📋 Key Information Summary
- Pre-eclampsia complicates 5–8% of pregnancies in Australia and remains a leading cause of maternal and perinatal morbidity and mortality
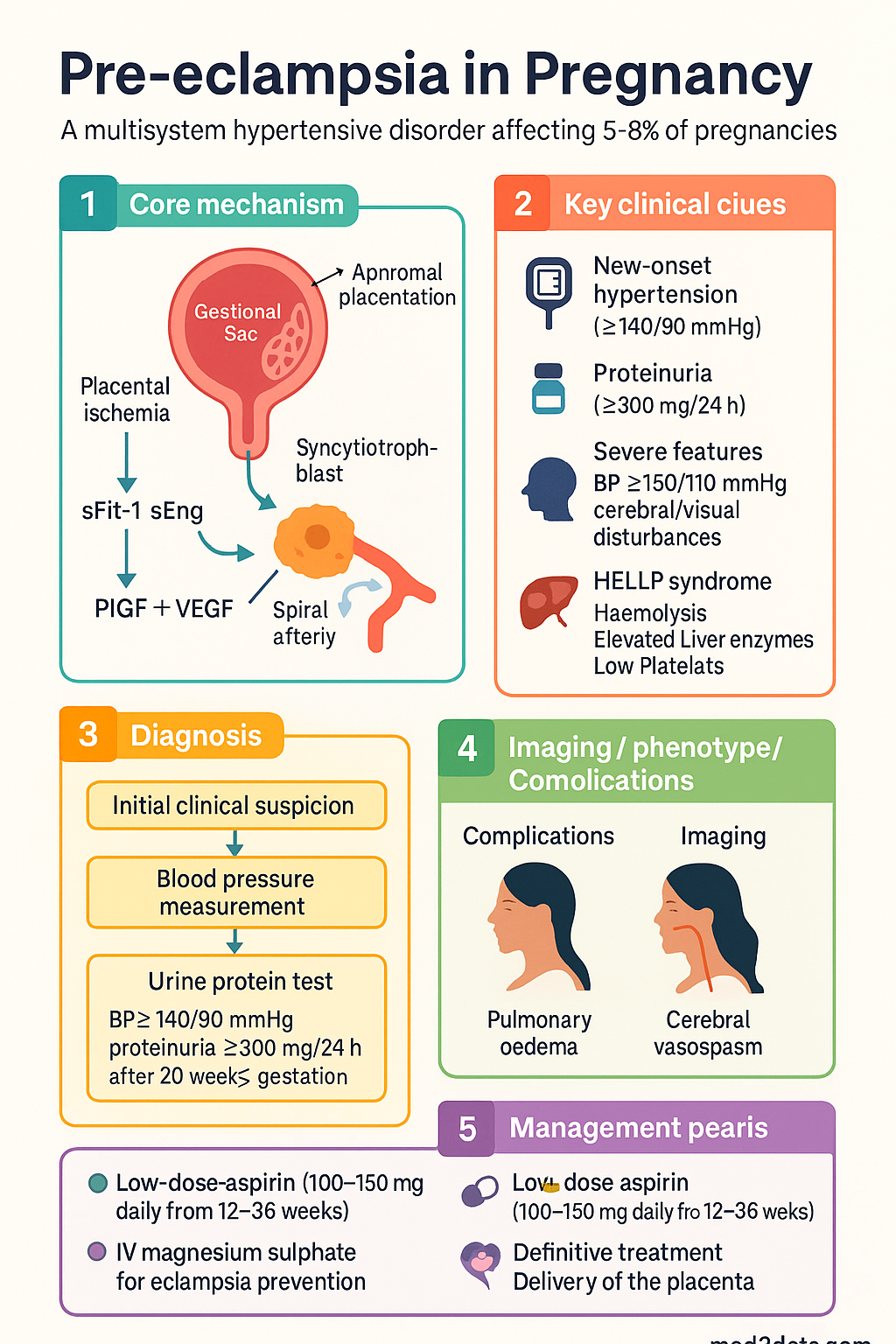
- Diagnosis requires new-onset hypertension (≥140/90 mmHg on two occasions ≥4 hours apart) plus proteinuria (≥300 mg/24 h or PCR ≥30 mg/mmol) after 20 weeks' gestation
- Renal physiological changes in normal pregnancy include a 50% rise in GFR, reduced serum creatinine (~45–70 µmol/L), and decreased uric acid due to enhanced tubular secretion
- Low-dose aspirin (100–150 mg daily from 12–36 weeks) reduces pre-eclampsia risk by ~60% in high-risk women; recommended by RANZCOG for risk-based prophylaxis
- Severe features include BP ≥160/110 mmHg, platelet count <100 × 10⁹/L, serum creatinine >90 µmol/L, LDH >600 U/L, pulmonary oedema, or new-onset cerebral/visual disturbances
- HELLP syndrome (Haemolysis, Elevated Liver enzymes, Low Platelets) is a severe variant occurring in 10–20% of pre-eclampsia cases, with significant maternal morbidity
- IV magnesium sulphate is first-line for eclampsia prevention and treatment (Sibai regimen: 4 g loading dose then 1–2 g/h infusion); available PBS General Benefit
- Labetalol (oral or IV) is the preferred antihypertensive; nifedipine slow-release oral and IV hydralazine are alternatives; target BP <140/90 mmHg
- Definitive treatment is delivery of the placenta; timing balances maternal severity against fetal maturity, guided by RANZCOG and SOMANZ guidelines
- Aboriginal and Torres Strait Islander women have higher rates of pre-eclampsia and hypertensive disorders, driven by chronic hypertension prevalence, remoteness barriers, and limited antenatal access
- Postpartum monitoring is essential as pre-eclampsia may develop or worsen up to 48–72 hours after delivery; 25% of eclampsia cases are postpartum
- Women with pre-eclampsia history have a 2–7× increased lifetime risk of cardiovascular disease; long-term cardiovascular risk reduction counselling is mandatory
Introduction & Australian Epidemiology
Pre-eclampsia is a multisystem hypertensive disorder of pregnancy affecting 5–8% of pregnancies worldwide, with similar prevalence reported in Australian population studies. It remains one of the leading causes of maternal mortality and morbidity in Australia, accounting for approximately 10–15% of direct maternal deaths as reported by the Australian Institute of Health and Welfare (AIHW) Maternal Deaths in Australia series. Pre-eclampsia is characterised by new-onset hypertension with proteinuria developing after 20 weeks' gestation, and may progress to eclampsia (seizures), HELLP syndrome, stroke, hepatic rupture, renal failure, or placental abruption.
The hypertensive disorders of pregnancy are classified by the Society of Obstetric Medicine of Australia and New Zealand (SOMANZ) into four categories: gestational hypertension, pre-eclampsia (new-onset or superimposed on chronic hypertension), chronic hypertension, and eclampsia. Pre-eclampsia can be further stratified into early-onset (<34 weeks) and late-onset (≥34 weeks), with early-onset disease carrying higher maternal and perinatal risks and a greater association with placental insufficiency.
Renal involvement is central to the pathophysiology of pre-eclampsia. Normal pregnancy induces dramatic haemodynamic and tubular changes including a 50% increase in glomerular filtration rate (GFR), reduction in serum creatinine, and altered electrolyte handling. Understanding these physiological adaptations is essential for distinguishing normal pregnancy physiology from pathological pre-eclamptic changes and for guiding safe prescribing in pregnancy.
In Australia, the burden of pre-eclampsia disproportionately affects Aboriginal and Torres Strait Islander women, women in rural and remote communities, and those with limited access to specialist antenatal care. Improving risk stratification, prophylaxis uptake, and timely escalation remain national priorities under the National Maternity Services Capability Framework.
Renal Physiological Changes in Pregnancy
Pregnancy induces profound cardiovascular, renal, and endocrine adaptations that are essential to support fetal growth and prepare for the haemodynamic demands of labour and postpartum recovery. Clinicians must understand these changes to avoid misdiagnosing normal physiology as pathology or overlooking true renal disease.
Haemodynamic Changes
- Cardiac output increases by 30–50% by the third trimester, driven by a rise in stroke volume and heart rate (HR typically 10–20 bpm above pre-pregnancy baseline)
- Systemic vascular resistance (SVR) falls by 20–30% due to nitric oxide, progesterone-mediated vasodilation, and the low-resistance uteroplacental circulation
- Mean arterial pressure (MAP) falls by 10–15 mmHg in the second trimester, reaching a nadir at approximately 24 weeks, then gradually returns toward pre-pregnancy levels by term
- Plasma volume expands by 40–50% (peaking at 32–34 weeks), while red cell mass increases by only 20–30%, producing physiological dilutional anaemia
Renal Structural & Haemodynamic Changes
- Kidney length increases by approximately 1 cm due to increased renal blood flow and interstitial volume
- Renal plasma flow (RPF) increases by 50–80% in the first trimester (peaking by 16 weeks), then gradually declines toward non-pregnant levels by term
- GFR increases by approximately 50% (from ~90 mL/min/1.73 m² to ~140 mL/min/1.73 m²) in early pregnancy, paralleling the RPF rise
- Serum creatinine in normal pregnancy is typically 45–70 µmol/L (lower than the non-pregnant reference range of 50–90 µmol/L); a creatinine of >75 µmol/L should raise concern for renal impairment
- Serum urea falls to 2.5–4.0 mmol/L (normal non-pregnant: 2.5–7.0 mmol/L) due to increased GFR and volume expansion
Tubular & Electrolyte Changes
- Enhanced sodium and water reabsorption despite increased GFR: net positive sodium balance of ~900 mmol by term, and total body water increases by 6–8 L
- Serum sodium falls by 3–5 mmol/L (physiological hyponatraemia of pregnancy; normal range ~130–135 mmol/L)
- Serum osmolality decreases by ~10 mOsm/kg due to reset osmostat for ADH release
- Serum potassium falls slightly; aldosterone levels rise significantly, promoting distal tubular K⁺ secretion
- Serum bicarbonate falls to 18–22 mmol/L (respiratory alkalosis with compensatory renal bicarbonate excretion; pCO₂ ~30 mmHg)
- Serum uric acid decreases in early pregnancy (enhanced tubular secretion) but rises in the third trimester; elevated uric acid is an early marker of pre-eclampsia
- Glycosuria and aminoaciduria may occur due to increased filtered load exceeding tubular reabsorption capacity — this does not necessarily indicate gestational diabetes or renal pathology
Urinary Tract Changes
- Physiological hydronephrosis (more pronounced on the right) affects up to 90% of pregnant women by the third trimester; avoid overdiagnosing obstruction
- Ureteric dilation may persist for up to 12 weeks postpartum
- Bladder capacity increases but detrusor tone is reduced, contributing to urinary frequency and incomplete emptying
- Risk of asymptomatic bacteriuria is 2–10% (similar to non-pregnant women) but progression to pyelonephritis is much higher (up to 30% if untreated); screening at first antenatal visit is standard Australian practice
| Parameter | Non-Pregnant | Pregnant (3rd Trimester) | Clinical Significance |
|---|---|---|---|
| Serum Creatinine | 50–90 µmol/L | 45–70 µmol/L | >75 µmol/L suggests impairment |
| Serum Urea | 2.5–7.0 mmol/L | 2.5–4.0 mmol/L | >5.0 mmol/L is abnormal in pregnancy |
| eGFR | ~90 mL/min/1.73 m² | ~140 mL/min/1.73 m² | CKD-EPI formula unreliable; use 24-h creatinine clearance |
| Serum Uric Acid | 0.15–0.40 mmol/L | 0.18–0.32 mmol/L (varies by trimester) | Rising uric acid in 3rd trimester is a marker of pre-eclampsia |
| Serum Sodium | 135–145 mmol/L | 130–135 mmol/L | Physiological hyponatraemia; do not over-correct |
| Serum Bicarbonate | 22–28 mmol/L | 18–22 mmol/L | Compensated respiratory alkalosis is normal |
| Urine Protein | <150 mg/24 h | <300 mg/24 h | ≥300 mg/24 h or PCR ≥30 mg/mmol is pathological |
Pre-eclampsia: Pathophysiology & Diagnosis
Pathophysiology
Pre-eclampsia is a two-stage disorder. Stage 1 involves abnormal placentation: defective remodelling of the spiral arteries by extravillous trophoblast results in inadequate conversion to high-capacity, low-resistance vessels. This creates placental ischaemia and hypoperfusion, triggering release of anti-angiogenic factors (particularly soluble fms-like tyrosine kinase-1 [sFlt-1] and soluble endoglin [sEng]) into the maternal circulation.
Stage 2 represents the maternal systemic inflammatory and endothelial dysfunction response. The imbalance between pro-angiogenic (PlGF, VEGF) and anti-angiogenic factors leads to:
- Widespread endothelial dysfunction and loss of normal vasodilatory response to nitric oxide
- Increased vascular permeability → proteinuria, oedema, hypoalbuminaemia
- Activation of the coagulation cascade → microangiopathic haemolysis, thrombocytopenia
- Cerebral vasospasm and hyperperfusion → headache, visual disturbance, seizures (eclampsia)
- Hepatic sinusoidal endothelial dysfunction → right upper quadrant pain, elevated transaminases, HELLP syndrome
- Glomerular endotheliosis → reduced GFR, rising creatinine and uric acid, proteinuria
- Pulmonary endothelial leak → pulmonary oedema (a severe feature)
Risk Factors
| Risk Category | Factors |
|---|---|
| High risk (≥1 major) | Previous pre-eclampsia; chronic hypertension; pre-existing diabetes (type 1 or 2); CKD; autoimmune disease (SLE, antiphospholipid syndrome); multiple pregnancy |
| Moderate risk (≥2 moderate) | Nulliparity; BMI ≥35; maternal age ≥40; family history of pre-eclampsia; interpregnancy interval >10 years; pre-existing renal disease stage 1–2 |
| ATSI-specific | Higher baseline rates of chronic hypertension, diabetes, and obesity; lower rates of early antenatal booking; higher rates of remote residence limiting access to specialist care |
Prophylaxis with Low-Dose Aspirin
Diagnostic Criteria (SOMANZ / ISSHP)
Pre-eclampsia is diagnosed when both of the following are present after 20 weeks' gestation:
- Hypertension: Systolic BP ≥140 mmHg and/or diastolic BP ≥90 mmHg on two occasions ≥4 hours apart, measured using validated automated device with appropriate cuff size, in the seated position after 5 minutes' rest
- Significant proteinuria: ≥300 mg/24-hour urine collection, or spot urine protein:creatinine ratio (PCR) ≥30 mg/mmol, or urine dipstick ≥2+ (if quantitative testing unavailable)
Severe Features — Criteria for Classification as "Severe Pre-eclampsia"
HELLP Syndrome
HELLP syndrome is a severe complication of pre-eclampsia, occurring in 10–20% of cases. The acronym describes the triad of Haemolysis, Elevated Liver enzymes, and Low Platelets. It is associated with significant maternal morbidity (including hepatic rupture, DIC, placental abruption, and acute kidney injury) and perinatal mortality rates of 7–34% depending on gestational age and severity.
Diagnostic Criteria (Tennessee Classification)
| Component | Diagnostic Threshold | Notes |
|---|---|---|
| Haemolysis | LDH >600 U/L, or peripheral smear showing schistocytes, or bilirubin >20 µmol/L | Haptoglobin <0.25 g/L is the most sensitive marker |
| Elevated Liver Enzymes | AST or ALT >70 U/L (i.e., >2× ULN) | Right upper quadrant / epigastric pain in ~90% of cases |
| Low Platelets | Platelet count <100 × 10⁹/L | Severe thrombocytopenia (<50 × 10⁹/L) increases risk of haemorrhage at delivery |
Mississippi Classification (Severity Sub-classification)
- Class 1 (most severe): Platelets <50 × 10⁹/L, LDH ≥600 U/L, AST/ALT ≥70 U/L
- Class 2: Platelets 50–100 × 10⁹/L, LDH ≥600 U/L, AST/ALT ≥70 U/L
- Class 3: Platelets 100–150 × 10⁹/L, LDH ≥600 U/L, AST/ALT ≥40 U/L
Complications of HELLP Syndrome
- Placental abruption (16–36%)
- Disseminated intravascular coagulation (DIC) (10–20%)
- Hepatic haematoma or rupture (rare but life-threatening)
- Acute kidney injury (7–15%)
- Pulmonary oedema (6–10%)
- Cerebral haemorrhage or infarction
- Retinal detachment
- Wound haematoma (particularly post-caesarean)
Management & Timing of Delivery
Delivery of the placenta is the only definitive treatment for pre-eclampsia and HELLP syndrome. However, the timing of delivery must be carefully balanced between the severity of maternal disease and the risks of prematurity for the fetus. Management follows a structured approach: initial stabilisation, antihypertensive therapy, seizure prophylaxis, maternal and fetal monitoring, and timely delivery.
Antihypertensive Therapy
The target BP in pre-eclampsia is <140/90 mmHg (NICE, SOMANZ). The CHIPS trial (2015) demonstrated that targeting diastolic BP of 85 mmHg (vs 100 mmHg) did not increase perinatal adverse outcomes and reduced maternal severe hypertension.
Seizure Prophylaxis — Magnesium Sulphate
Antenatal Corticosteroids for Fetal Lung Maturity
- Betamethasone 11.4 mg IM × 2 doses 24 hours apart (or dexamethasone 12 mg IM × 2 doses 12 hours apart) — recommended if delivery is anticipated before 34+6 weeks
- Reduces respiratory distress syndrome by ~50% when given 24 hours to 7 days before delivery
- May transiently improve maternal platelet count and liver function in HELLP
- Monitor maternal blood glucose in diabetic women; temporary insulin dose adjustment often required
- PBS General Benefit
Timing of Delivery — RANZCOG/SOMANZ Guidance
| Gestational Age | Severe Pre-eclampsia / HELLP | Non-Severe Pre-eclampsia |
|---|---|---|
| <24 weeks | Offer delivery (perinatal mortality >90%); provide counselling re resuscitation limits | Close surveillance; consider termination if maternal condition deteriorates |
| 24+0 – 33+6 weeks | Deliver if: uncontrollable HTN, eclampsia, HELLP with deteriorating condition, placental abruption, DIC, pulmonary oedema, AKI (creatinine >150 µmol/L); otherwise stabilise then deliver at 34 weeks | Expectant management in tertiary centre with twice-weekly fetal assessment; deliver at 37 weeks |
| 34+0 – 36+6 weeks | Deliver after corticosteroid completion (if given); do not delay beyond 48 h for steroids | Deliver at 37 weeks; induction of labour appropriate if favourable cervix |
| ≥37 weeks | Deliver promptly | Deliver promptly; induction or caesarean as clinically indicated |
Postpartum Management
- Continue magnesium sulphate for at least 24 hours post-delivery or 24 hours post-last eclamptic seizure
- Continue antihypertensives — BP may worsen in the first 3–6 days postpartum due to fluid redistribution and mobilisation of interstitial oedema; step-down gradually over 2–6 weeks
- Monitor FBC, LFTs, renal function, and LDH at 48–72 hours post-delivery (HELLP parameters may transiently worsen before improving)
- Labetalol, nifedipine SR, and enalapril are compatible with breastfeeding
- ACE inhibitors (enalapril, perindopril) may be used postpartum for persistent hypertension — safe in breastfeeding
- Arrange GP follow-up at 2 weeks, 6 weeks, and 6–12 months for BP review, renal function, and cardiovascular risk assessment
- Women with pre-eclampsia have a 2–7× increased lifetime risk of hypertension, ischaemic heart disease, and stroke; encourage healthy lifestyle, weight management, and regular BP screening
Investigations
The following investigations are recommended for assessment and monitoring of pre-eclampsia and HELLP syndrome. Availability of urgent pathology varies by site; metropolitan hospitals will have 24-hour turnaround, while remote and rural centres should establish clear transfer protocols with receiving tertiary centres.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference — Management Summary
📚 References
- 1. Lowe SA, Bowyer L, Lust K, et al. The SOMANZ Guideline for the Management of Hypertensive Disorders of Pregnancy (2014). Aust N Z J Obstet Gynaecol. 2015;55(5):e1–e29.
- 2. Brown MA, Magee LA, Kenny LC, et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations. Hypertension. 2018;72(1):24–43.
- 3. Magee LA, von Dadelszen P, Rey E, et al. Less-Tight versus Tight Control of Hypertension in Pregnancy (CHIPS Trial). N Engl J Med. 2015;372(5):407–417.
- 4. Duley L, Meher S, Hunter KE, et al. Antiplatelet Agents for Preventing Pre-eclampsia and Its Complications. Cochrane Database Syst Rev. 2019;10:CD004659.
- 5. Duley L, Gülmezoglu AM, Henderson-Smart DJ, Chou D. Magnesium Sulphate and Other Anticonvulsants for Women with Pre-eclampsia. Cochrane Database Syst Rev. 2010;(11):CD000025.
- 6. Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Management of Hypertension in Pregnancy. College Statement C-Obs 27. Melbourne: RANZCOG; 2019.
- 7. National Institute for Health and Care Excellence (NICE). Hypertension in Pregnancy: Diagnosis and Management. NICE Guideline [NG133]. London: NICE; 2019 (updated 2022).
- 8. Australian Institute of Health and Welfare (AIHW). Maternal Deaths in Australia 2018–2020. Cat. no. PER 113. Canberra: AIHW; 2023.
- 9. Weinstein L. Syndrome of Hemolysis, Elevated Liver Enzymes, and Low Platelet Count: A Severe Consequence of Hypertension in Pregnancy. Am J Obstet Gynecol. 1982;142(2):159–167.
- 10. Roberts JM, Escudero C. The Placenta in Pre-eclampsia. Pregnancy Hypertens. 2012;2(2):72–83.
- 11. Rana S, Lemoine E, Granger JP, Karumanchi SA. Preeclampsia: Pathophysiology, Challenges, and Perspectives. Circ Res. 2019;124(7):1094–1112.
- 12. Davison JM, Dunlop W. Renal Hemodynamics and Tubular Function in Normal Human Pregnancy. Kidney Int. 1980;18(2):152–161.
- 13. Cheung KL, Lafayette RA. Renal Physiology of Pregnancy. Adv Chronic Kidney Dis. 2013;20(3):209–214.
- 14. Brown MC, Best KE, Pearce MS, Waugh J, Robson SC, Bell R. Cardiovascular Disease Risk in Women with Pre-eclampsia: Systematic Review and Meta-analysis. Eur J Epidemiol. 2013;28(1):1–19.