations on low-flow supplemental O2.
- Reduces hospital length of stay, hospital-acquired infections, and delirium risk; patient satisfaction is high.
Non-Pharmacologic Management
Non-pharmacological interventions are integral to comprehensive COPD management and are recommended for all patients across all GOLD stages. These interventions address exercise capacity, symptom burden, disease progression, and quality of life.
Pulmonary Rehabilitation
- Programme components: Supervised exercise training (minimum 6 weeks, ideally 8 weeks), education, nutritional advice, psychosocial support, self-management strategies.
- Exercise prescription: Aerobic (walking or cycling) 20–30 min, 2–3 times/week at 60–80% peak work rate; resistance training for upper and lower limbs; flexibility and balance components.
- Australian availability: Offered through public hospitals (bulk-billed), community health centres, and some private practices. Referral pathways vary by state/territory — some require respiratory physician or GP referral.
- Maintenance: Long-term maintenance exercise following formal programme is critical to sustain benefits; community-based and telehealth options increasing across Australia.
Smoking Cessation
- Behavioural support: Combine pharmacotherapy with counselling (face-to-face, telephone via Quitline 13 7848, or digital programmes). The Australian Government funds Quitline services in all states and territories.
- A brief intervention (ABCD framework): Ask about smoking at every visit; Brief advice to quit; Counsel and assist (set quit date, provide NRT/pharmacotherapy); Do arrange follow-up.
Long-Term Oxygen Therapy (LTOT)
- Prescription: Oxygen concentrator (primary device) ± portable oxygen cylinder for mobility; flow rate titrated to achieve SpO2 88–92% (typical 1–3 L/min via nasal prongs).
- Australian funding: Funded through the state/territory Aids and Equipment programmes (e.g. SWEP in Victoria, ILC in NSW). Patients must be assessed by a respiratory physician or thoracic medicine specialist.
- Monitoring: ABG reassessment at 60–90 days to confirm ongoing need; annual review by respiratory specialist.
- Ambulatory oxygen: Consider for patients with significant exertional desaturation who are already on LTOT and remain mobile — may improve exercise capacity.
Vaccinations
| Vaccine | Schedule | Funding |
|---|---|---|
| Influenza (annual) | Every autumn; all COPD patients | Free under NIP for all Australians ≥65 or with chronic respiratory disease |
| Pneumococcal | PCV20 (single dose) or PCV15 followed by PPV23 ≥1 year later | Free under NIP for Aboriginal and Torres Strait Islander peoples ≥50 and all adults ≥65 |
| COVID-19 | As per current ATAGI recommendations; boosters recommended for immunocompromised and elderly | Free under NIP for all eligible Australians |
| Zoster (shingles) | Shingrix® (2 doses, 2–6 months apart) for adults ≥50; preferred over Zostavax | Free under NIP for adults ≥65; ATSI ≥50 |
| Pertussis (dTpa) | One booster if not received in past 10 years | Free under NIP (catch-up); funded for pregnant women |
Nutrition
- Low BMI (<20 kg/m²): Associated with increased mortality, reduced respiratory muscle strength, and worse quality of life. Refer to a dietitian for high-calorie, high-protein nutritional support.
- Obesity (BMI ≥30): Worsens dyspnoea and exercise tolerance; weight management is important but avoid excessive calorie restriction.
- Vitamin D: Supplementation (1,000–2,000 IU daily) may reduce moderate-to-severe exacerbations in patients with baseline 25(OH)D <25 nmol/L — test and replace if deficient.
- Small, frequent meals: Reduce diaphragmatic splinting and postprandial dyspnoea; avoid carbonated drinks and gas-producing foods.
Advanced COPD
Patients with advanced COPD (GOLD 4, BODE index ≥7, frequent exacerbations despite maximal medical therapy) should be evaluated for advanced interventional therapies and palliative care. Referral to a respiratory specialist or multidisciplinary advanced lung disease service is essential.
Surgical & Interventional Options
| Intervention | Indication | Key Criteria | Australian Availability |
|---|---|---|---|
| Lung Volume Reduction Surgery (LVRS) | Upper-lobe predominant emphysema with low baseline exercise capacity | FEV1 15–45%, heterogeneous emphysema on CT, PaCO2 ≤50 mmHg, no significant pulmonary hypertension | Available at major tertiary centres (e.g. Royal Prince Alfred, Alfred Hospital, Prince Charles Hospital); Medicare-funded |
| Endobronchial Valves (EBV) | Severe heterogeneous emphysema with complete fissure and no collateral ventilation | FEV1 15–45%, hyperinflation (RV >175%), intact interlobar fissure on CT (Chartis assessment) | Available at specialised interventional pulmonology centres; TGA-approved; PBS listing pending for devices |
| Bullectomy | Giant bullae (>30% hemithorax) compressing adjacent functional lung | Relatively preserved underlying lung parenchyma; heterogeneous disease with compression effect | Available at thoracic surgery centres; may be performed via VATS |
| Lung Transplantation | End-stage COPD refractory to all other therapies | BODE 7–10, FEV1 <15–20%, frequent hospitalisations, PaCO2 >50 mmHg, pulmonary hypertension, or rapid FEV1 decline | Available at St Vincent's Hospital (Sydney), Alfred Hospital (Melbourne), Prince Charles Hospital (Brisbane); waitlist 12–24 months |
Lung Transplant Evaluation — Practical Approach
- When to refer: Consider referral when BODE index ≥7 or any single criterion suggesting rapid decline (e.g. FEV1 <20% predicted, ≥3 exacerbations/year, or FEV1 decline >40 mL/year).
- Age limits: Most Australian centres accept patients up to 65 years for single lung and 60 years for bilateral transplant; selected patients older may be considered.
- Contraindications: Active malignancy, active infection (including non-treated TB), severe skeletal deformity, non-adherence, substance abuse (must demonstrate ≥6 months abstinence), BMI >35 or <17.
- Pre-transplant workup: Comprehensive cardiopulmonary assessment, CT chest/abdomen, coronary angiography if indicated, bone densitometry, psychological and social assessment, dental review, HLA typing.
Palliative Care
- When to refer: GOLD 4 with progressive decline, recurrent hospitalisations, refractory dyspnoea despite maximal therapy, significant symptom burden (CAT >20), patient-expressed preference for comfort-focused care.
- Symptom management: Low-dose opioids (oral morphine 2.5–5 mg BD) for refractory breathlessness; anxiolytics for associated anxiety; fan therapy; positioning and breathing techniques.
- Advance Care Planning: Document patient preferences regarding intubation, NIV, hospitalisation, and resuscitation. Use the National Advance Care Planning templates available from Advance Care Planning Australia.
- Community palliative care: Available in all Australian states and territories; referral via GP or hospital team. In remote areas, Royal Flying Doctor Service and specialist palliative care outreach programmes provide support.
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
COPD is one of the most significant chronic conditions affecting Aboriginal and Torres Strait Islander Australians, with prevalence approximately 2.5 times that of the non-Indigenous population and mortality rates 3 times higher. The burden is greatest in remote and very remote communities, where indoor wood-fire smoke exposure, high smoking rates, early-life respiratory infections, and limited access to diagnostic and treatment services compound the disease impact.
Monitoring & Follow-Up
Regular monitoring is essential to assess disease progression, treatment response, and complications. A structured follow-up plan should be established at the time of diagnosis and adjusted based on disease severity and stability.
Self-Management Action Plan
- All patients should have a written COPD Action Plan (similar to asthma action plans) with clear instructions for GREEN (stable), YELLOW (worsening — start prednisolone/antibiotics), and RED (severe — seek emergency care).
- Self-management education should cover recognition of exacerbation symptoms, early initiation of standby medications, correct inhaler and oxygen use, and when to call 000.
- Supported self-management (with regular follow-up) reduces hospital presentations and improves quality of life (Cochrane review evidence).
Quick Reference — Maintenance Therapy Summary
📚 References
- 1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2024 Report. Available at: goldcopd.org.
- 2. Yang IA, Brown JL, George J, et al. COPD-X Australian and New Zealand guidelines for the diagnosis and management of chronic obstructive pulmonary disease: 2024 update. Med J Aust. 2024;220(5):248–258.
- 3. Lipson DA, Barnhart F, Brealey N, et al. Once-single-inhaler triple therapy and the risk of mortality in patients with chronic obstructive pulmonary disease (IMPACT). N Engl J Med. 2018;378(18):1671–1680.
- 4. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD (ETHOS). N Engl J Med. 2020;383(1):35–48.
- 5. Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD (WISDOM). N Engl J Med. 2014;371(14):1285–1294.
- 6. Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease (REDUCE). JAMA. 2013;309(21):2223–2231.
- 7. Australian Institute of Health and Welfare (AIHW). Chronic obstructive pulmonary disease (COPD). Cat. no. ACM 35. Canberra: AIHW; 2023.
- 8. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Health Survey, 2018–19. ABS Cat. no. 4715.0. Canberra: ABS; 2019.
- 9. Yang IA, Johns DP, Toelle BG, et al. Spirometry in Australian general practice: a national audit of training, equipment, and practice. Med J Aust. 2020;212(8):364–369.
- 10. McCarthy B, Casey D, Devane D, et al. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793.
- 11. Stoller JK, Campos M. Alpha-1 antitrypsin deficiency. Lancet. 2023;401(10378):761–777.
- 12. National Asthma Council Australia. Australian Asthma Handbook, Version 2.2. Melbourne: NAC; 2024. [For ACO guidance].
- 13. Criner GJ, Sue R, Wright S, et al. A multicenter RCT of Zephyr endobronchial valves in heterogeneous emphysema (LIBERATE). Am J Respir Crit Care Med. 2018;198(9):1151–1164.
- 14. Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) Australia study. PLoS One. 2013;8(6):e66326.
- 15. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.