📋 Key Information Summary
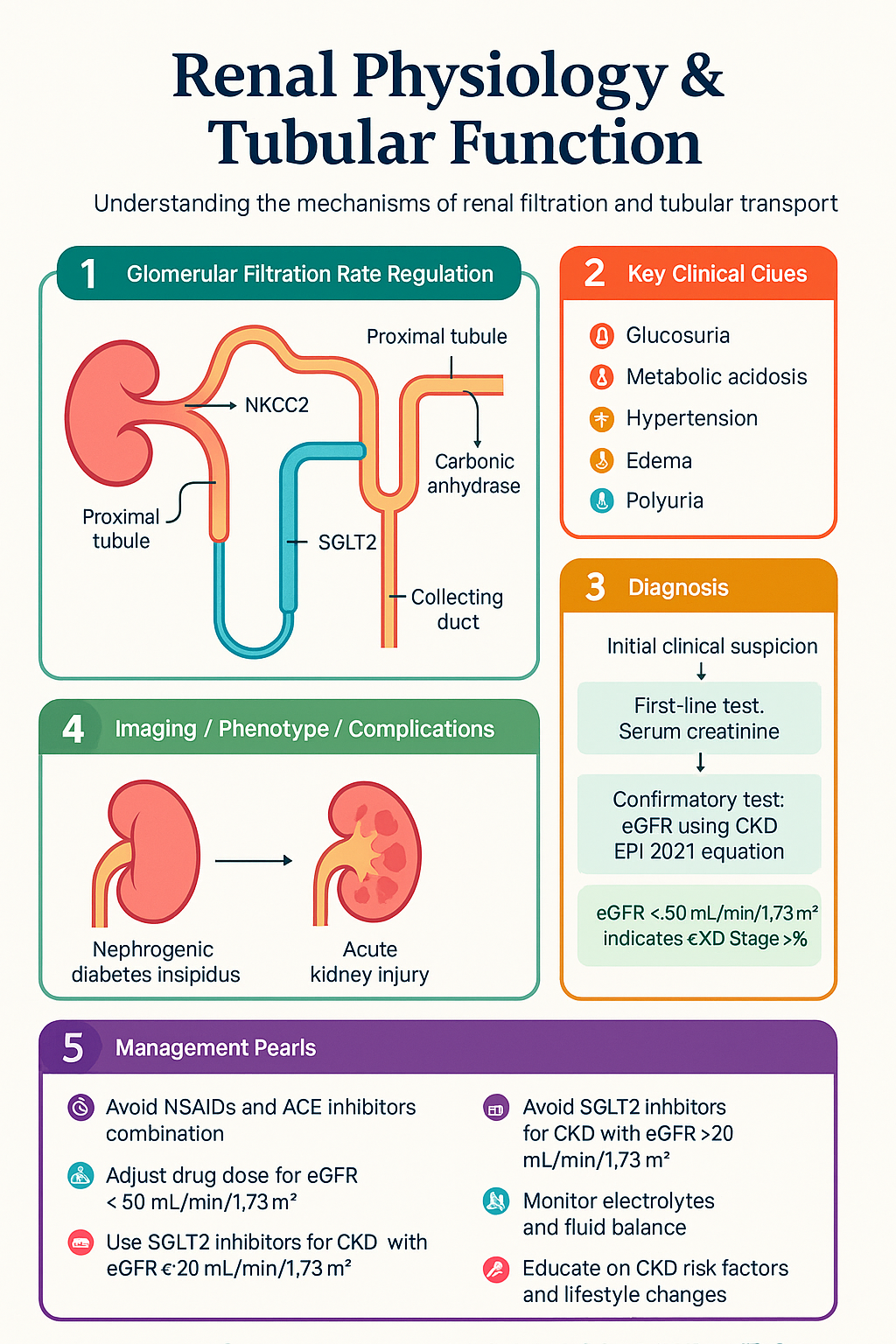
- Glomerular filtration rate (GFR) is the volume of plasma filtered by all functioning glomeruli per unit time; normal adult GFR is approximately 90–120 mL/min/1.73 m², estimated clinically using CKD-EPI 2021 creatinine equation (without race variable) in Australian laboratories.
- Renal blood flow is autoregulated between mean arterial pressures of ~80–180 mmHg via the myogenic response (afferent arteriole) and tubuloglomerular feedback (macula densa sensing NaCl delivery to the distal nephron).
- The proximal tubule reabsorbs ~65% of filtered Na⁺, ~85% of filtered HCO₃⁻, and virtually 100% of filtered glucose and amino acids via sodium-coupled co-transporters (SGLT2/SGLT1, EAAT, Na⁺-coupled amino acid carriers).
- Proximal tubular HCO₃⁻ reclamation depends on luminal carbonic anhydrase IV and intracellular carbonic anhydrase II; inhibition by acetazolamide causes bicarbonaturia and metabolic acidosis.
- The thick ascending limb of the loop of Henle (TAL) reabsorbs ~25% of filtered NaCl via the NKCC2 (Na⁺-K⁺-2Cl⁻) transporter — the target of loop diuretics such as furosemide.
- The TAL is impermeable to water, generating the corticomedullary osmotic gradient essential for urinary concentration; dysfunction causes nephrogenic diabetes insipidus.
- The distal convoluted tubule (DCT) reabsorbs ~5% of filtered NaCl via the NCC (Na⁺-Cl⁻ co-transporter) — the target of thiazide diuretics.
- The collecting duct is the principal site of aldosterone-mediated Na⁺ reabsorption (ENaC) and K⁺ secretion (ROMK channels); also the site of ADH-regulated water reabsorption via aquaporin-2 (AQP2).
- The countercurrent multiplication system (loop of Henle) and countercurrent exchange (vasa recta) maintain a medullary interstitial osmolality of ~300–1200 mOsm/kg, enabling urine concentration up to ~1200 mOsm/kg.
- Prescribing implications: NSAIDs disrupt autoregulation (afferent vasoconstriction); ACE inhibitors reduce efferent tone — both lower GFR and can precipitate acute kidney injury, especially in combination.
- Understanding tubular physiology underpins safe drug dosing: renally excreted medications require dose adjustment when eGFR <60 mL/min/1.73 m²; the Australian Medicines Handbook (AMH) provides standardised guidance.
- SGLT2 inhibitors (dapagliflozin, empagliflozin) exploit proximal tubular physiology to induce glycosuria and natriuresis; now PBS-listed for CKD with eGFR ≥20 mL/min/1.73 m² in Australia.
- Aboriginal and Torres Strait Islander peoples experience CKD at 2–3 times the rate of non-Indigenous Australians, making understanding of tubular physiology critical for culturally safe chronic kidney disease management.
Introduction & Australian Epidemiology
Understanding renal physiology — including glomerular filtration rate regulation, tubular transport mechanisms, and electrolyte handling — is fundamental to interpreting kidney disease, prescribing safely, and managing fluid and electrolyte disorders in clinical practice. The kidney performs excretory, homeostatic, endocrine (erythropoietin, calcitriol), and metabolic functions, with each nephron segment performing specialised transport tasks.
Chronic kidney disease (CKD) affects approximately 1.7 million Australians, with prevalence increasing with age: roughly 20% of adults aged ≥65 years have an eGFR <60 mL/min/1.73 m² (AIHW, 2023). Acute kidney injury (AKI) complicates 10–15% of hospital admissions and up to 50–60% of intensive care unit admissions in Australian tertiary centres. The burden is not equally distributed — Aboriginal and Torres Strait Islander peoples experience end-stage kidney disease (ESKD) at 4–8 times the rate of non-Indigenous Australians, with onset approximately 20 years earlier.
This guideline reviews renal physiology at each nephron segment, emphasising clinical correlations relevant to Australian primary care, emergency medicine, and specialist nephrology practice. Knowledge of where drugs act along the nephron enables rational diuretic prescribing, understanding of drug-induced nephrotoxicity, and appropriate dose adjustment in renal impairment.
GFR & Renal Autoregulation
Glomerular Filtration Rate
GFR is determined by the net ultrafiltration pressure across the glomerular capillary wall, governed by the Starling equation:
where Kf = ultrafiltration coefficient (hydraulic permeability × surface area), PGC = glomerular capillary hydrostatic pressure (~60 mmHg), PBC = Bowman's capsule hydrostatic pressure (~18 mmHg), πGC = glomerular capillary oncotic pressure (~28 mmHg rising to ~35 mmHg at efferent end), πBC ≈ 0 (negligible protein filtration).
The normal single-nephron GFR (SNGFR) is approximately 40–60 nL/min; total GFR across ~1 million nephrons per kidney is approximately 90–120 mL/min/1.73 m² in a healthy young adult.
Determinants of GFR
| Factor | Effect on GFR | Clinical Example |
|---|---|---|
| Afferent arteriolar constriction | ↓↓ GFR | NSAIDs, high sympathetic tone, hypercalcaemia |
| Afferent arteriolar dilation | ↑ GFR | Prostaglandins (PGI₂, PGE₂), low-dose dopamine |
| Efferent arteriolar constriction | ↑ GFR (initially) | Angiotensin II, noradrenaline |
| Efferent arteriolar dilation | ↓ GFR | ACE inhibitors / ARBs |
| ↓ Plasma oncotic pressure | ↑ GFR | Nephrotic syndrome (hypoalbuminaemia) |
| ↑ Bowman's capsule pressure | ↓↓ GFR | Urinary obstruction, tubular obstruction (casts) |
| ↓ Renal plasma flow | ↓ GFR | Hypovolaemia, heart failure, hepatorenal syndrome |
Autoregulation Mechanisms
Renal blood flow (RBF) and GFR are maintained relatively constant over a wide range of mean arterial pressures (~80–180 mmHg) via two primary mechanisms:
1. Myogenic Response (Bayliss Effect)
An increase in perfusion pressure stretches the afferent arteriolar smooth muscle, triggering mechanosensitive ion channel activation, calcium influx, and vasoconstriction — thereby preventing a rise in glomerular capillary pressure and GFR. This response occurs within seconds. Conversely, reduced perfusion pressure causes afferent relaxation.
2. Tubuloglomerular Feedback (TGF)
The macula densa, a specialised epithelial plaque in the early distal tubule (at the junction of TAL and DCT), senses luminal NaCl concentration via the NKCC2 transporter:
- ↑ NaCl delivery to macula densa → ATP/adenosine release → afferent arteriolar constriction → ↓ GFR (negative feedback, preventing Na⁺ wasting).
- ↓ NaCl delivery to macula densa → reduced ATP release + prostaglandin/NO release → afferent dilation + renin release from juxtaglomerular (granular) cells → ↑ angiotensin II → efferent constriction → preserved GFR + ↑ Na⁺ reabsorption.
GFR Measurement & Estimation in Australia
| Method | Details | Availability |
|---|---|---|
| CKD-EPI 2021 creatinine (recommended) | Uses serum creatinine, age, sex; no race coefficient. Validated in Australian populations. Reported automatically by all Australian labs. | Universal |
| CKD-EPI cystatin C | Less affected by muscle mass. Useful when creatinine-based eGFR unreliable (extremes of body habitus, amputees, cirrhosis). | Request test — MBS item 66823 |
| Iohexol or iothalamate clearance (measured GFR) | Gold-standard measurement. Requires IV contrast agent and serial plasma sampling. | Specialist / research |
| 24-hour urine creatinine clearance | Overestimates GFR due to tubular creatinine secretion. Largely superseded by eGFR equations. | Universal — but rarely recommended |
Proximal Tubule Function (Glucose, Amino Acids, HCO₃⁻)
The proximal tubule (PT) is the workhorse of the nephron, responsible for reabsorbing approximately 65% of filtered Na⁺ and water, ~85% of filtered HCO₃⁻, and virtually 100% of filtered glucose and amino acids. It also performs organic anion and cation secretion (drug elimination), gluconeogenesis, ammoniagenesis, and 1α-hydroxylation of 25-hydroxyvitamin D.
Sodium & Water Reabsorption
The basolateral Na⁺/K⁺-ATPase maintains a low intracellular [Na⁺], driving luminal Na⁺ entry through multiple co-transporters and exchangers:
- Na⁺/H⁺ exchanger (NHE3): Accounts for ~2/3 of proximal Na⁺ reabsorption; also mediates H⁺ secretion for HCO₃⁻ reclamation. Angiotensin II stimulates NHE3.
- SGLT2 (S5a segment, early PT): Low-affinity, high-capacity Na⁺-glucose co-transporter; reabsorbs ~90% of filtered glucose. Target of SGLT2 inhibitors.
- SGLT1 (S3 segment, late PT): High-affinity, low-capacity Na⁺-glucose co-transporter; reabsorbs remaining ~10% of glucose.
- Na⁺-amino acid co-transporters: Multiple families (EAAT for acidic amino acids, B⁰AT1 for neutral amino acids, etc.) — virtually 100% reabsorption.
Glucose Handling
Filtered glucose is freely filtered at the glomerulus and entirely reabsorbed in the proximal tubule up to a transport maximum (Tm) of approximately 375 mg/min in males and 300 mg/min in females. The threshold plasma glucose at which glucosuria appears is approximately 10–11 mmol/L (slightly below Tm due to nephron heterogeneity — a "splay" in the titration curve).
- CKD with eGFR ≥20 mL/min/1.73 m² (cardiorenal protection, independent of diabetes) — PBS Authority Required
- Heart failure with reduced ejection fraction (HFrEF) — PBS Authority Required
Bicarbonate Reclamation
Approximately 85% of filtered HCO₃⁻ is reabsorbed in the proximal tubule via the following mechanism:
- Luminal H⁺ secretion via NHE3 (and H⁺-ATPase) combines filtered HCO₃⁻ with H⁺ to form H₂CO₃.
- Membrane-bound carbonic anhydrase IV (CA-IV) rapidly converts H₂CO₃ → CO₂ + H₂O.
- CO₂ diffuses into the cell and is reconverted to HCO₃⁻ + H⁺ by intracellular carbonic anhydrase II (CA-II).
- HCO₃⁻ exits the basolateral membrane via Na⁺/HCO₃⁻ co-transporter (NBCe1-A) into peritubular capillary blood.
The H⁺ secreted intracellularly is recycled via NHE3. The net effect is HCO₃⁻ reclamation without net acid excretion (that occurs primarily in the collecting duct via type A intercalated cells).
Amino Acid Reabsorption
Filtered amino acids are almost completely reabsorbed in the proximal tubule via a variety of Na⁺-dependent and Na⁺-independent co-transporters. Specific transporter defects cause distinct aminoacidurias:
| Disorder | Defective Transporter | Amino Acids Lost | Clinical Features |
|---|---|---|---|
| Cystinuria | rBAT/b⁰,⁺AT (SLC3A1/SLC7A9) | Cystine, lysine, ornithine, arginine | Cystine kidney stones (hexagonal crystals). Managed with hydration >3 L/day, urinary alkalinisation (potassium citrate), tiopronin (not PBS-listed). |
| Hartnup disease | B⁰AT1 (SLC6A19) | Neutral amino acids (tryptophan, etc.) | Pellagra-like rash, cerebellar ataxia (variable). Nicotinamide supplementation. |
| Fanconi syndrome (generalised) | Multiple proximal transporters | All amino acids, glucose, phosphate, HCO₃⁻, urate | Causes: tenofovir, ifosfamide, multiple myeloma, Wilson disease. Rickets/osteomalacia in children. |
Proximal Tubular Drug Secretion
The proximal tubule secretes many drugs and toxins via organic anion transporters (OAT1/3) and organic cation transporters (OCT2/MATE):
- OAT1/3 substrates: Penicillins, cephalosporins, methotrexate, furosemide, NSAIDs, probenecid (competitively inhibits OATs — used historically to prolong penicillin levels).
- OCT2/MATE substrates: Metformin, cisplatin, trimethoprim, cimetidine, procainamide.
- Cisplatin uptake via OCT2 contributes to nephrotoxicity; MATE variants affect renal clearance of metformin (relevant to T2DM patients with CKD).
Loop of Henle & Distal Tubule
Thin Descending Limb
The thin descending limb is highly permeable to water (via AQP1 channels) and moderately permeable to urea and small solutes, but relatively impermeable to NaCl. As tubular fluid descends into the hypertonic medullary interstitium, water is osmotically extracted, concentrating the luminal fluid to ~1200 mOsm/kg at the hairpin turn. This is a passive process — no active transport occurs in this segment.
Thin Ascending Limb
The thin ascending limb is impermeable to water but permeable to NaCl, which passively diffuses out along the concentration gradient established by the descending limb. This contributes to the countercurrent multiplication process.
Thick Ascending Limb (TAL) — The Diluting Segment
The TAL is the pharmacological target of loop diuretics and the primary generator of the medullary osmotic gradient.
NKCC2 (Na⁺-K⁺-2Cl⁻) Co-transporter
The apical NKCC2 (SLC12A1) transporter is the dominant mechanism for NaCl reabsorption in the TAL. It transports 1 Na⁺, 1 K⁺, and 2 Cl⁻ from the lumen into the cell:
- Reabsorbs ~25% of filtered NaCl.
- The TAL is impermeable to water — hence the tubular fluid becomes progressively diluted (hence "diluting segment").
- NaCl reabsorption without water generates the corticomedullary osmotic gradient (300 → 1200 mOsm/kg).
- ROMK (renal outer medullary K⁺) channels recycle K⁺ back into the lumen, generating a lumen-positive transepithelial voltage that drives paracellular reabsorption of Ca²⁺, Mg²⁺, Na⁺, and K⁺.
Bartter Syndrome — NKCC2 & ROMK Defects
Inactivating mutations in TAL transporters cause Bartter syndrome, a group of inherited salt-wasting tubulopathies phenotypically resembling chronic loop diuretic use:
| Type | Gene/Protein | Features |
|---|---|---|
| Type 1 | SLC12A1 (NKCC2) | Antenatal, polyhydramnios, nephrocalcinosis |
| Type 2 | KCNJ1 (ROMK) | Antenatal; transient hyperkalaemia then hypokalaemia |
| Type 3 (classic) | CLCNKB (ClC-Kb) | Later onset; hypokalaemia, metabolic alkalosis, hypercalciuria |
Distal Convoluted Tubule (DCT)
The DCT reabsorbs approximately 5% of filtered NaCl via the apical NCC (Na⁺-Cl⁻ co-transporter, SLC12A3) — the target of thiazide diuretics. The DCT is also a major site of Ca²⁺ reabsorption via TRPV5 channels (stimulated by parathyroid hormone and calcitriol).
Gitelman Syndrome — NCC Defect
Loss-of-function mutations in SLC12A3 (NCC) cause Gitelman syndrome — the most common inherited salt-wasting tubulopathy (prevalence ~1:40,000). Features include hypokalaemia, metabolic alkalosis, hypomagnesaemia, hypocalciuria, and typically presents in adolescence/adulthood. Phenotypically resembles chronic thiazide use. Management: K⁺ and Mg²⁺ supplementation, spironolactone if refractory hypokalaemia.
Juxtaglomerular Apparatus (JGA)
The JGA consists of three cell types that integrate the tubuloglomerular feedback and renin-angiotensin system:
- Granular (JG) cells: Modified smooth muscle cells in the afferent arteriolar wall that synthesise, store, and secrete renin. Stimuli: ↓ renal perfusion pressure, ↓ macula densa NaCl, β₁-adrenergic stimulation, PGE₂.
- Macula densa cells: Sense luminal [NaCl] via NKCC2 and modulate both afferent arteriolar tone and renin release.
- Extraglomerular mesangial (lacis) cells: Transmit signals between macula densa and granular cells.
Collecting Duct & Countercurrent Mechanism
The collecting duct is the final site of urine modification, responsible for fine-tuning Na⁺, K⁺, H⁺, and water excretion under hormonal control. It traverses the medullary osmotic gradient generated by the loop of Henle, enabling both dilute and concentrated urine production.
Principal Cells — Na⁺, K⁺, and Water Handling
Principal cells constitute ~65–70% of collecting duct epithelium and express:
- ENaC (epithelial Na⁺ channel): Apical; mediates electrogenic Na⁺ reabsorption. Stimulated by aldosterone (via mineralocorticoid receptor → SGK1 → ENaC membrane insertion) and ADH. Blocked by amiloride and triamterene.
- ROMK and BK (big-K⁺) channels: Apical; mediate K⁺ secretion. Aldosterone and high tubular flow rates enhance K⁺ secretion (relevant to K⁺-sparing vs K⁺-wasting diuretic effects).
- Aquaporin-2 (AQP2): Apical; ADH (vasopressin, AVP)-regulated water channel. AVP binds V2 receptors on the basolateral membrane → cAMP → PKA → AQP2 vesicle insertion into apical membrane → water reabsorption. AQP3 and AQP4 are constitutively expressed on the basolateral membrane.
Intercalated Cells — Acid-Base Handling
| Cell Type | Function | Key Transporters | Stimulus |
|---|---|---|---|
| Type A (α) intercalated cell | H⁺ secretion (net acid excretion) | Apical H⁺-ATPase, H⁺/K⁺-ATPase; basolateral Cl⁻/HCO₃⁻ exchanger (AE1/Band 3) | Acidosis, aldosterone, hypokalaemia |
| Type B (β) intercalated cell | HCO₃⁻ secretion | Apical Cl⁻/HCO₃⁻ exchanger (pendrin); basolateral H⁺-ATPase | Alkalosis, hypochloraemia |
| Non-A, non-B intercalated cell | Both H⁺ and HCO₃⁻ secretion | Expresses both pendrin and H⁺-ATPase | Transitional state |
Aldosterone Actions — Clinical Pharmacology
Aldosterone, synthesised in the zona glomerulosa of the adrenal cortex, acts on principal cells and intercalated cells via the mineralocorticoid receptor (MR):
- ↑ ENaC expression → ↑ Na⁺ reabsorption → ↑ ECF volume → ↑ blood pressure
- ↑ ROMK expression → ↑ K⁺ secretion → hypokalaemia risk
- ↑ H⁺-ATPase in type A intercalated cells → metabolic alkalosis
ADH (Vasopressin) — Water Balance
ADH (arginine vasopressin, AVP) is synthesised in the hypothalamic supraoptic and paraventricular nuclei, stored in the posterior pituitary, and released in response to:
- ↑ Plasma osmolality (detected by hypothalamic osmoreceptors; threshold ~280 mOsm/kg)
- ↓ Effective circulating volume (detected by baroreceptors in carotid sinus, aortic arch, left atrium)
- Angiotensin II, pain, nausea, certain drugs
ADH binds V2 receptors on the collecting duct principal cell basolateral membrane → Gs → adenylyl cyclase → ↑ cAMP → PKA → AQP2 phosphorylation and insertion into apical membrane → water reabsorption → concentrated urine. ADH also stimulates urea transporter UT-A1 in the inner medullary collecting duct, enhancing urea recycling and medullary concentration capacity.
Liddle Syndrome — ENaC Gain-of-Function
Activating mutations in ENaC subunits (SCNN1B, SCNN1G) cause Liddle syndrome — a rare autosomal dominant form of early-onset hypertension characterised by:
- Hypertension (often severe, presenting in adolescence/young adulthood)
- Hypokalaemia, metabolic alkalosis
- Low renin and low aldosterone (suppressed by volume expansion)
- Treatment: amiloride (directly blocks ENaC) — not spironolactone (aldosterone is already suppressed)
Countercurrent Multiplication & Exchange
The corticomedullary osmotic gradient (300 → 1200 mOsm/kg) is established by the countercurrent multiplication system and preserved by the countercurrent exchange system:
Countercurrent Multiplication (Loop of Henle)
- Single effect: NKCC2 in the TAL actively pumps NaCl into the interstitium (without water, as TAL is water-impermeable), creating a ~200 mOsm/kg transepithelial gradient.
- Multiplication: The hairpin turn of the loop allows the ascending and descending limbs to operate in a countercurrent arrangement, multiplicatively amplifying the single effect along the corticomedullary axis.
- Urea recycling: ADH-stimulated UT-A1 in the inner medullary collecting duct allows urea to enter the medullary interstitium, contributing ~50% of the inner medullary osmolality. Urea then re-enters the thin descending limb via UT-A2, completing the recycling loop.
Countercurrent Exchange (Vasa Recta)
The vasa recta are specialised peritubular capillaries that run parallel to the loops of Henle in the medulla. Their hairpin configuration and high permeability to solutes and water allow them to supply oxygen and nutrients to the medulla without dissipating the osmotic gradient:
- Descending vasa recta: blood gains solute (NaCl, urea) and loses water as it descends into the hypertonic medulla.
- Ascending vasa recta: blood loses solute and gains water as it returns toward the cortex.
- Net effect: medullary blood flow washes out only a small fraction of the gradient, preserving concentrating ability.
Diabetes Insipidus — Collecting Duct Water Handling
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Clinical Correlations & Prescribing Implications
A thorough understanding of renal physiology enables rational prescribing, anticipation of drug effects, and early recognition of tubulopathies. The following table summarises the key nephron segment–drug interactions:
| Nephron Segment | Key Transporter | Drug Target | Clinical Effect |
|---|---|---|---|
| Proximal tubule | SGLT2 | Dapagliflozin, empagliflozin | Glycosuria, natriuresis, cardiorenal protection |
| Proximal tubule | CA-IV / CA-II | Acetazolamide | Bicarbonaturia, metabolic acidosis |
| TAL | NKCC2 | Furosemide, bumetanide | Natriuresis, K⁺ wasting, gradient destruction |
| DCT | NCC | Hydrochlorothiazide, indapamide | Natriuresis, ↑ Ca²⁺ reabsorption, hypokalaemia |
| Collecting duct | ENaC | Amiloride, triamterene | Na⁺ wasting, K⁺ sparing |
| Collecting duct | MR | Spironolactone, eplerenone | Na⁺ wasting, K⁺ sparing, anti-fibrotic |
| Collecting duct | AQP2 (via V2R) | Desmopressin | Water retention, concentrated urine |