📋 Key Information Summary
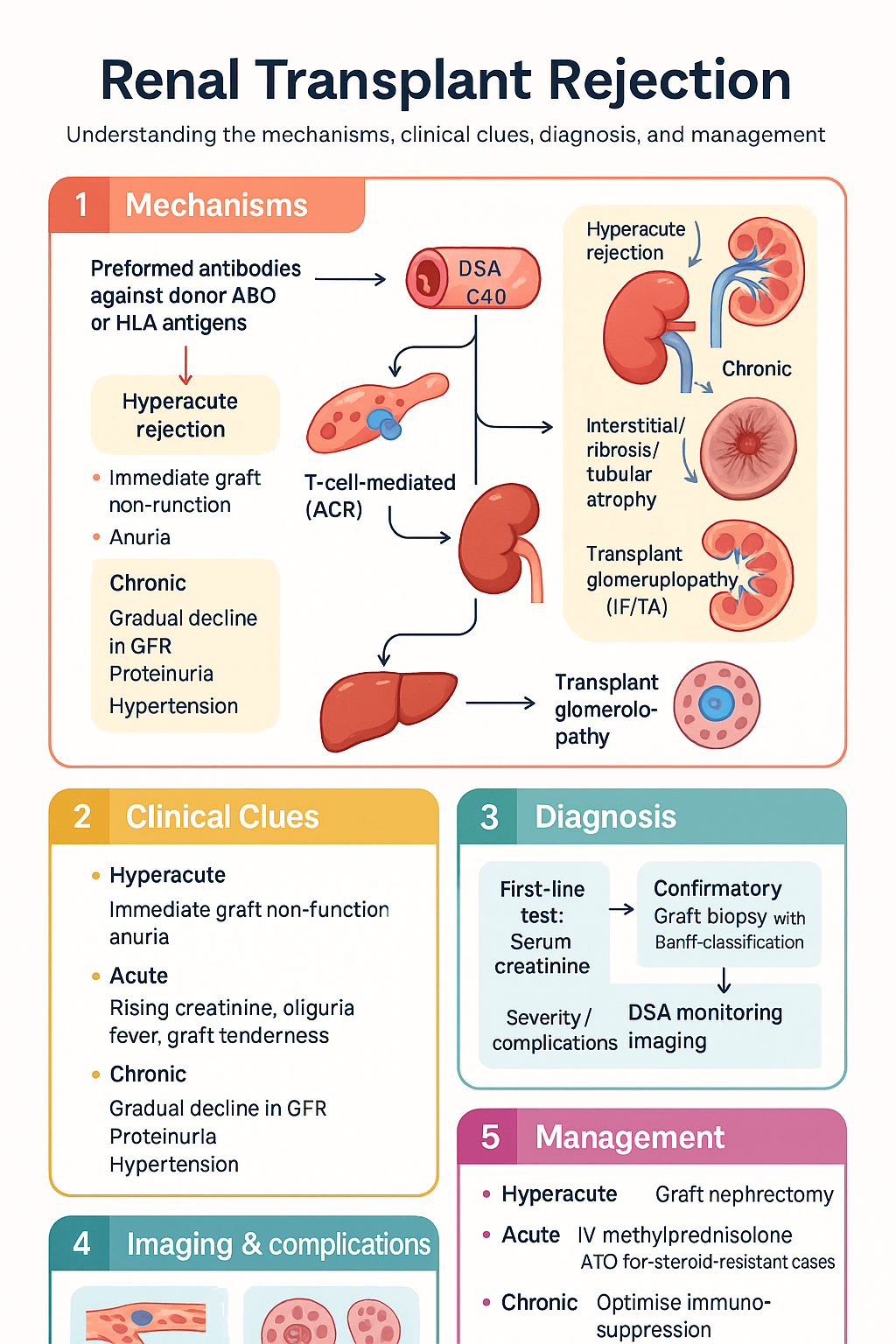
- Three temporal categories: Hyperacute (minutes–hours), Acute (days–months), Chronic (months–years); timely distinction is critical for graft survival.
- Hyperacute rejection occurs within minutes from preformed circulating antibodies against donor ABO or HLA antigens; graft loss is nearly universal and re-transplantation is usually required.
- Acute cellular rejection (ACR) is diagnosed by protocol or for-cause biopsy graded using the Banff 2019 classification (borderline changes, grades IA/IB/IIA/IIB/III).
- First-line treatment of ACR: IV methylprednisolone 500 mg daily for 3 days; steroid-resistant ACR warrants anti-thymocyte globulin (Thymoglobulin®).
- Antibody-mediated rejection (AMR) is defined by the Banff triad: donor-specific antibody (DSA) positivity, histological evidence of tissue injury (C4d, microvascular inflammation), and graft dysfunction.
- AMR first-line therapy: Plasma exchange + IVIg (2 g/kg); adjunctive rituximab and/or bortezomib for refractory cases.
- Protocol biopsies at 3, 6, and 12 months post-transplant detect subclinical rejection and improve long-term outcomes — recommended in Australian centres.
- DSA monitoring (Luminex single-antigen bead assay) should be performed pre-transplant, post-transplant at defined intervals, and with any graft dysfunction.
- Chronic allograft nephropathy involves interstitial fibrosis/tubular atrophy (IF/TA) and transplant glomerulopathy; management focuses on optimising immunosuppression and addressing modifiable risk factors.
- ATSI patients experience higher rates of end-stage kidney disease and longer wait times; culturally safe post-transplant follow-up and medication adherence support are essential.
- Drug interactions: Tacrolimus and ciclosporin are CYP3A4 substrates — avoid concurrent azole antifungals, grapefruit juice, and monitor for nephrotoxicity with all calcineurin inhibitors.
- TMA and BK virus nephropathy must be excluded before diagnosing persistent rejection, as treatment differs significantly.
Introduction & Australian Epidemiology
Renal allograft rejection remains the leading cause of early and late graft loss following kidney transplantation. Despite advances in immunosuppressive therapy, rejection episodes continue to affect approximately 15–25% of kidney transplant recipients in the first year post-transplant in Australia. Rejection is classified into three broad temporal categories — hyperacute, acute, and chronic — each with distinct immunological mechanisms, clinical presentations, and management strategies. Percutaneous graft biopsy with Banff classification remains the gold standard for diagnosis and guides therapeutic decisions.
In Australia, the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) reports that over 1,200 kidney transplants are performed annually, with living donor transplants accounting for approximately 40% of procedures. Acute rejection rates have declined to approximately 10–15% at 12 months with contemporary triple immunosuppression (tacrolimus, mycophenolate, prednisolone), but antibody-mediated rejection continues to be a major cause of late graft loss. The prevalence of chronic kidney disease is disproportionately high among Aboriginal and Torres Strait Islander peoples, and ensuring equitable access to transplantation and culturally safe post-transplant care remains a national priority.
This guideline provides a structured approach to the recognition, investigation, and management of renal transplant rejection, aligned with current Australian and international consensus frameworks including the Banff 2019 classification, Kidney Disease: Improving Global Outcomes (KDIGO) transplant guidelines, and the Transplantation Society of Australia and New Zealand (TSANZ) standards.
Hyperacute vs Acute vs Chronic Rejection
Understanding the temporal and immunological distinctions between rejection types is fundamental to appropriate management. Each category has different pathophysiological mechanisms, clinical trajectories, and therapeutic approaches.
| Feature | Hyperacute | Acute | Chronic |
|---|---|---|---|
| Timing | Minutes to hours | Days to 3–6 months (can occur later) | Months to years |
| Mechanism | Preformed antibodies (ABO or HLA); complement-mediated endothelial injury | T-cell mediated (ACR) or de novo DSA (AMR) | Chronic immune injury, ischaemia, nephrotoxicity, hypertension |
| Histology | Thrombotic microangiopathy, cortical necrosis | Tubulitis (ACR); C4d+, microvascular inflammation (AMR) | IF/TA (interstitial fibrosis/tubular atrophy), transplant glomerulopathy, vasculopathy |
| Clinical | Immediate graft non-function, anuria | Rising creatinine, oliguria, fever, graft tenderness | Gradual decline in GFR, proteinuria, hypertension |
| Treatment | Graft nephrectomy usually required | Steroids, ATG, plasma exchange, IVIg, rituximab | Optimise IS, treat modifiable factors, RAAS blockade |
| Graft outcome | Almost universal graft loss | Good if treated promptly; steroid-resistant worse | Progressive; 50% lose graft within 5 years of diagnosis |
Hyperacute Rejection
Hyperacute rejection results from preformed circulating antibodies directed against donor ABO blood group antigens or HLA class I molecules. These antibodies bind to donor endothelium upon reperfusion, activating complement and causing immediate thrombotic occlusion of the graft vasculature. In the modern era of routine pre-transplant crossmatching (complement-dependent cytotoxicity and virtual crossmatch by Luminex), hyperacute rejection has become exceedingly rare (<0.1%). It manifests as immediate graft non-function with cyanotic, mottled appearance of the kidney intraoperatively. Treatment is immediate graft nephrectomy. Prevention centres on rigorous ABO compatibility testing and HLA crossmatching prior to transplantation.
Acute Rejection
Acute rejection is the most clinically significant rejection type encountered in routine practice. It may be T-cell mediated (acute cellular rejection, ACR) or antibody-mediated (AMR), and both types can coexist (mixed rejection). The incidence of acute rejection in the first year post-transplant in Australia is approximately 10–15% with standard triple immunosuppression, with higher rates in sensitised patients, paediatric recipients, and those with poor adherence. Clinical suspicion is raised by a rise in serum creatinine of ≥20% above baseline, oliguria, or graft tenderness, but subclinical rejection — detected on protocol biopsy — occurs in up to 20–30% of stable patients.
Chronic Rejection
Chronic allograft dysfunction encompasses a spectrum of histological changes including interstitial fibrosis and tubular atrophy (IF/TA), transplant glomerulopathy (TG), and chronic transplant vasculopathy. It is now understood that both immune-mediated (subclinical rejection, de novo DSA) and non-immune-mediated (calcineurin inhibitor toxicity, hypertension, diabetes, BK virus nephropathy) factors contribute. Transplant glomerulopathy, characterised by double contours of the glomerular basement membrane on electron microscopy, is increasingly recognised as a manifestation of chronic AMR and is associated with particularly poor graft survival.
Acute Cellular Rejection: Banff Criteria & Treatment
The Banff classification, most recently updated in 2019, provides a standardised histopathological framework for grading allograft rejection. For acute cellular rejection (ACR), the classification focuses on tubulitis (t- and i-scores) and interstitial inflammation. Adequate biopsy sampling (≥7 glomeruli and ≥1 artery on light microscopy) is essential for accurate grading.
Banff 2019 — Acute Cellular Rejection Grading
Treatment of Acute Cellular Rejection
Antibody-Mediated Rejection (AMR) & DSA
Antibody-mediated rejection (AMR) accounts for approximately 30–40% of acute rejection episodes and is increasingly recognised as the dominant cause of chronic graft loss. The Banff 2019 criteria require three features for definitive AMR diagnosis: (1) circulating donor-specific antibody (DSA) or C4d positivity, (2) histological evidence of acute tissue injury (microvascular inflammation, acute thrombotic microangiopathy, or acute tubular injury in the absence of other causes), and (3) at least one of C4d positivity in peritubular capillaries or validated molecular evidence of endothelial injury.
Donor-Specific Antibodies (DSA)
DSA are antibodies directed against donor HLA antigens (class I: HLA-A, B, C; class II: HLA-DR, DQ, DP). De novo DSA — antibodies that develop post-transplant — are detected in 15–25% of recipients within 5 years and are associated with a 3–5-fold increased risk of graft loss. DSA characteristics that predict worse outcomes include:
- High mean fluorescence intensity (MFI): >5,000 on Luminex single-antigen bead assay
- Complement-fixing capacity: C1q-binding DSA
- IgG subclass: IgG1 and IgG3 are more pathogenic than IgG2/IgG4
- HLA class II (especially DQ) DSA: associated with worse chronic AMR outcomes
- Multiple DSA specificities and broad sensitisation (high panel reactive antibody, PRA)
Banff 2019 — AMR Classification
| Category | DSA / C4d | Histology | Clinical |
|---|---|---|---|
| Active AMR | DSA+ or C4d+ | Microvascular inflammation (g+ptc ≥2), TMA, acute tubular injury | Graft dysfunction (rising creatinine, proteinuria) |
| Chronic active AMR | DSA+ or C4d+ | Transplant glomerulopathy (cg >0), peritubular capillary basement membrane multilayering | Chronic graft dysfunction, proteinuria |
| C4d staining without evidence of rejection | C4d+ | No microvascular inflammation, no other injury | Stable graft function |
| Suspicious for AMR | DSA+ or C4d+ (only one criterion) | Microvascular inflammation without other cause | May be stable or dysfunctional |
DSA Monitoring Protocol (Australian Practice)
Management: Steroids, Thymoglobulin, IVIG, Rituximab
Management of renal transplant rejection is guided by the type (cellular vs antibody-mediated), severity (Banff grade), and response to initial therapy. A stepwise approach with escalation for refractory cases is recommended. The following pharmacological agents form the core of rejection treatment in Australian transplant centres.
AMR Treatment Protocol
Maintenance Immunosuppression Optimisation During Rejection
In addition to pulse or depleting therapies, maintenance immunosuppression should be reviewed and optimised during any rejection episode:
- Tacrolimus: Target trough 8–12 ng/mL during active rejection; reduce to 5–8 ng/mL once resolved.
- Mycophenolate mofetil: Increase to maximum tolerated dose (1 g BD for adults; 600 mg/m² BD for paediatrics) if not already maximised.
- Prednisolone: After pulse methylprednisolone, continue oral prednisolone 20–25 mg/day and taper over 4–6 weeks to maintenance dose (5–7.5 mg/day).
- Adherence assessment: Non-adherence is implicated in 20–30% of late rejection episodes. Use validated tools (BAASIS scale) and consider electronic pill monitoring.
Quick Reference: Rejection Treatment
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience end-stage kidney disease (ESKD) at rates 6–8 times higher than non-Indigenous Australians, with the highest burden in remote and very remote communities. Despite this, transplant rates remain lower and wait times longer for Indigenous Australians. Addressing barriers to transplantation and ensuring culturally safe, equitable post-transplant care — including rejection surveillance and management — is a national health priority.
📚 References
- 1. Loupy A, Haas M, Roufosse C, et al. The Banff 2019 Kidney Meeting Report: an update on classification of kidney disease pathology and potential biomarkers. Transplantation. 2020;104(10):2048–2068.
- 2. KDIGO Clinical Practice Guideline on the Evaluation and Management of Candidates for Kidney Transplantation. Transplantation. 2020;104(4S1):S1–S103.
- 3. Transplantation Society of Australia and New Zealand (TSANZ). Clinical Guidelines for Organ Transplantation from Deceased Donors. Version 1.5. 2021.
- 4. Clayton PA, McDonald SP, Russ GR, Chadban SJ. Long-term outcomes after acute rejection in kidney transplant recipients: an ANZDATA analysis. J Am Soc Nephrol. 2019;30(9):1697–1707.
- 5. Wiebe C, Gibson IW, Blydt-Hansen TD, et al. Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am J Transplant. 2012;12(5):1157–1167.
- 6. Roberts DM, Jiang SH, Chadban SJ. The treatment of acute antibody-mediated rejection in kidney transplant recipients — a systematic review. Transplantation. 2012;94(8):775–783.
- 7. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 217. Canberra: AIHW; 2023.
- 8. Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). 46th Annual Report 2023 (Data to 2022). Adelaide, South Australia.
- 9. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th Edition. Melbourne: Kidney Health Australia; 2020.
- 10. National Aboriginal Community Controlled Health Organisation (NACCHO). Cultural safety in health care — framework. Canberra: NACCHO; 2022.
- 11. Haas M, Sis B, Racusen LC, et al. Banff 2013 meeting report: inclusion of C4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am J Transplant. 2014;14(2):272–283.
- 12. Schinstock CA, Mannon RB, Budde K, et al. Recommended treatment for antibody-mediated rejection after kidney transplantation: the 2019 expert consensus from the Transplantion Society Working Group. Transplantation. 2020;104(5):911–922.
- 13. Gallagher MP, Kelly PJ, Jardine M, et al. Long-term cancer risk of immunosuppressive regimens after kidney transplantation. J Am Soc Nephrol. 2010;21(5):852–858.
- 14. Grace S, Clayton P, McDonald SP. Increases in renal replacement therapy in Australia and New Zealand: understanding trends in Indigenous and non-Indigenous incidence. Nephrology. 2012;17(1):37–45.