📋 Key Information Summary
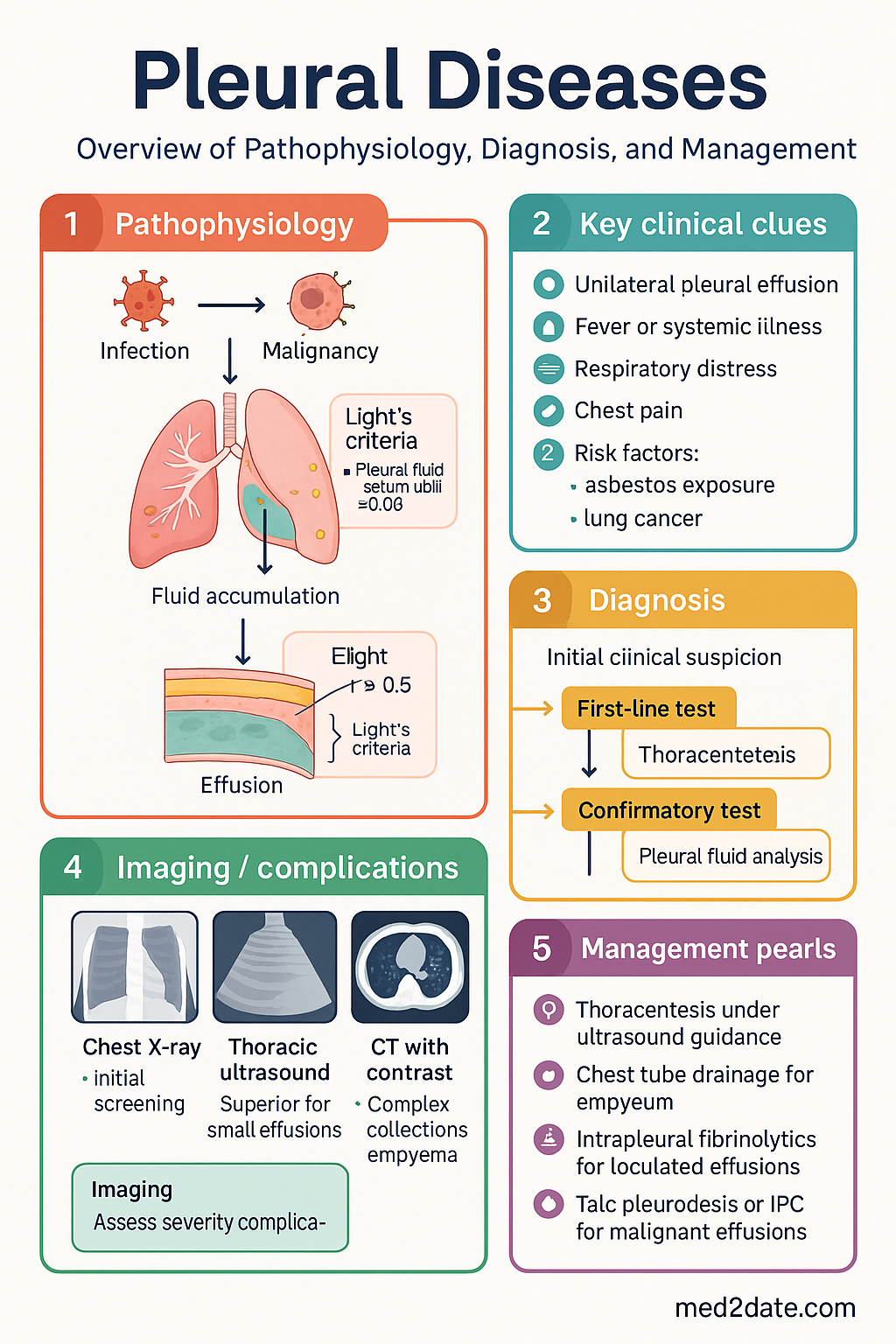
- Light's criteria remain the gold standard for distinguishing exudative from transudative pleural effusions — an effusion is exudative if it meets any one of: pleural fluid protein/serum protein > 0.5, pleural fluid LDH/serum LDH > 0.6, or pleural fluid LDH > two-thirds the upper limit of normal serum LDH.
- Diagnostic thoracentesis is indicated for all undiagnosed unilateral pleural effusions > 10 mm on ultrasound, and bilateral effusions that are clinically atypical or fail to respond to treatment of the suspected underlying cause.
- Parapneumonic effusions are staged as uncomplicated (free-flowing, culture-negative), complicated (loculated or pH < 7.2 or glucose < 3.3 mmol/L or positive Gram stain/culture), or empyema (frank pus) — complicated effusions and empyema require chest tube drainage and antibiotics.
- Intrapleural fibrinolytics (alteplase + DNase) are recommended for loculated parapneumonic effusions/empyema not responding to initial chest tube drainage, reducing the need for surgical intervention (MIST-2 trial).
- Malignant pleural effusion (MPE) is confirmed by pleural fluid cytology (sensitivity ~60%) or pleural biopsy; pleuroscopy (medical thoracoscopy) offers > 90% diagnostic sensitivity when cytology is non-diagnostic.
- For recurrent MPE, choice between talc pleurodesis and indwelling pleural catheter (IPC) should be guided by expected survival, lung re-expandability, and patient preference — IPC avoids hospital stay and is preferred when trapped lung is present.
- Primary spontaneous pneumothorax (PSP): small (< 2 cm rim at hilum) asymptomatic PSP can be observed with supplemental oxygen; larger or symptomatic PSP is managed with aspiration (first-line) then intercostal catheter (ICC) if aspiration fails.
- Secondary spontaneous pneumothorax (SSP) in patients with underlying lung disease (especially COPD) carries higher morbidity — all SSP should be admitted and an ICC is usually required; consider early surgical review for recurrence or persistent air leak.
- Chest X-ray remains the initial imaging modality for pleural disease; thoracic ultrasound is superior for detecting small effusions, guiding thoracentesis, and identifying septations; CT with contrast is indicated for complex collections, empyema, and staging MPE.
- Aboriginal and Torres Strait Islander Australians experience significantly higher rates of pneumonia, empyema, and pleural disease, particularly in remote communities — delayed presentation, barriers to specialist access, and higher background rates of rheumatic heart disease and chronic lung disease contribute to worse outcomes.
- All pleural procedures should be performed under ultrasound guidance where possible (NSQHS Standards) to reduce complication rates — pneumothorax rates drop from ~18% (landmark-guided) to ~3% (US-guided).
- Asbestos-related pleural disease (plaques, diffuse thickening, mesothelioma) is a significant burden in Australia due to historical asbestos mining (Wittenoom) and widespread use in construction — Australia has the highest per-capita rate of mesothelioma globally.
Introduction & Australian Epidemiology
Pleural diseases encompass a broad spectrum of conditions affecting the visceral and parietal pleura, ranging from benign effusions to life-threatening infections and malignancies. In Australia, pleural effusions are among the most common reasons for respiratory consultation, with an estimated 50,000–75,000 new cases annually across all causes. The management of pleural disease has evolved significantly over the past two decades, with the widespread adoption of thoracic ultrasound for procedural guidance, the advent of indwelling pleural catheters for malignant effusions, and the introduction of combined intrapleural fibrinolytic therapy for empyema.
The Australian burden of pleural disease is shaped by several unique factors:
- Asbestos legacy: Australia was one of the world's largest consumers and exporters of asbestos (crocidolite and chrysotile), particularly through the Wittenoom mine in Western Australia. Asbestos-related pleural disease — including benign plaques, diffuse pleural thickening, and malignant mesothelioma — remains a significant ongoing health burden. Australia has the highest per-capita incidence of mesothelioma in the world, with approximately 700–800 new cases diagnosed annually (Australian Institute of Health and Welfare, AIHW).
- Infectious disease burden: Parapneumonic effusions and empyema are disproportionately common in Aboriginal and Torres Strait Islander Australians, children in remote communities, and the elderly. Staphylococcus aureus and Streptococcus species remain the predominant causative organisms, with increasing recognition of antimicrobial resistance patterns.
- Malignant pleural effusion: Lung cancer, breast cancer, and mesothelioma are the three most common causes of MPE in Australia, collectively accounting for approximately 75% of cases. The median survival following MPE diagnosis ranges from 4 months (lung cancer) to 12–22 months (breast cancer).
- Pneumothorax: The incidence of primary spontaneous pneumothorax in Australia is approximately 7–18 per 100,000 per year in males and 1–6 per 100,000 in females, with higher rates observed in tall, thin young adults and smokers.
Pleural Effusion Diagnosis
Approach to Diagnosis
The diagnostic evaluation of a pleural effusion follows a systematic approach: confirm the presence of fluid, determine the cause (transudate vs exudate), and identify the specific aetiology. Thoracentesis is the cornerstone investigation and should be performed in virtually all undiagnosed unilateral effusions, bilateral effusions of uncertain aetiology, and any effusion associated with fever or systemic illness.
Light's Criteria — Exudate vs Transudate
Light's criteria, first published in 1972, remain the most validated and widely used method for distinguishing exudative from transudative pleural effusions. An effusion is classified as an exudate if it meets any one of the following three criteria:
| Parameter | Criterion for Exudate | Sensitivity |
|---|---|---|
| Pleural fluid protein / Serum protein | > 0.5 | ~98% |
| Pleural fluid LDH / Serum LDH | > 0.6 | ~98% |
| Pleural fluid LDH | > two-thirds the upper limit of normal serum LDH | ~98% |
Common Causes by Category
- Congestive heart failure (most common)
- Hepatic hydrothorax (cirrhosis)
- Nephrotic syndrome
- Myxoedema
- Pulmonary embolism (can be either)
- Peritoneal dialysis
- Parapneumonic / Empyema
- Malignancy
- Tuberculosis
- Pulmonary embolism
- Rheumatoid arthritis / SLE
- Pancreatitis
- Post-cardiac injury syndrome
- Chylothorax
Diagnostic Thoracentesis — Technique & Safety
Thoracentesis should be performed under ultrasound guidance (MBS item 55066 for ultrasound guidance) in all cases where feasible. Key procedural points:
- Patient positioning: sitting upright, leaning forward over a pillow on a bedside table, or side-lying with the affected side up.
- Site selection: identify the largest pocket of fluid on ultrasound, typically in the posterior triangle (between the diaphragm, vertebral column, and a vertical line through the posterior axillary fold). Avoid the 9th intercostal space posteriorly to prevent subdiaphragmatic or splenic/hepatic injury.
- Needle: 21-gauge butterfly needle or spinal needle for diagnostic aspiration; larger bore if therapeutic drainage planned.
- Maximum drainage: up to 1.5 L can be safely removed in a single therapeutic aspiration if the patient remains asymptomatic — monitor for re-expansion pulmonary oedema (rare but serious).
- Coagulopathy: correct INR < 2.0 and platelets > 50 × 10⁹/L where possible; however, thoracentesis can proceed with caution if correction is not possible and the benefit outweighs risk (BTS guidelines).
Pleural Fluid Analysis — Initial Panel
| Test | Diagnostic Clue |
|---|---|
| Protein, LDH (paired serum levels) | Light's criteria — exudate vs transudate |
| pH (heparinised syringe, on ice, analysed within 1 hour) | pH < 7.2 suggests complicated parapneumonic effusion, empyema, oesophageal rupture, rheumatoid effusion |
| Glucose (paired serum) | Low glucose (< 3.3 mmol/L) — empyema, rheumatoid, malignancy, TB, oesophageal rupture |
| Cell count & differential | Neutrophils → acute process; lymphocytes → TB, malignancy; eosinophils (> 10%) → air/blood in pleural space, drug reaction |
| Gram stain & culture (aerobic + anaerobic) | Positive in ~40% of parapneumonic effusions; send in blood culture bottles to improve yield |
| Cytology (≥ 3 samples on separate days improve sensitivity) | Malignant cells — sensitivity ~60% for a single sample (up to ~80% with three samples) |
| Triglycerides, cholesterol | Chylothorax if triglycerides > 1.24 mmol/L (or cholesterol > 5.18 mmol/L for pseudochylothorax) |
| Adenosine deaminase (ADA) | Elevated (> 40 U/L) suggestive of TB effusion (sensitivity ~90%, specificity ~90% in lymphocytic exudates) |
| Amylase | Elevated in pancreatitis, oesophageal rupture, malignancy |
Imaging
Parapneumonic Effusion & Empyema
Pathogenesis & Staging
Parapneumonic effusions develop in 20–40% of bacterial pneumonias, and approximately 5–10% of these progress to empyema. The natural history progresses through three stages, each with distinct management implications:
Indications for Chest Tube Drainage
- Frank pus on thoracentesis (empyema)
- Pleural fluid pH < 7.2
- Pleural fluid glucose < 3.3 mmol/L
- Positive Gram stain or culture of pleural fluid
- Loculated effusion
- Failure to improve on appropriate antibiotics after 48–72 hours
Chest Tube Placement
Intercostal catheter (ICC) insertion should be performed under ultrasound guidance. A small-bore catheter (10–14 French) is adequate for most parapneumonic effusions and is associated with less pain and equivalent efficacy to large-bore tubes. MBS item 18260 (intercostal catheter insertion).
Intrapleural Fibrinolytics — MIST-2 Regimen
The landmark MIST-2 trial (Rahman et al., NEJM 2011) demonstrated that combined alteplase + DNase significantly reduced pleural opacity, surgical referral, and hospital stay in patients with pleural infection. The standard regimen is:
VATS Indications
- Failure of chest tube drainage + intrapleural fibrinolytics (persistent sepsis, residual effusion at 72 hours)
- Complex multiloculated empyema not amenable to percutaneous drainage
- Organised empyema with thick pleural peel restricting lung expansion
- Persistent air leak (> 5 days) from underlying cavitary pneumonia or bronchopleural fistula
- Open thoracotomy and decortication if VATS is not feasible or fails
Antibiotic Selection for Parapneumonic Effusion / Empyema
Empirical antibiotic therapy should cover typical community-acquired pneumonia organisms and anaerobes. In Australia, the following regimens are recommended (aligned with eTG Antibiotic guidelines):
Malignant Pleural Effusion
Epidemiology & Aetiology
Malignant pleural effusion (MPE) affects approximately 50,000 Australians annually and represents an advanced-stage manifestation of malignancy. In Australia, the most common primary malignancies causing MPE are:
- Lung cancer (~35%)
- Breast cancer (~25%)
- Lymphoma (~10%)
- Mesothelioma (~10%) — disproportionately high in Australia
- Gastrointestinal, genitourinary, and ovarian cancers (remaining cases)
Diagnostic Approach
Management of MPE
Management is guided by symptom burden, expected survival, lung re-expandability, and patient preference. All patients with MPE should be offered palliative care involvement early.
Options for Recurrent MPE
| Intervention | Indication | Success Rate | Key Considerations |
|---|---|---|---|
| Talc pleurodesis | Recurrent symptomatic MPE; lung fully re-expandable; expected survival > 3 months | 80–90% | Talc slurry via ICC or talc poudrage via pleuroscopy/VATS. Requires inpatient stay (3–5 days). MBS item 18370. |
| Indwelling pleural catheter (IPC) | Recurrent MPE (including trapped lung); patient preference for ambulatory management | ~95% symptom control | Outpatient insertion under local anaesthesia. Spontaneous pleurodesis occurs in ~45% over weeks–months. Daily/intermittent drainage by patient or community nurse. MBS item 18371. |
| Serial thoracentesis | Poor performance status; very short expected survival; patient preference; interim measure | Temporary only | Re-accumulation within days–weeks; consider if other options declined |
Talc Pleurodesis — Procedure
Sterile asbestos-free talc (4–5 g in 50 mL 0.9% NaCl as slurry, or 2–5 g via poudrage) is instilled into the pleural space after complete fluid drainage. Pre-medicate with IV opioid (morphine 2.5–5 mg or fentanyl 25–50 μg) and consider intrapleural lignocaine (3 mg/kg, max 250 mg) 15 minutes before talc administration. Clamp ICC for 1–2 hours post-instillation, turning the patient every 15–20 minutes to distribute talc. Unclamp and connect to suction (–20 cmH₂O) until drainage < 150 mL/day.
Indwelling Pleural Catheter
The PleurX™ tunnelled catheter is the most commonly used IPC system in Australia. Inserted under local anaesthesia and ultrasound guidance in a day-procedure setting. The catheter is tunnelled subcutaneously to reduce infection risk. Patients or carers drain 500–1000 mL every 1–3 days using a vacuum bottle system. Community nursing support is essential — coordinate with the local District Nursing service. Monitor for catheter-related infection (cellulitis, empyema) and loculation (consider intrapleural fibrinolytics if drainage becomes difficult).
Palliative Management
All patients with MPE should have access to palliative care services. Breathlessness management includes:
- Low-dose opioids for breathlessness (modified-release morphine 5–10 mg PO BD, titrated; immediate-release morphine 2.5–5 mg PO PRN)
- Low-dose benzodiazepines if anxiety-related dyspnoea (diazepam 2–5 mg PO PRN)
- Supplemental oxygen if hypoxic (SpO₂ < 90%) — available via Home Oxygen Program in most Australian states
- Fan therapy and positioning advice
- Refer to community palliative care for home-based symptom management
Pneumothorax
Classification
- No underlying lung disease
- Typically tall, thin young males (15–34 years)
- Smoking increases risk ~20-fold
- Bullae/blisters at lung apices (CT)
- Mortality: very low
- Underlying lung disease (COPD most common; also CF, TB, lung cancer, PJP, bullous disease)
- Older patients (peak 60–70 years)
- Lower respiratory reserve — higher morbidity and mortality
- Mortality: up to 1–2% (higher in ventilated patients)
Size Assessment
Pneumothorax size is estimated on CXR by measuring the interpleural distance at the level of the hilum:
| Size (BTS Classification) | Measurement | Management Implications |
|---|---|---|
| Small | Rim of air < 2 cm between lung margin and chest wall at hilum level | PSP: may observe; SSP: may observe if asymptomatic and SpO₂ > 94% |
| Large | Rim of air ≥ 2 cm between lung margin and chest wall at hilum level | PSP: aspiration or ICC; SSP: usually ICC |
Management Algorithm — Primary Spontaneous Pneumothorax
Management Algorithm — Secondary Spontaneous Pneumothorax
- Small SSP, asymptomatic: Admit, supplemental O₂ (titrated to SpO₂ 88–92% in COPD), close monitoring, repeat CXR 2–4 hours. Most require ICC due to underlying lung disease.
- Large SSP or symptomatic: ICC insertion is first-line (aspiration has lower success rate in SSP ~30%). Small-bore (10–14F) via Seldinger technique under US guidance.
- Persistent air leak (> 5 days): Refer to thoracic surgery for VATS.
- First recurrence: Surgical pleurodesis recommended (chemical pleurodesis with doxycycline 500 mg or talc 2–4 g via ICC is an alternative if surgery is not feasible).
- Tension pneumothorax: Clinical diagnosis — immediate needle decompression (14G cannula, 2nd intercostal space, mid-clavicular line) followed by ICC. Do not delay for imaging.
Intercostal Catheter Removal
ICC can be removed when: (1) no air leak for ≥ 24 hours (bubbling ceased in underwater seal), (2) lung re-expanded on CXR, and (3) drainage < 200 mL/day (for effusions). Remove during expiration or Valsalva manoeuvre, with an occlusive dressing applied promptly. No clamping trial is needed for straightforward pneumothorax (BTS 2023 update).
Other Pleural Disorders
Haemothorax
Haemothorax is defined as pleural fluid with a haematocrit > 50% of the peripheral blood haematocrit. In Australia, the most common causes are trauma (penetrating and blunt), iatrogenic (post–central line insertion, post–lung biopsy, post–thoracic surgery), and spontaneous (coagulopathy, malignancy, aortic dissection).
- Initial management: large-bore ICC (28–32F) to drain blood and monitor ongoing losses.
- Massive haemothorax (> 1.5 L initial drainage or > 200 mL/hour for 2–4 hours): urgent surgical consultation — likely requires thoracotomy.
- Retained haemothorax (incomplete drainage): CT to assess. If > 1/3 hemithorax, consider VATS evacuation to prevent empyema and fibrothorax. Intrapleural fibrinolytics (alteplase 10 mg) may be used for retained clotted haemothorax as a bridge to surgery.
- Blood transfusion as per institutional massive transfusion protocol.
Chylothorax
Chylothorax results from disruption or obstruction of the thoracic duct, leading to chyle accumulation in the pleural space. Diagnosis requires pleural fluid triglycerides > 1.24 mmol/L (with lymphocyte-predominant cell count) or confirmation of chylomicrons on lipoprotein electrophoresis.
| Cause | Details | Management |
|---|---|---|
| Traumatic (most common) | Post-oesophagectomy (~5%), post-cardiac surgery, post-thoracic trauma | Conservative first: NPO/medium-chain triglyceride diet, ICC drainage, TPN if persistent (> 1 L/day × 5 days). Octreotide 50–100 μg SC TDS. Surgical thoracic duct ligation (VATS) if conservative management fails at 2 weeks. |
| Non-traumatic | Lymphoma (most common non-traumatic cause), metastatic malignancy, lymphangioleiomyomatosis (LAM), filariasis, congenital | Treat underlying cause. ICC drainage for symptom control. Consider thoracic duct embolisation (interventional radiology) or surgical ligation. Pleuroperitoneal shunt as last resort. |
Pleural Thickening
Diffuse pleural thickening (DPT) may follow empyema, haemothorax, tuberculous pleurisy, or asbestos exposure. It represents organised exudate and fibrin that has become incorporated into the visceral pleura, restricting lung expansion. DPT is distinguished from benign asbestos pleural plaques (which involve the parietal pleura and do not restrict lung function).
- DPT is significant if it causes > 25% volume loss or restrictive ventilatory defect on spirometry.
- CT is essential to distinguish thickening from effusion and to assess the extent of involvement.
- Decortication (VATS or open) may be considered in symptomatic patients with significant restrictive physiology and preserved underlying lung parenchyma.
- No effective medical therapy exists; pulmonary rehabilitation and breathlessness management are the mainstays of conservative treatment.
Asbestos-Related Pleural Disease
Australia's extensive history of asbestos use (until a nationwide ban in December 2003) means that asbestos-related pleural disease remains a significant clinical and medicolegal issue. The latency period from first exposure to disease manifestation is typically 20–40 years.
| Condition | Features | Management |
|---|---|---|
| Bilateral pleural plaques | Most common manifestation (up to 50% of exposed individuals). Calcified or non-calcified, parietal pleura, diaphragmatic, typically bilateral. No significant functional impairment. Marker of exposure, not premalignant. | No treatment required. Surveillance for mesothemioma not recommended (low sensitivity of screening). Patient education about asbestos exposure history. Notify state/territory occupational health authority (SafeWork). Medicolegal referral if relevant. |
| Diffuse pleural thickening | Extensive visceral pleural fibrosis causing restrictive physiology. Usually follows asbestos-related pleural effusion. Can be unilateral or bilateral. | Functional assessment (spirometry, 6MWT). Pulmonary rehabilitation. Decortication in select cases with significant restriction. Medicolegal assessment. |
| Asbestos-related pleural effusion | Exudative, typically unilateral, occurring within 10–20 years of exposure. Usually self-limiting. Exclusion of mesothelioma is critical. | Thoracentesis with cytology and mesothelioma markers (calretinin, WT-1, CK5/6). CT with contrast. Pleuroscopy/biopsy if diagnosis uncertain. Monitor for development of DPT. |
| Malignant mesothelioma | Aggressive malignancy of pleural mesothelial cells. Median survival 12–18 months. ~700–800 new cases/year in Australia (world's highest incidence). Most commonly epithelioid subtype (better prognosis). | Multidisciplinary management: chemotherapy (pemetrexed + cisplatin/carboplatin — PBS authority required), immunotherapy (nivolumab + ipilimumab — PBS-listed for unresectable pleural mesothelioma), surgery (EPP or P/D in select early-stage cases), radiation. Palliative care from diagnosis. Refer to specialist mesothelioma centres. Asbestos Exposure Register (Asbestos Safety and Eradication Agency). Compensable disease — SafeWork notification and legal referral. |
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972;77(4):507–513.
- 2. Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection (MIST-2 trial). N Engl J Med. 2011;365(6):518–526.
- 3. Hooper CE, Welham SA, Maskell NA; British Thoracic Society Pleural Disease Guideline Group. British Thoracic Society pleural disease guideline 2023. Thorax. 2023;78(Suppl 1):s1–s42.
- 4. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ; BTS Pleural Disease Guideline Group. Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65(Suppl 2):ii32–ii40.
- 5. MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65(Suppl 2):ii18–ii31.
- 6. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 7. Australian Mesothelioma Registry (AMR). Mesothelioma in Australia 2023. Canberra: Safe Work Australia; 2023.
- 8. Davies HE, Davies RJO, Davies CW; BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65(Suppl 2):ii41–ii53.
- 9. Dicpinigaitis PV, Mehta DC. Malignant pleural effusion: diagnosis and management. Am J Respir Crit Care Med. 2022;205(4):382–396.
- 10. Baas P, Scherpereel A, Nowak AK, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743). N Engl J Med. 2021;384(3):210–221.
- 11. Royal Australian College of General Practitioners (RACGP). Management of Asbestos-Related Disease in General Practice. Melbourne: RACGP; 2020.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 13. RHDAustralia (Communicable Diseases Network Australia). Recommendations for the Prevention, Control and Public Health Management of Rheumatic Heart Disease in Australia. Darwin: RHDAustralia; 2023.
- 14. Bibby AC, Dorn P, Psallidas I, et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur Respir J. 2019;53(5):1802158.
- 15. Corcoran JP, Psallidas I, Wrightson JM, Hallifax RJ, Rahman NM. Pleural procedural ultrasound: a systematic review and meta-analysis. Thorax. 2017;72(11):1035–1043.
- 16. Australian Commission on Safety and Quality in Health Care (ACSQHC). Antimicrobial Stewardship in Australian Health Care. Sydney: ACSQHC; 2018.