📋 Key Information Summary
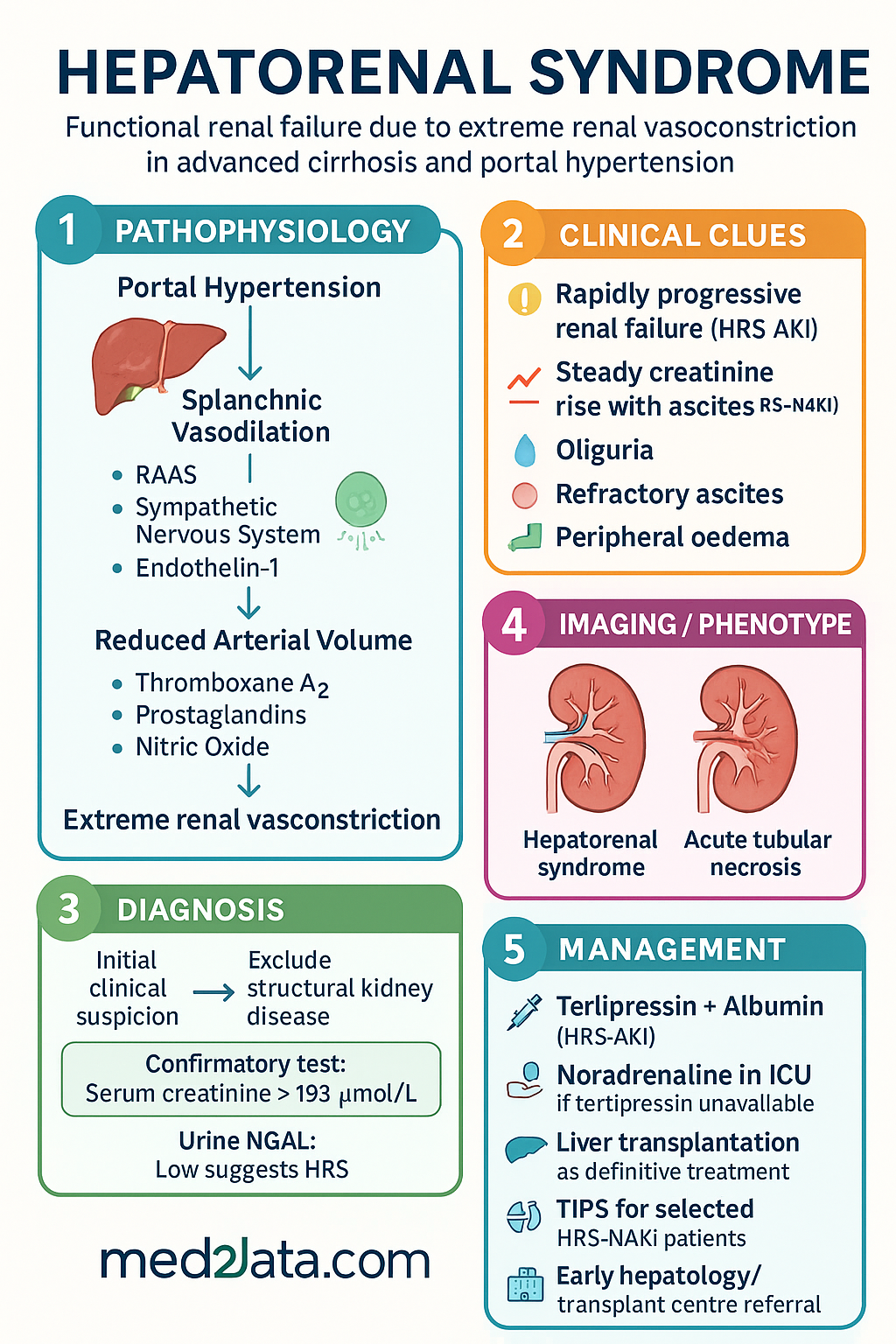
- Hepatorenal syndrome (HRS) is a diagnosis of exclusion, representing functional renal failure due to extreme renal vasoconstriction in patients with advanced cirrhosis and portal hypertension.
- HRS Type 1 (now HRS-AKI) is rapidly progressive, defined by a doubling of serum creatinine to >265 µmol/L in <2 weeks, and carries a very high mortality without intervention.
- HRS Type 2 (now HRS-NAKI) is characterised by a steady, moderate rise in creatinine (often with diuretic-resistant ascites) and has a more indolent course.
- Key pathophysiology involves splanchnic vasodilation, reduced effective circulating volume, and activation of the RAAS and sympathetic nervous system, causing intense renal vasoconstriction.
- Diagnosis requires ruling out structural kidney disease, shock, nephrotoxic drugs, and intravascular volume depletion. Urine biomarkers (e.g., NGAL) may aid differentiation.
- First-line pharmacotherapy for HRS-AKI is terlipressin (IV) + albumin (IV). This is PBS Authority Required in Australia.
- Noradrenaline (IV) in an ICU setting is an alternative vasopressor if terlipressin is unavailable or contraindicated.
- Albumin is critical for volume expansion and is co-administered with vasopressors; its use in HRS-NAKI is less defined.
- Liver transplantation is the definitive treatment and only curative option for both types of HRS.
- Transjugular intrahepatic portosystemic shunt (TIPS) may be considered for selected patients with HRS-NAKI to reduce portal pressure.
- Renal replacement therapy (RRT) is a bridge to transplantation or recovery in HRS-AKI but does not improve long-term survival alone.
- Aboriginal and Torres Strait Islander peoples experience a higher burden of liver disease and may face barriers to timely specialist care and transplantation assessment.
- All management decisions should involve early consultation with a hepatology/transplant centre.
Introduction & Australian Epidemiology
Hepatorenal syndrome (HRS) is a life-threatening complication of advanced liver disease, defined as functional renal failure in the absence of structural kidney pathology. It arises from profound alterations in systemic and renal haemodynamics driven by portal hypertension. HRS is a diagnosis of exclusion, with a pathognomonic feature of intense renal vasoconstriction.
In Australia, HRS complicates approximately 10–20% of hospitalisations for decompensated cirrhosis. The mortality rate for untreated HRS Type 1 (HRS-AKI) exceeds 80% within two weeks. While nationwide incidence data is limited, the burden aligns with rising rates of alcohol-related liver disease and metabolic dysfunction-associated steatohepatitis (MASH). Aboriginal and Torres Strait Islander peoples experience a disproportionately higher incidence of severe liver disease, which may contribute to a greater relative risk of HRS.
Pathophysiology
Renal Vasoconstriction & Haemodynamic Changes
The primary driver is portal hypertension, leading to splanchnic and systemic arterial vasodilation. This reduces effective arterial blood volume (underfilling theory) and triggers a compensatory homeostatic response:
- Renin-Angiotensin-Aldosterone System (RAAS) Activation: Reduced renal perfusion pressure stimulates renin release, increasing angiotensin II and aldosterone. This causes efferent arteriolar vasoconstriction and sodium/water retention, but fails to restore systemic perfusion.
- Sympathetic Nervous System (SNS) Activation: Further renal vasoconstriction and sodium retention.
- Imbalance of Renal Vasoactive Substances: An increase in vasoconstrictors (endothelin-1, thromboxane A2) and a decrease in vasodilators (prostaglandins, nitric oxide) within the renal circulation.
The net result is a critical reduction in renal blood flow and glomerular filtration rate (GFR), while the kidneys themselves remain structurally intact and capable of function if normal perfusion is restored.
HRS Type 1 vs Type 2
Historically classified as Type 1 and Type 2, the International Ascites Club now recommends terminology aligning with acute kidney injury (AKI) stages, though the classic types remain clinically descriptive.
| Feature | HRS Type 1 (HRS-AKI) | HRS Type 2 (HRS-NAKI) |
|---|---|---|
| Clinical Course | Rapidly progressive, often triggered by infection (e.g., SBP), GI bleeding, or large-volume paracentesis without albumin. | Slowly progressive, steady decline in renal function over weeks to months. |
| Serum Creatinine | Doubles to >265 µmol/L within 2 weeks. Often a swift rise. | Elevated (usually 133–265 µmol/L), but relatively stable. |
| Key Presentation | Acute decompensation of cirrhosis; oliguria; rapid development of refractory ascites. | Typically presents with diuretic-resistant or refractory ascites. Peripheral oedema common. |
| Prognosis | Median survival without treatment: 2–4 weeks. | Median survival: 3–6 months. |
| Primary Goal of Treatment | Reverse AKI with vasopressors as a bridge to liver transplant. | Manage ascites, consider TIPS, and prioritise for liver transplant. |
Investigations & Diagnosis (Exclusion Criteria)
Diagnosis is based on the revised International Ascites Club criteria and is primarily one of exclusion.
Diagnostic Criteria
- Cirrhosis with ascites.
- Serum creatinine >133 µmol/L (for HRS-AKI: a rise of ≥26.5 µmol/L in 48h or ≥50% from baseline within 7 days).
- No improvement of creatinine after at least 2 days of diuretic withdrawal and volume expansion with albumin (1g/kg/day, max 100g/day).
- Absence of shock.
- No current or recent treatment with nephrotoxic drugs (NSAIDs, aminoglycosides, IV contrast).
- No structural kidney disease: absence of proteinuria >500 mg/day, no microhaematuria (>50 RBCs/HPF), and normal renal ultrasound.
Key Investigations
Management
Management aims to reverse renal dysfunction as a bridge to liver transplantation, the only curative therapy. All patients require immediate referral to a hepatology/transplant centre.
1. General & Supportive Measures
- Admit to high-dependency or ICU setting for HRS-AKI.
- Stop all nephrotoxins (NSAIDs, aminoglycosides).
- Volume expansion: Intravenous albumin 1g/kg (max 100g) on day 1, then 20–40g/day. Monitor for pulmonary oedema.
- Treat precipitating factors: Active infection (e.g., SBP with IV cefotaxime or ceftriaxone), GI bleeding.
2. Pharmacotherapy (Vasoconstrictors + Albumin)
Alternative Vasopressor: Noradrenaline
Noradrenaline (Levophed®) is a valid alternative, particularly if terlipressin is unavailable or contraindicated (e.g., severe coronary artery disease). It requires continuous infusion in an ICU setting.
3. Definitive Therapy: Liver Transplantation
Liver transplant assessment must be initiated immediately upon diagnosis. Renal function often recovers post-transplant. HRS is a strong indication for transplant listing, and wait-listing strategies (e.g., simultaneous liver-kidney transplant criteria) are complex and centre-specific.
4. Other Therapies
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): Can improve renal function in selected patients with HRS-NAKI (Type 2). Requires assessment of liver function (MELD <11-12), no encephalopathy, and patent portal vein. Not a first-line therapy for HRS-AKI.
- Renal Replacement Therapy (RRT): Used as a bridge for transplant candidates with severe uraemia, acidosis, or fluid overload unresponsive to diuretics. Does not alter the natural history of HRS.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of liver disease, often at a younger age, driven by higher rates of hepatitis B and C, alcohol-related harm, and metabolic syndrome. This leads to a greater risk of developing cirrhosis and its complications, including HRS.
📚 References
- 1. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatic encephalopathy. J Hepatol. 2022.
- 2. Angeli P, Ginès P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol. 2015;62(4):968-974.
- 3. Wong F, Pappas SC, Curry MP, et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N Engl J Med. 2021;384(9):818-828.
- 4. Boyer TD, Sanyal AJ, Wong F, et al. Terlipressin plus albumin is more effective than albumin alone in improving renal function in patients with cirrhosis and hepatorenal syndrome type 1. Gastroenterology. 2016;150(4):945-955.
- 5. Australian Institute of Health and Welfare (AIHW). Liver and biliary cancer in Australia. Cat. no. CAN 126. Canberra: AIHW; 2021.
- 6. RHDAustralia (a program of NACCHO). Australian Aboriginal and Torres Strait Islander Health InfoNet. Various publications on chronic disease burden.
- 7. Pharmaceuticals Benefits Scheme (PBS). Terlipressin (Authority Required) and Albumin (Restricted Benefit) indications. Australian Government Department of Health.
- 8. Nadim MK, Kellum JA, Davenport A, et al. Hepatorenal syndrome: the 8th International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2012;16(1):R23.
- 9. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book), 9th edn. 2016.
- 10. Fagiuoli S, Colli A, Bruno R, et al. Management of infections in patients with cirrhosis. Lancet Gastroenterol Hepatol. 2021;6(4):318-330.