📋 Key Information Summary
- Lupus nephritis (LN) develops in approximately 40–60% of systemic lupus erythematosus (SLE) patients, typically within the first 5 years of diagnosis.
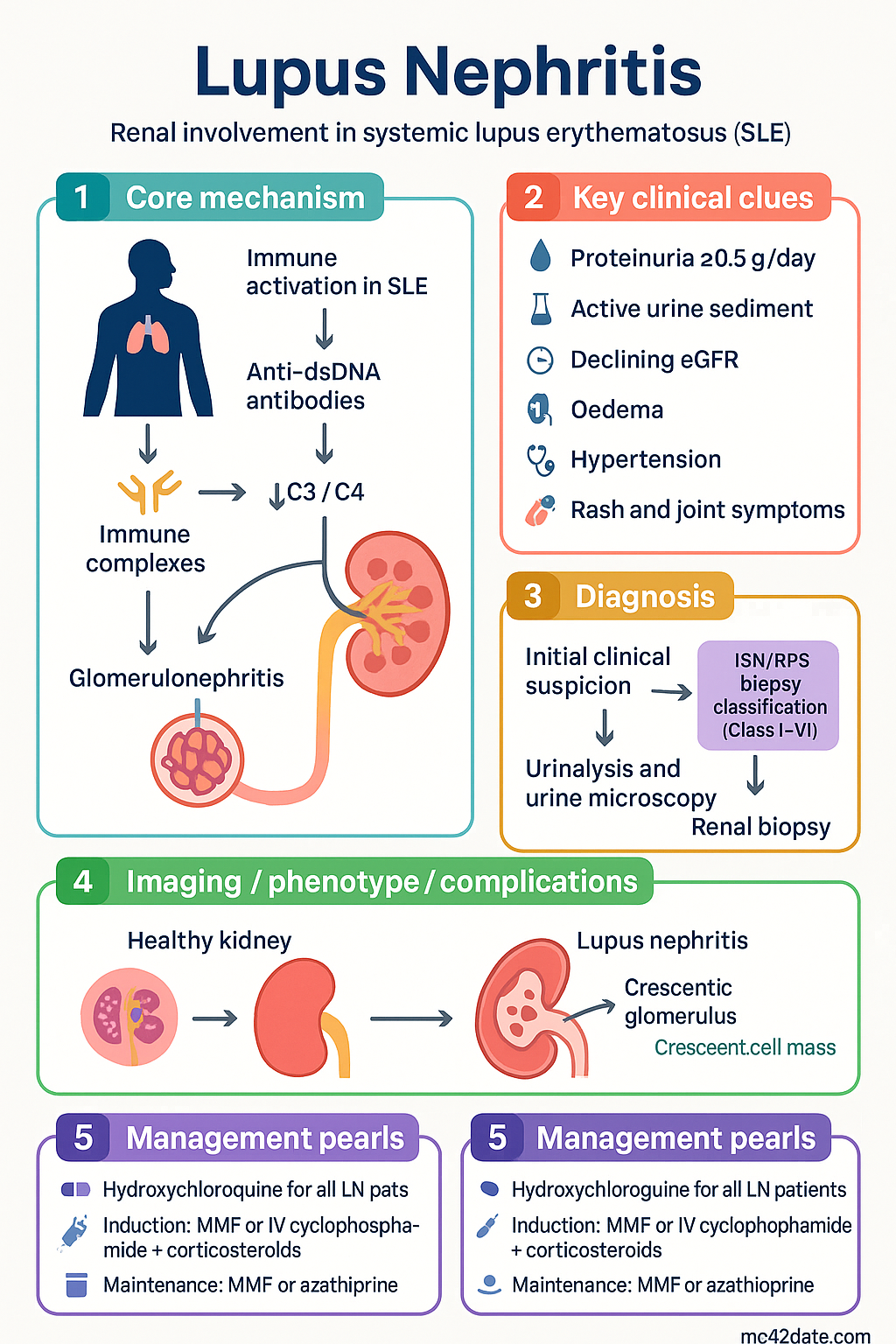
- ISN/RPS biopsy classification (Class I–VI) guides prognosis and treatment intensity; Class III (focal) and Class IV (diffuse) proliferative nephritis carry the highest risk of end-stage kidney disease (ESKD).
- All patients with SLE and clinical renal involvement (proteinuria ≥0.5 g/day, active sediment, declining eGFR) require a renal biopsy for definitive classification.
- Hydroxychloroquine (Plaquenil®) is recommended for ALL patients with LN regardless of class — reduces flares, thrombotic risk, and improves long-term renal survival.
- Induction therapy for Class III/IV LN: mycophenolate mofetil (MMF) or intravenous cyclophosphamide (Euro-Lupus or NIH regimen) plus corticosteroids.
- Maintenance therapy for Class III/IV: MMF (preferred) or azathioprine for at least 3–5 years after complete/partial response.
- Class V (membranous) LN with nephrotic-range proteinuria: MMF + low-dose corticosteroids; add calcineurin inhibitor (tacrolimus) if suboptimal response.
- Belimumab (Benlysta®) is PBS-authority approved as add-on therapy in active LN with inadequate response to standard immunosuppression.
- Voclosporin (Lupkynis®) — a novel calcineurin inhibitor — has emerging evidence (AURORA trial) and TGA approval for Class III–V LN.
- Anti-dsDNA titres and complement levels (C3/C4) correlate with disease activity but should be interpreted alongside clinical and histological findings.
- All immunosuppressed patients require Pneumocystis jirovecii prophylaxis (trimethoprim-sulfamethoxazole) and cardiovascular risk factor optimisation.
- Aboriginal and Torres Strait Islander peoples have higher SLE prevalence, later presentation, and worse renal outcomes — targeted screening and culturally safe care are essential.
Introduction & Australian Epidemiology
Lupus nephritis (LN) is one of the most serious and common organ-threatening manifestations of systemic lupus erythematosus (SLE), occurring in approximately 40–60% of SLE patients during the course of their disease. Renal involvement typically presents within the first five years of SLE diagnosis and is a major determinant of morbidity and mortality, with up to 10–30% of patients with proliferative LN progressing to end-stage kidney disease (ESKD) within 15 years.
In Australia, SLE affects an estimated 20–50 per 100,000 population, with significantly higher prevalence among women of childbearing age (female-to-male ratio approximately 9:1). Aboriginal and Torres Strait Islander Australians experience a disproportionate burden of autoimmune disease, including SLE and LN, with higher rates of renal disease, later presentation, and poorer long-term outcomes compared to non-Indigenous Australians. The AIHW reports that chronic kidney disease related to autoimmune glomerulonephritis contributes meaningfully to the ESKD burden in Indigenous communities.
The World Health Organization (WHO) classification of lupus nephritis, originally developed in 1974 and subsequently revised by the International Society of Nephrology/Renal Pathology Society (ISN/RPS) in 2003 and updated in 2018, provides a standardised histopathological framework that guides prognostication and therapeutic decision-making. The ISN/RPS classification (Class I–VI) remains the cornerstone of LN management in Australian nephrology and rheumatology practice.
Management of LN has evolved significantly over the past two decades. While intravenous cyclophosphamide combined with corticosteroids was historically the standard induction regimen, mycophenolate mofetil (MMF) has emerged as equally effective with a more favourable safety profile and is now the preferred first-line induction and maintenance agent in most Australian centres. Biologic therapies — particularly belimumab (Benlysta®), now PBS-listed for LN — and the calcineurin inhibitor voclosporin represent important additions to the therapeutic armamentarium. This guideline synthesises current Australian and international evidence for the diagnosis, classification, and management of lupus nephritis in the Australian healthcare context.
ISN/RPS Classification (Class I–VI)
The ISN/RPS classification system requires adequate renal biopsy tissue (minimum 10 glomeruli on light microscopy, ideally ≥20) and mandates immunofluorescence and electron microscopy for complete evaluation. Classes are defined by the predominant histological pattern; however, mixed patterns and transformation between classes over time are well recognised.
| Class | Name | Light Microscopy | IF / EM | Clinical Relevance |
|---|---|---|---|---|
| I | Minimal mesangial LN | Normal LM | Mesangial immune deposits | No clinical renal disease; no treatment required |
| II | Mesangial proliferative LN | Mesangial hypercellularity or matrix expansion | Mesangial deposits | Mild proteinuria (<1 g/day), no active sediment; treat SLE globally; monitor |
| III | Focal LN | Endocapillary or extracapillary proliferation in <50% of glomeruli | Subendothelial ± mesangial deposits | Active nephritis; requires immunosuppression; subclassified A (active), A/C, C (chronic) |
| IV | Diffuse LN | Proliferation in ≥50% of glomeruli (segmental [IV-S] or global [IV-G]) | Subendothelial ± mesangial deposits | Most aggressive proliferative class; highest ESKD risk; aggressive induction required |
| V | Membranous LN | Diffuse thickening of GBM with subepithelial deposits | Diffuse subepithelial deposits | Nephrotic syndrome common; may coexist with III or IV (mixed); different therapeutic approach |
| VI | Advanced sclerosing LN | ≥90% globally sclerosed glomeruli without residual activity | Few residual deposits | Irreversible; immunosuppression not indicated; manage as CKD; plan for RRT |
Activity Index (AI) and Chronicity Index (CI): The NIH activity index scores glomerular proliferation, leucocyte infiltration, karyorrhexis, fibrinoid necrosis, cellular crescents, hyaline deposits, and interstitial inflammation (0–24). The chronicity index scores glomerular sclerosis, fibrous crescents, tubular atrophy, and interstitial fibrosis (0–12). An AI >12 suggests aggressive disease; a CI >7 portends poor renal recovery and progression to ESKD.
Clinical Features & Renal Presentation
The clinical presentation of lupus nephritis varies substantially depending on the histological class, ranging from asymptomatic urinary abnormalities detected on screening to rapidly progressive glomerulonephritis (RPGN) with acute kidney injury. In Australian practice, routine urinalysis and serum creatinine monitoring at every SLE review is standard of care.
Typical Clinical Presentations by Class
Key Clinical Signs to Assess
- Oedema: Peripheral, periorbital, sacral — suggests nephrotic syndrome or fluid overload from AKI.
- Hypertension: Present in 30–50% of LN at diagnosis; correlates with disease severity and chronicity.
- Rash: Active malar rash or discoid lesions may parallel renal flare activity.
- Joint symptoms: Synovitis may indicate concurrent systemic flare.
- Serositis: Pleuritis or pericarditis suggests high systemic disease activity.
- Cytopenias: Thrombocytopenia, leucopenia, or haemolytic anaemia may coexist with renal flare.
Investigations (Biopsy, Complement, Anti-dsDNA)
Investigation of suspected lupus nephritis requires a combination of serological markers, urine studies, renal function assessment, and — critically — renal biopsy for histopathological classification. The following investigations should be performed in all patients with SLE and evidence of renal involvement.
Risk Stratification & Severity Scoring
Risk stratification in lupus nephritis integrates histological class, activity/chronicity indices, clinical severity markers, and patient factors to guide treatment intensity and prognostication.
Poor Prognostic Factors
- Diffuse proliferative class (IV-S or IV-G) with crescents
- Chronicity index >7 (tubular atrophy, interstitial fibrosis, global sclerosis)
- Failure to achieve complete or partial response within 6–12 months
- African, Hispanic, or Aboriginal Australian ethnicity (higher ESKD progression rates)
- Delayed diagnosis (>6 months from onset of renal involvement to treatment)
- Persistent nephrotic-range proteinuria despite induction therapy
- Recurrent renal flares (≥2 flares associated with increased chronicity)
- Non-adherence to hydroxychloroquine and immunosuppressive therapy
Management
Management of lupus nephritis involves a multiphase approach: induction of remission, maintenance of remission, and long-term supportive care. All patients require hydroxychloroquine, RAAS blockade (ACE inhibitor or ARB), cardiovascular risk optimisation, and bone protection. Immunosuppressive therapy is determined by ISN/RPS class, severity, and patient factors.
Universal Measures (All Classes)
- Hydroxychloroquine: Recommended for ALL patients with SLE and LN regardless of class — reduces flares by 50%, decreases thrombotic risk, improves renal survival, and reduces mortality.
- RAAS blockade: ACE inhibitor or ARB for proteinuria reduction and renoprotection. Target BP <130/80 mmHg (or <125/75 if proteinuria >1 g/day).
- Statin therapy: If dyslipidaemia or cardiovascular risk factors present. Nephrotic syndrome itself increases CV risk.
- Vitamin D and calcium: Supplementation in all patients receiving corticosteroids. Target 25-OH vitamin D >75 nmol/L.
- PJP prophylaxis: Trimethoprim-sulfamethoxazole (TMP-SMX) 480 mg daily or 960 mg three times weekly if receiving significant immunosuppression (MMF, cyclophosphamide, or high-dose corticosteroids).
- Vaccination: Influenza annually, pneumococcal (Prevenar 13 then Pneumovax 23), COVID-19 as per ATAGI. Avoid live vaccines on immunosuppression. Hepatitis B if not immune.
Hydroxychloroquine
Class III/IV Proliferative LN — Induction Therapy
Two equally accepted induction regimens are used in Australian practice. The choice between MMF and IV cyclophosphamide depends on centre experience, patient factors (fertility, infection risk, prior intolerance), and access to infusion services.
Option A: Mycophenolate Mofetil (MMF) + Corticosteroids
Corticosteroids (Induction Phase)
Option B: Intravenous Cyclophosphamide + Corticosteroids
Class V (Membranous) LN — Management
Pure Class V LN without proliferative component presents primarily with nephrotic syndrome. Treatment differs from proliferative classes.
- Non-nephrotic Class V (proteinuria <3.5 g/day): Hydroxychloroquine + RAAS blockade + corticosteroids; immunosuppression may be deferred if eGFR stable.
- Nephrotic Class V (proteinuria ≥3.5 g/day): MMF (2–3 g/day) + low-dose prednisolone (0.5 mg/kg, taper to ≤10 mg by 3 months). Add tacrolimus (0.05–0.1 mg/kg/day) if suboptimal response at 6 months.
- Resistant Class V: Consider rituximab (off-label but widely used; increasing evidence from LUNAR trial subgroup analyses and real-world data).
Maintenance Therapy (Class III/IV/V after induction)
After achieving complete or partial response to induction, patients require prolonged maintenance immunosuppression to prevent relapse. The ALMS maintenance trial demonstrated superiority of MMF over azathioprine for preventing renal flares.
Biologic & Novel Therapies
Belimumab (Benlysta®)
Voclosporin (Lupkynis®)
Treatment Response Definitions
| Response | Definition |
|---|---|
| Complete response | Proteinuria <0.5 g/day (uPCR <50 mg/mmol), normal or stable eGFR (within 10% of baseline or eGFR ≥90), inactive urine sediment |
| Partial response | ≥50% reduction in proteinuria from peak, stable or improved eGFR |
| Treatment failure | Failure to achieve partial response by 6 months or complete response by 12 months; worsening proteinuria or eGFR despite therapy |
| Renal flare | Reappearance of active sediment, rise in proteinuria ≥50%, or new/worsening renal impairment after prior response |
Management of Treatment Failure / Refractory LN
- If MMF induction fails at 6 months: switch to IV cyclophosphamide (or vice versa).
- If both MMF and cyclophosphamide fail: consider rituximab (1 g IV × 2 doses, 2 weeks apart) — increasing evidence from observational studies and RCTs (LUNAR trial showed trend to benefit).
- Add-on belimumab to standard therapy is supported by BLISS-LN data.
- Voclosporin as add-on to MMF is an option (AURORA data) but access is limited by PBS status.
- Re-biopsy should be considered if treatment failure persists — may reveal class transformation or increased chronicity.
Monitoring
Regular monitoring is essential to detect treatment response, disease flares, and medication toxicity. The following schedule applies to patients with active LN on immunosuppressive therapy:
Drug-Specific Monitoring
| Drug | Monitoring | Frequency |
|---|---|---|
| Hydroxychloroquine | Ophthalmology review (OCT + visual fields) | Baseline, then annually from year 5 (or earlier if risk factors) |
| MMF | FBC, LFTs; consider MPA-AUC levels | FBC every 2 weeks × 3 months, then monthly; levels if suboptimal response |
| Cyclophosphamide | FBC at nadir, urinalysis (haematuria), LFTs | FBC days 10–14 post each infusion; urinalysis at each visit |
| Azathioprine | FBC, LFTs; TPMT/NUDT15 before initiation | FBC every 2 weeks × 2 months, then monthly |
| Belimumab | Infection screening, FBC | Prior to each infusion; infection assessment at each visit |
| Voclosporin | eGFR, BP, lipid panel, potassium | eGFR weekly × 4 weeks, then every 2 weeks × 2 months, then monthly |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Bajema IM, Wilhelmus S, Alpers CE, et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018;93(4):789–796.
- 2. Appel GB, Contreras G, Dooley MA, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Am Soc Nephrol. 2009;20(5):1103–1112. (ALMS trial)
- 3. Houssiau FA, Vasconcelos C, D'Cruz D, et al. The 10-year follow-up data of the Euro-Lupus Nephritis Trial comparing low-dose and high-dose intravenous cyclophosphamide. Ann Rheum Dis. 2010;69(1):61–64.
- 4. Dooley MA, Jayne D, Ginzler EM, et al. Mycophenolate versus azathioprine as maintenance therapy for lupus nephritis. N Engl J Med. 2011;365(20):1886–1895. (ALMS Maintenance trial)
- 5. Furie R, Rovin BH, Houssiau F, et al. Two-year, randomized, controlled trial of belimumab in lupus nephritis. N Engl J Med. 2020;383(12):1117–1128. (BLISS-LN trial)
- 6. Rovin BH, Teng YKO, Ginzler EM, et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2021;397(10289):2070–2080.
- 7. Hahn BH, McMahon MA, Wilkinson A, et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 2012;64(6):79