📋 Key Information Summary
- Anaemia affects 40–60% of CKD patients (eGFR <60 mL/min/1.73 m²) and is nearly universal by CKD stage 5; predominantly normocytic normochromic.
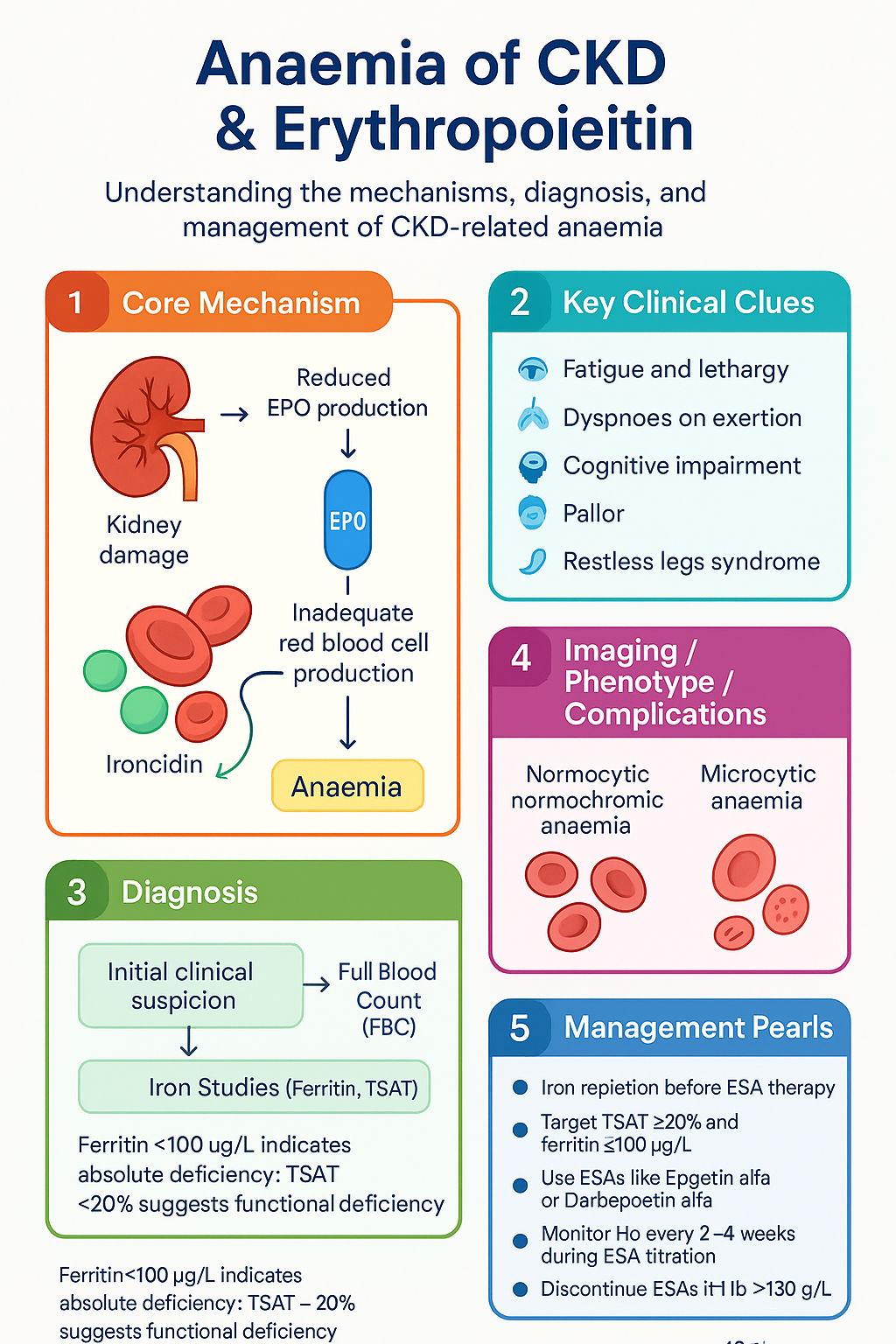
- The primary driver is relative erythropoietin (EPO) deficiency — the kidney fails to upregulate EPO proportionally to the degree of anaemia.
- Functional iron deficiency (iron-restricted erythropoiesis) is the second major mechanism: ferritin may be normal or high yet transferrin saturation (TSAT) is low, limiting iron availability for red cell production.
- Investigate all CKD patients with Hb <110 g/L (women) or <120 g/L (men) — rule out non-renal causes including GI bleeding, nutritional deficiency, and haematological malignancy before attributing anaemia solely to CKD.
- Iron repletion should be initiated BEFORE or alongside ESA therapy; target TSAT ≥20% and ferritin ≥100 µg/L (non-dialysis) or ≥200 µg/L (dialysis).
- First-line ESAs in Australia: Epoetin alfa (Eprex®) or Darbepoetin alfa (Aranesp®), both PBS-listed for CKD-related anaemia with authority requirements.
- Haemoglobin target: 100–115 g/L; do NOT exceed 130 g/L — meta-analyses show increased stroke, thrombosis, and mortality with higher targets.
- IV iron (ferric carboxymaltose, iron polymaltose) is preferred in haemodialysis patients; oral iron is suitable in non-dialysis CKD with mild iron deficiency.
- Monitor Hb every 2–4 weeks during ESA dose titration; every 1–3 months when stable. Check iron indices (ferritin, TSAT) every 3 months.
- HIF-PH inhibitors (roxadustat) are now PBS-listed for CKD anaemia and provide an oral alternative for patients with functional iron deficiency — reviewed separately.
- Discontinue ESAs if Hb exceeds 130 g/L or if uncontrolled hypertension, pure red cell aplasia (PRCA) with anti-EPO antibodies, or active malignancy is diagnosed.
- Aboriginal and Torres Strait Islander peoples experience CKD at 2–4× the rate of non-Indigenous Australians; earlier screening for anaemia and iron deficiency is essential.
Introduction & Australian Epidemiology
Anaemia is one of the most prevalent and consequential complications of chronic kidney disease (CKD), contributing to fatigue, reduced exercise tolerance, left ventricular hypertrophy, cognitive impairment, and increased cardiovascular mortality. It is driven primarily by reduced erythropoietin (EPO) production from the diseased kidney, compounded by iron deficiency, chronic inflammation, uraemic toxin-mediated red cell destruction, and shortened red blood cell survival.
In Australia, CKD affects approximately 1 in 10 adults (AIHW 2023), and anaemia prevalence rises steeply with declining eGFR: roughly 15% at CKD stage 3a, 40% at stage 4, and over 80–90% in patients on dialysis (eGFR Study, McMahon et al.). The economic burden is significant, with ESA and intravenous iron therapies representing major PBS expenditure — over 0 million annually.
Management centres on two pillars: (1) iron repletion to correct absolute or functional iron deficiency, and (2) erythropoiesis-stimulating agents (ESAs) to replace the relative EPO deficiency. Appropriate target-setting, vigilant monitoring, and awareness of ESA-related risks are essential to optimise outcomes while minimising harm.
Pathophysiology: EPO Deficiency & Iron-Restricted Erythropoiesis
Erythropoietin Deficiency
Erythropoietin is a 34-kDa glycoprotein produced predominantly by peritubular interstitial fibroblasts in the renal cortex and outer medulla. Hypoxia-inducible factor 2α (HIF-2α) drives EPO transcription in response to tissue hypoxia. In CKD, progressive tubulointerstitial fibrosis replaces EPO-producing fibrocytes, resulting in a blunted EPO response: serum EPO levels may be in the "normal" range (8–30 mU/mL) but are inappropriately low for the degree of anaemia (expected >50–100 mU/mL).
This relative deficiency manifests from CKD stage 3 onwards and worsens linearly. Unlike anaemia from other causes, patients with CKD anaemia rarely mount an adequate reticulocyte response.
Iron-Restricted Erythropoiesis
Iron restriction in CKD is multifactorial and frequently functional (adequate total body iron but insufficient available iron for erythropoiesis):
- Absolute iron deficiency: GI blood loss (angiodysplasia, NSAID use, uraemic gastropathy), dietary inadequacy, phlebotomy losses in haemodialysis (50–100 mL blood/week).
- Functional iron deficiency: Hepcidin excess — the key mediator. CKD-driven inflammation elevates IL-6, which upregulates hepcidin (a 25-amino-acid peptide). Hepcidin binds ferroportin on enterocytes and macrophages, causing its internalisation and degradation, thereby trapping iron intracellularly and blocking intestinal absorption and macrophage iron recycling.
- Iron utilisation impaired: Even when TSAT is nominally adequate (≥20%), the inflammatory milieu may impair iron delivery to erythroid precursors.
Other Contributing Mechanisms
- Uraemic toxin-mediated inhibition of erythroid progenitor proliferation
- Shortened RBC survival (from ~120 days to ~60–90 days in advanced CKD)
- Folate and vitamin B₁₂ losses in dialysate
- Chronic inflammation suppressing erythropoiesis via TNF-α, IL-1, IFN-γ
- Aluminium toxicity (historically from phosphate binders; now rare in Australia)
- Hyperparathyroidism — secondary hyperparathyroidism with marrow fibrosis
Clinical Presentation & Diagnostic Criteria
WHO Definitions of Anaemia
| Population | Hb Threshold (g/L) |
|---|---|
| Non-pregnant women (≥15 years) | <120 g/L |
| Men (≥15 years) | <130 g/L |
| Pregnant women | <110 g/L |
| Children 12–14 years | <120 g/L |
| Children 5–11 years | <115 g/L |
| Children 6 months – 4 years | <110 g/L |
Symptoms & Signs
CKD-related anaemia is typically insidious. Patients may present with:
- Fatigue, lethargy, and reduced exercise capacity (most common)
- Dyspnoea on exertion
- Cognitive impairment and poor concentration
- Pallor (conjunctival, palmar)
- Angina or worsening heart failure (in patients with pre-existing CVD)
- Restless legs syndrome
- Cold intolerance
Symptoms often correlate poorly with Hb level; some patients are symptomatic at Hb 100 g/L while others are asymptomatic at 80 g/L. Quality-of-life tools (KDQoL, SF-36) help quantify symptom burden.
When to Suspect CKD Anaemia
- Any patient with eGFR <60 mL/min/1.73 m² and normocytic normochromic anaemia
- Rising Hb (>10 g/L drop) between visits in known CKD
- Persistent anaemia despite iron supplementation — consider functional iron deficiency, ESA-naïve, or non-renal cause
Investigations & Iron Indices
Baseline Workup for Anaemia in CKD
Before attributing anaemia to CKD, perform the following investigations:
Iron Status Interpretation Guide
| Scenario | Ferritin | TSAT | Interpretation |
|---|---|---|---|
| Absolute iron deficiency | <100 µg/L | <20% | Severe depletion — replete aggressively |
| Functional iron deficiency | 100–500 µg/L | <20% | Iron sequestered by hepcidin — IV iron often needed |
| Iron replete (non-dialysis) | ≥100 µg/L | ≥20% | Adequate stores |
| Iron replete (dialysis) | ≥200 µg/L | ≥20% | Adequate for ESA optimisation |
| Iron overload risk | >500 µg/L | >50% | Withhold IV iron — monitor closely |
ESA Therapy: Epoetin Alfa & Darbepoetin Alfa
Erythropoiesis-stimulating agents (ESAs) remain the cornerstone pharmacotherapy for CKD-related anaemia after iron optimisation. Two agents are available on the PBS for CKD in Australia:
Intravenous Iron Preparations
Oral Iron
Oral iron (ferrous sulfate 325 mg [~65 mg elemental iron] PO daily or on alternate days) is suitable for non-dialysis CKD patients with mild absolute iron deficiency. Efficacy is limited by poor GI absorption (hepcidin-mediated in CKD), GI side effects, and poor adherence. Avoid taking concurrently with phosphate binders, calcium supplements, or proton pump inhibitors (reduce absorption).
Conversion: Epoetin → Darbepoetin
| Weekly Epoetin Dose (units/week) | Equivalent Darbepoetin Dose (µg/week) |
|---|---|
| 2,000 | 10 |
| 4,000 | 20 |
| 6,000 | 30 |
| 8,000 | 40 |
| 10,000 | 50 |
| 20,000 | 100 |
| 30,000 | 150 |
| 40,000 | 200 |
| 50,000 | 250 |
| 60,000 | 300 |
| 80,000 | 400 |
Dosing ratio approximately 200:1 (units epoetin : µg darbepoetin). Administer the first dose of darbepoetin at the time the next epoetin dose would have been due. Monitor Hb weekly for 4 weeks after conversion.
Iron Repletion Strategy
Iron should be repleted to target TSAT ≥20% and ferritin ≥100 µg/L (non-dialysis) or ≥200 µg/L (haemodialysis) BEFORE initiating an ESA. In many patients, correcting iron deficiency alone may raise Hb sufficiently to delay or avoid ESA therapy.
Iron Repletion Algorithm
Targets & Monitoring
Haemoglobin Targets
Monitoring Schedule
Iron Monitoring Parameters
| Parameter | Target (non-dialysis) | Target (dialysis) | Action if High |
|---|---|---|---|
| Ferritin | ≥100 µg/L | ≥200 µg/L | Hold IV iron if >500 µg/L; monitor if 200–500 |
| TSAT | ≥20% | ≥20% | Hold IV iron if >50% |
| RET-He (CHr) | ≥29 pg | ≥29 pg | If low despite TSAT ≥20%, suggest functional deficiency |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
ESA Hyporesponsiveness & Complications
ESA hyporesponsiveness is defined as failure to achieve target Hb despite an epoetin dose ≥300 units/kg/week (or darbepoetin ≥1.5 µg/kg/week) or progressive dose escalation to maintain target Hb.
Causes of ESA Hyporesponsiveness
| Category | Specific Causes | Investigation |
|---|---|---|
| Iron deficiency | Absolute or functional; erythropoiesis outstrips iron supply | Ferritin, TSAT, RET-He |
| Infection / inflammation | Chronic infections, access graft infections, SLE, vasculitis | CRP, ESR, blood cultures if febrile |
| Hyperparathyroidism | Bone marrow fibrosis suppresses erythropoiesis | PTH, calcium, phosphate, vitamin D |
| Chronic blood loss | GI angiodysplasia, menstruation, dialysis circuit | FOBT, GI endoscopy, stool Hb |
| Nutritional deficiency | B₁₂, folate — dialysate losses | Serum B₁₂, red cell folate |
| Malignancy | Myeloma, myelodysplasia, solid tumour marrow infiltration | Peripheral film, serum protein electrophoresis, bone marrow biopsy |
| PRCA | Anti-EPO neutralising antibodies (rare; associated with SC Eprex®) | Anti-EPO antibodies, reticulocyte count (<10 × 10⁹/L), bone marrow biopsy |
Management of ESA Hyporesponsiveness
- Correct all modifiable causes: replete iron, treat infection, manage hyperparathyroidism
- Consider IV iron course (ferric carboxymaltose 1000 mg) even if ferritin is mildly elevated but TSAT <20%
- If Hb continues to fall despite maximum ESA and adequate iron, consider transfusion support — but aim to minimise transfusion frequency (risk of HLA sensitisation in transplant candidates)
- Refer to nephrology/haematology for further workup
- HIF-PH inhibitors (roxadustat) may be considered for ESA-hyporesponsive patients — see separate guideline
Red Blood Cell Transfusion in CKD
Transfusion is reserved for symptomatic severe anaemia or when ESA/iron therapy is insufficient, contraindicated, or being initiated (bridge therapy).
- Consider transfusion if Hb <70 g/L with symptoms, or Hb <80 g/L with acute cardiovascular compromise
- Aim for Hb 80–100 g/L post-transfusion (single-unit strategy preferred — prescribe one unit and reassess)
- Leucodepleted, CMV-safe blood products standard in Australia (National Blood Authority)
- Iron overload risk with repeated transfusions — monitor ferritin (transfusion-related haemochromatosis threshold >1000 µg/L)
- HLA sensitisation is a concern in transplant-waitlisted patients — minimise transfusions
- Post-transfusion Hb expected increment: ~10 g/L per unit of packed RBCs (adult)
Quick Reference: CKD Anaemia Management
📚 References
- 1. Kidney Health Australia — Caring for Australasians and New Zealanders with Kidney Disease (KHA-CARI). CARI Guidelines: Anaemia in Chronic Kidney Disease. Melbourne: KHA; 2023.
- 2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3(1):1–150.
- 3. McMahon LP, Roger SD, Levin A; for the Slimbridge Study Group. Development, implementation, and audit of a clinical algorithm for the management of anaemia in CKD. Nephrology. 2004;9:113–120.
- 4. Pfeffer MA, Burdmann EA, Chen C-Y, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019–2032 (TREAT Trial).
- 5. Singh AK, Szczech L, Tang KL, et al. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med. 2006;355(20):2085–2098 (CHOIR Trial).
- 6. Drüeke TB, Locatelli F, Clyne N, et al. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med. 2006;355(20):2071–2084 (CREATE Trial).
- 7. Locatelli F, Bárány P, Covic A, et al. Kidney Disease: Improving Global Outcomes guidelines on anaemia management in chronic kidney disease: a European Renal Best Practice position statement. Nephrol Dial Transplant. 2013;28(6):1346–1359.
- 8. National Blood Authority Australia. National Patient Blood Management Guidelines — Module 6: Critical Care. Canberra: NBA; 2012 (updated 2023).
- 9. Macdougall IC, White C, Anker SD, et al. Intravenous iron in patients undergoing maintenance hemodialysis. N Engl J Med. 2019;380(5):447–458 (PIVOTAL Trial).
- 10. Australian Institute of Health and Welfare (AIHW). Chronic Kidney Disease in Aboriginal and Torres Strait Islander People. Cat. no. PHE 265. Canberra: AIHW; 2023.
- 11. Babitt JL, Lin HY. Mechanisms of anemia in CKD. J Am Soc Nephrol. 2012;23(10):1631–1634.
- 12. Besarab A, Bolton WK, Browne JK, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. 1998;339(9):584–590 (Normal Haematocrit Study).
- 13. Pharmaceutical Benefits Scheme (PBS). Epoetin alfa and Darbepoetin alfa — Authority Required Listings for CKD-Related Anaemia. Commonwealth of Australia; 2024. Available at: pbs.gov.au.
- 14. Casadevall N, Nataf J, Viron B, et al. Pure red-cell aplasia and antierythropoietin antibodies in patients treated with recombinant erythropoietin. N Engl J Med. 2002;346(7):469–475.