📋 Key Information Summary
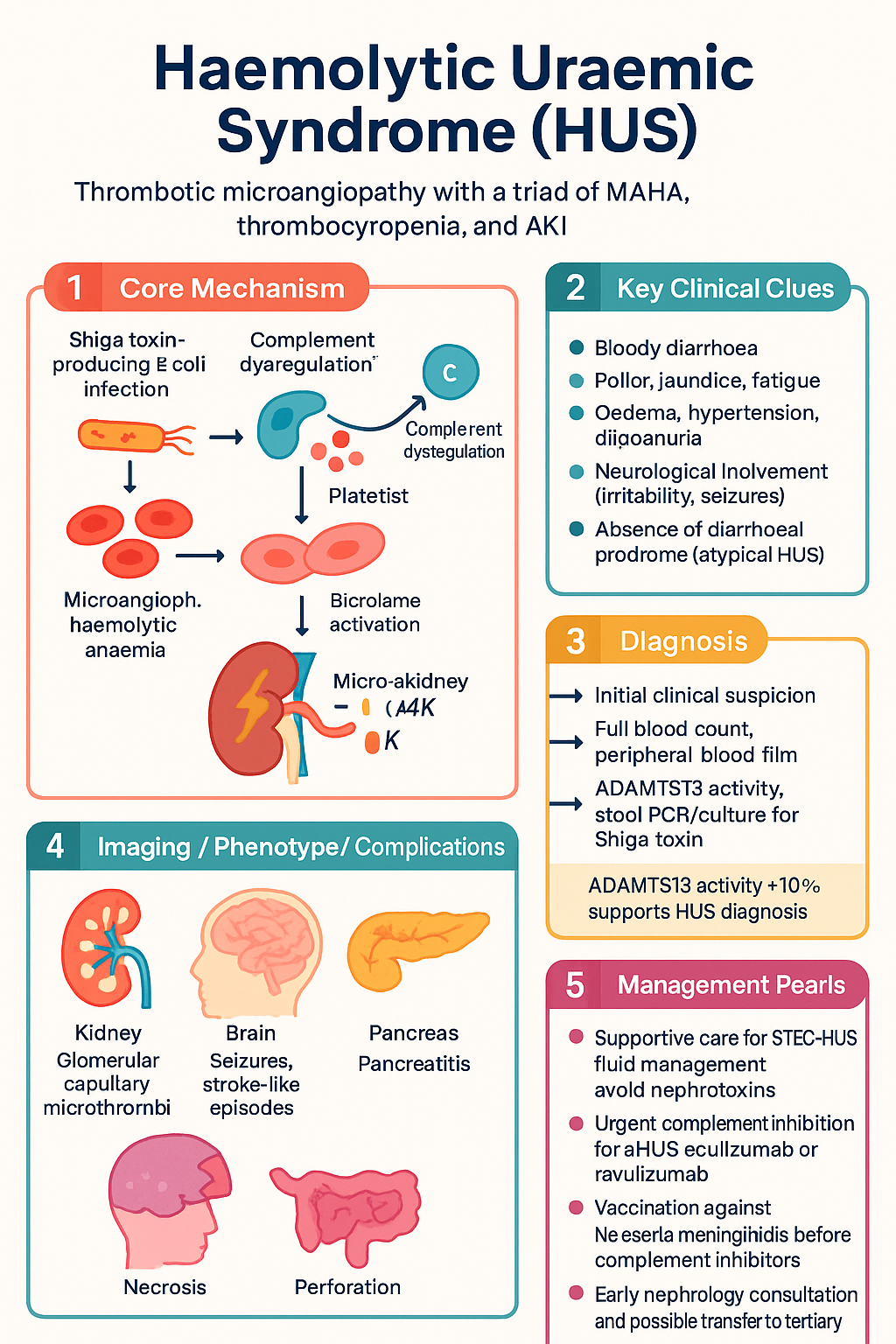
- Haemolytic uraemic syndrome (HUS) is a thrombotic microangiopathy (TMA) defined by the triad of microangiopathic haemolytic anaemia (MAHA), thrombocytopenia, and acute kidney injury (AKI).
- Typical (diarrhoea-positive) HUS is caused by Shiga toxin-producing Escherichia coli (STEC) — predominantly O157:H7 — and accounts for approximately 90% of paediatric HUS cases in Australia.
- Atypical HUS (aHUS) is caused by uncontrolled complement alternative pathway activation and represents approximately 5–10% of all HUS presentations; it is often diarrhoea-negative and carries significant risk of end-stage kidney disease (ESKD).
- STEC-HUS management is primarily supportive: careful fluid and electrolyte management, avoidance of nephrotoxins, and renal replacement therapy (RRT) when indicated. Antibiotics are generally contraindicated in suspected STEC infection.
- Antibiotic use in STEC may increase the risk of HUS by promoting Shiga toxin release; avoid empirical antibiotics in bloody diarrhoea until STEC is excluded.
- aHUS requires urgent complement inhibition with eculizumab (Soliris®) or ravulizumab (Ultomiris®), which are PBS Authority Required in Australia for complement-mediated aHUS.
- Before initiating complement inhibitor therapy, exclude TTP (ADAMTS13 activity <10%), STEC-HUS (stool PCR/culture for Shiga toxin), drug-induced TMA, and secondary TMA causes.
- Vaccination against Neisseria meningitidis (MenACWY + MenB) is mandatory before starting eculizumab or ravulizumab due to life-threatening meningococcal infection risk.
- Australian STEC notifications have risen in recent years; OzFoodNet reports outbreaks linked to contaminated salad greens, raw milk, and undercooked minced beef.
- Aboriginal and Torres Strait Islander children experience higher rates of infectious gastroenteritis and may present later with more severe STEC-HUS, requiring outreach and telepaediatric support.
- Early nephrology consultation is essential for all suspected HUS; transfer to a paediatric tertiary centre is recommended for children requiring dialysis or suspected aHUS.
- Long-term follow-up is critical: up to 25% of STEC-HUS survivors develop chronic kidney disease (CKD), and aHUS patients on complement inhibitors require lifelong monitoring.
Introduction & Australian Epidemiology
Haemolytic uraemic syndrome (HUS) is a form of thrombotic microangiopathy (TMA) characterised by the clinical triad of microangiopathic haemolytic anaemia (MAHA), consumptive thrombocytopenia, and acute kidney injury (AKI). It is the most common cause of AKI in young children in Australia and other high-income countries.
HUS is broadly classified into two major subtypes:
- Typical HUS (STEC-HUS / diarrhoea-associated HUS): Accounts for approximately 90% of paediatric HUS cases. Caused by Shiga toxin-producing Escherichia coli (STEC), most commonly serotype O157:H7. Preceded by a prodrome of bloody diarrhoea.
- Atypical HUS (aHUS / complement-mediated HUS): Accounts for approximately 5–10% of cases. Driven by dysregulated activation of the complement alternative pathway due to genetic mutations or acquired autoantibodies. Often diarrhoea-negative at presentation.
Australian Epidemiology
In Australia, STEC is a notifiable condition under the National Notifiable Diseases Surveillance System (NNDSS). OzFoodNet data indicate an annual notification rate of approximately 0.5–1.0 per 100,000 population for STEC infection nationally, with seasonal peaks in summer and autumn. The progression rate from confirmed STEC infection to HUS is approximately 8–15% in children under 5 years of age.
Key Australian epidemiological observations include:
- Age distribution: STEC-HUS predominantly affects children aged 6 months to 5 years (median age 2–3 years), though adult cases occur, particularly in the elderly.
- Serotype distribution: While O157:H7 remains the most common STEC serotype in Australia, non-O157 serotypes (O26, O111, O121) are increasingly identified, particularly in South Australia and Queensland.
- Outbreak sources: Documented Australian outbreaks have been linked to contaminated lettuce and salad greens, petting zoos, farm visits, raw milk products, and undercooked minced beef.
- Indigenous considerations: Aboriginal and Torres Strait Islander children in remote communities may experience higher exposure to STEC through environmental water sources and limited food safety infrastructure, with delayed access to specialist nephrology care.
- Regional variation: South Australia has historically reported the highest STEC notification rates in Australia, linked to intensive local surveillance and molecular testing.
Typical HUS (STEC-HUS): Pathophysiology
STEC-HUS follows a well-characterised sequence of events initiated by ingestion of Shiga toxin-producing E. coli, most commonly through contaminated food or water.
Step 1: Colonisation & Shiga Toxin Production
After ingestion, STEC colonises the large intestine using attaching-and-effacing (A/E) lesions mediated by the locus of enterocyte effacement (LEE) pathogenicity island. Intimate attachment to colonic enterocytes triggers local inflammation and bloody diarrhoea. Shiga toxin (Stx1 and/or Stx2) is produced in the gut lumen and released during bacterial lysis.
Step 2: Toxin Translocation & Endothelial Injury
Shiga toxin crosses the intestinal epithelial barrier into the systemic circulation. It binds to globotriaosylceramide (Gb3/CD77) receptors expressed on renal glomerular endothelial cells, and to a lesser extent on intestinal, cerebral, and pancreatic endothelium. The toxin is internalised via receptor-mediated endocytosis, inhibits ribosomal protein synthesis via N-glycosidase activity, and triggers endothelial cell apoptosis and activation.
Step 3: Thrombotic Microangiopathy
Damaged endothelial cells lose their normal antithrombotic surface properties. Consequences include:
- Upregulation of von Willebrand factor (vWF) and tissue factor release.
- Loss of heparan sulfate and thrombomodulin expression.
- Platelet adhesion, activation, and aggregation on exposed subendothelium.
- Fibrin deposition forming microthrombi predominantly in the renal glomerular capillaries.
- Mechanical fragmentation of red blood cells passing through partially occluded vessels → microangiopathic haemolytic anaemia with schistocytes on peripheral blood film.
- Consumptive thrombocytopenia as platelets are consumed in microthrombi.
- Glomerular ischaemia and acute tubular injury → AKI (the dominant clinical feature).
Step 4: Complement Activation (Secondary)
Shiga toxin also directly activates the alternative complement pathway, cleaving factor H binding sites on endothelial cells and amplifying the microangiopathic process. This has led to investigation of complement inhibition as adjunctive therapy in severe STEC-HUS, though current evidence does not support routine use of eculizumab in typical HUS outside clinical trials.
Atypical HUS (aHUS): Complement Dysregulation
Atypical HUS (aHUS) results from uncontrolled activation of the complement alternative pathway on endothelial surfaces, leading to a complement-mediated thrombotic microangiopathy that is clinically indistinguishable from STEC-HUS and TTP at presentation, but requires fundamentally different treatment.
Genetic & Acquired Causes
A pathogenic complement gene variant or autoantibody is identified in approximately 60–70% of aHUS cases. The major genetic and acquired defects include:
| Defect Type | Gene / Factor | Frequency in aHUS | Mechanism |
|---|---|---|---|
| Loss-of-function (regulators) | Factor H (CFH) | 20–30% | Impaired C3b inactivation on endothelium |
| Loss-of-function | Membrane cofactor protein (CD46/MCP) | 10–15% | Reduced cell-surface complement regulation |
| Loss-of-function | Factor I (CFI) | 5–10% | Impaired C3b/Factor B cleavage |
| Gain-of-function (activators) | Factor B (CFB) | 1–4% | Excessive C3 convertase formation |
| Gain-of-function | C3 (C3) | 5–10% | Resistance to Factor H/mediated inactivation |
| Acquired autoantibody | Anti-Factor H antibodies | 5–10% | Block Factor H regulatory function on endothelium |
| Thrombomodulin | THBD | 3–5% | Impaired protein C activation and complement modulation |
Triggering Events
aHUS may manifest de novo or be triggered by events that stress the complement system:
- Infection (including STEC — so-called "aHUS triggered by STEC")
- Pregnancy (particularly postpartum)
- Surgery or trauma
- Drugs: calcineurin inhibitors (cyclosporin, tacrolimus), anti-VEGF agents (bevacizumab, sunitinib), oral contraceptive pill
- Transplantation (de novo or recurrent aHUS in renal allografts)
- Malignancy
Pathophysiology of Complement-Mediated TMA
Under normal conditions, the alternative complement pathway undergoes continuous low-grade ("tick-over") activation in plasma. Endothelial surfaces are protected by membrane-bound regulators (MCP/CD46) and fluid-phase regulators (Factor H, Factor I). In aHUS, loss of these protective mechanisms — or excessive complement activation — results in:
- Unchecked C3 convertase (C3bBb) activity on the glomerular endothelial surface.
- Massive C3b deposition, membrane attack complex (C5b-9) formation, and endothelial damage.
- Thrombotic microangiopathy identical in histopathology to STEC-HUS but mediated entirely by complement rather than Shiga toxin.
Prognosis by Genotype
Clinical Features & Laboratory Findings
STEC-HUS — Typical Presentation
The classic presentation follows a predictable sequence:
- Prodrome (Days 1–3): Abdominal cramps, watery diarrhoea progressing to bloody diarrhoea. Low-grade fever may be present. The causative exposure typically occurred 2–8 days earlier.
- HUS phase (Days 3–10): Onset of pallor (anaemia), oliguria or anuria (AKI), and petechiae or purpura (thrombocytopenia). The platelet count nadir typically precedes the peak of AKI by 1–2 days.
Clinical features may include:
- Pallor, jaundice (from haemolysis), fatigue
- Oedema, hypertension, oligoanuria
- Petechiae, purpura, mucosal bleeding (generally mild)
- Abdominal distension, ileus, bloody stools
- Neurological involvement (10–20%): irritability, seizures, altered consciousness, stroke
- Pancreatitis (hyperamylasaemia in ~30%; clinically significant in ~5%)
- Colonic necrosis, perforation (rare but serious)
- Myocardial ischaemia or cardiomyopathy (rare)
Atypical HUS — Presentation
aHUS may present at any age (including neonates and adults). Key distinguishing features from STEC-HUS include:
- Absence of a diarrhoeal prodrome (though preceding infection may be present)
- Insidious onset with progressive AKI, often severe at presentation
- More severe and relapsing course without complement inhibition
- May present in association with pregnancy, postpartum period, or drug exposure
- Family history of HUS or ESKD may be present (~20% have familial disease)
Laboratory Findings — Shared Features
| Investigation | Expected Finding | Clinical Significance |
|---|---|---|
| Full blood count | Hb ↓ (often <80 g/L), Plt ↓ (often <60 × 10⁹/L), WCC ↑ | MAHA + thrombocytopenia = TMA triad components |
| Peripheral blood film | Schistocytes (fragmented RBCs), polychromasia | Confirms microangiopathic haemolysis |
| Reticulocyte count | Elevated | Bone marrow response to haemolysis |
| LDH | Markedly elevated (>500 U/L, often >1000) | Tissue ischaemia + haemolysis marker |
| Haptoglobin | Low / undetectable | Confirms haemolysis |
| Unconjugated bilirubin | Elevated | Haemolysis |
| Coombs test (DAT) | Negative | Distinguishes TMA from autoimmune haemolytic anaemia |
| Creatinine / eGFR | Acute rise (AKI Stage 1–3) | Primary determinant of need for dialysis |
| Electrolytes | Hyperkalaemia, hyperphosphataemia, metabolic acidosis | Urgent correction if severe |
| Coagulation (PT/aPTT/Fibrinogen) | Usually normal or mildly deranged | If markedly abnormal → consider DIC |
| ADAMTS13 activity | >10% in HUS (may be mildly reduced) | <10% = TTP — different emergency treatment pathway |
| C3 / C4 | C3 ↓ in aHUS (especially Factor H, Factor I, C3, Factor B mutations); C4 usually normal | Supports complement-mediated aHUS; normal C3 does not exclude aHUS |
Management
Management of HUS depends critically on the subtype. STEC-HUS requires primarily supportive care, while aHUS mandates early complement inhibition.
STEC-HUS: Supportive Management
Fluid & Electrolyte Management
- Pre-HUS phase (during diarrhoeal prodrome): Aggressive oral rehydration is recommended. Some evidence suggests early, vigorous intravenous fluid resuscitation during the diarrhoeal prodrome may reduce the severity of subsequent HUS by maintaining renal perfusion. Consider 0.9% NaCl 20 mL/kg bolus followed by 1.5–2× maintenance if oliguric or dehydrated.
- Anuric phase: Restrict fluids to insensible losses (400 mL/m²/day) plus urine output. Avoid fluid overload — pulmonary oedema is a major cause of death in paediatric HUS.
- Electrolytes: Treat hyperkalaemia aggressively (calcium gluconate, insulin-dextrose, resonium). Correct metabolic acidosis with sodium bicarbonate if pH <7.1.
Renal Replacement Therapy (RRT)
Indications for dialysis in STEC-HUS include:
- Refractory hyperkalaemia (>6.5 mmol/L despite medical management)
- Fluid overload with pulmonary oedema or refractory hypertension
- Severe metabolic acidosis (pH <7.1) unresponsive to bicarbonate
- Uraemic symptoms (encephalopathy, pericarditis, bleeding)
- Persistent oligoanuria >48 hours with rising creatinine
Peritoneal dialysis (PD) is the preferred modality in children, particularly in infants, as it is well tolerated and does not require vascular access. PD catheter insertion may be performed at the bedside by experienced paediatric surgeons. Haemodialysis (HD) or continuous renal replacement therapy (CRRT) are used when PD is contraindicated or unavailable.
Blood Product Support
- Packed red blood cells (pRBCs): Transfuse if Hb <60 g/L or symptomatic anaemia. Avoid excessive transfusion to prevent fluid overload. Irradiated and CMV-safe products preferred in paediatric patients.
- Platelets: Do NOT transfuse platelets prophylactically — platelets are consumed in microthrombi and may worsen TMA. Reserve platelet transfusion for active life-threatening haemorrhage or pre-operative (e.g., PD catheter insertion) if platelets <30 × 10⁹/L.
Antihypertensive Management
Hypertension is common in HUS and may be volume-dependent or renin-mediated:
- First-line: fluid removal via dialysis if volume-overloaded.
- Pharmacotherapy: amlodipine (0.1–0.3 mg/kg/day PO, max 10 mg/day) or nifedipine (0.25–0.5 mg/kg/dose SL for hypertensive urgency). Enalapril (0.1 mg/kg/day PO) if renin-mediated hypertension.
- PBS: Amlodipine — General Benefit; Nifedipine — General Benefit; Enalapril — General Benefit.
Atypical HUS: Complement Inhibition
aHUS requires immediate initiation of complement inhibition once TTP and STEC-HUS have been excluded. Do not delay treatment while awaiting genetic results.
Eculizumab (Soliris®)
Ravulizumab (Ultomiris®)
Plasma Therapy in aHUS
Prior to the availability of eculizumab, plasma exchange (PEX) or fresh frozen plasma (FFP) infusion was the standard treatment for aHUS. With the advent of complement inhibitors, plasma therapy is now considered second-line or adjunctive, but remains important in specific scenarios:
- When eculizumab is not immediately available.
- Anti-Factor H antibody-mediated aHUS: PEX combined with immunosuppression (rituximab, mycophenolate) to remove and suppress antibody production.
- Factor H or Factor I mutations: PEX replaces deficient protein (though efficacy is inferior to eculizumab).
- MCP mutations: PEX is generally ineffective (MCP is membrane-bound).
Anti-Factor H Antibody aHUS
This subtype requires a combination approach:
- Plasma exchange: Daily PEX × 5, then taper.
- Immunosuppression: Rituximab (375 mg/m² IV weekly × 4) or mycophenolate mofetil (600 mg/m²/day PO in divided doses) to suppress antibody production.
- Eculizumab: If refractory or relapsing despite PEX + immunosuppression.
Monitoring on Complement Inhibitor Therapy
- Haematological: FBC, LDH, haptoglobin, reticulocytes — weekly during induction, then monthly.
- Renal: Creatinine, eGFR, urine protein:creatinine ratio (uPCR) — weekly during induction, then monthly.
- Complement: CH50 or free C5 level to confirm adequate complement blockade (target CH50 = undetectable).
- Infection surveillance: High index of suspicion for meningococcal disease. Check vaccination status.
- Duration: At least 6–12 months of treatment; consider discontinuation only in patients with MCP mutations or identified trigger (e.g., drug-induced) that has been removed. Genetic counselling for Factor H, Factor I, C3, or Factor B mutations generally recommends lifelong therapy.
Other Therapeutic Considerations
- Anticoagulation: There is no evidence supporting routine anticoagulation (heparin, antiplatelet agents) in HUS. Heparin has been tried historically without benefit and carries bleeding risk.
- Corticosteroids: No established role in STEC-HUS. May have a role in anti-Factor H antibody-mediated aHUS as part of immunosuppressive regimens.
- Dietary management: During acute HUS, appropriate renal diet (potassium and phosphate restriction if anuric). Enteral nutrition is preferred over parenteral where feasible.
Investigations
A systematic diagnostic approach is essential to classify the TMA subtype and guide management. The following investigations should be performed in all patients presenting with suspected HUS:
Risk Stratification & Severity Assessment
Risk stratification in HUS guides the intensity of monitoring, threshold for dialysis, and prognosis:
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of kidney disease, infectious gastroenteritis, and environmental health challenges relevant to HUS epidemiology and outcomes. The following considerations are essential for equitable care.
📚 References
- 1. Karpman D, Loos S, Tati R, Arvidsson I. Haemolytic uraemic syndrome. Journal of Internal Medicine. 2017;281(2):123–148.
- 2. Fakhouri F, Zuber J, Frémeaux-Bacchi V, Loirat C. Haemolytic uraemic syndrome. The Lancet. 2017;390(10095):681–696.
- 3. Australian Government Department of Health. National Notifiable Diseases Surveillance System — Shiga toxin-producing Escherichia coli (STEC) notifications. Canberra: DoH; 2024.
- 4. OzFoodNet Working Group. Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: annual report of the OzFoodNet network, 2021. Communicable Diseases Intelligence. 2023;47.
- 5. Loirat C, Fakhouri F, Ariceta G, et al. An international consensus approach to the management of atypical haemolytic uraemic syndrome in children. Pediatric Nephrology. 2016;31(1):15–39.
- 6. Legendre CM, Licht C, Muus P, et al. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. New England Journal of Medicine. 2013;368(23):2169–2181.
- 7. Rondeau E, Cataland SR, Al-Dakkak I, et al. Eculizumab efficacy and safety in atypical hemolytic uremic syndrome: 8-year follow-up. Nephrology Dialysis Transplantation. 2020;35(Suppl 3):iii521.
- 8. Kavanagh D, Goodship TH, Richards A. Atypical haemolytic uraemic syndrome. British Medical Bulletin. 2006;77–78(1):5–22.
- 9. Pharmaceuticals Benefits Scheme. Eculizumab (Soliris®) — Authority Required for complement-mediated aHUS. Australian Government Department of Health; 2024.
- 10. Pharmaceuticals Benefits Scheme. Ravulizumab (Ultomiris®) — Authority Required for complement-mediated aHUS. Australian Government Department of Health; 2024.
- 11. Wong CS, Mooney JC, Brandt JR, et al. Risk factors for the hemolytic uremic syndrome in children infected with Escherichia coli O157:H7: a multivariable analysis. Clinical Infectious Diseases. 2012;55(1):33–41.
- 12. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Aboriginal and Torres Strait Islander people. Cat. no. PHE 250. Canberra: AIHW; 2023.
- 13. The Royal Australian College of General Practitioners (RACGP). National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people. 3rd edition. Melbourne: RACGP; 2018.
- 14. RHDAustralia (NACCHO and Menzies School of Health Research). Chronic kidney disease management in primary care for Aboriginal and Torres Strait Islander people. 4th edition. Darwin: RHDAustralia; 2020.
- 15. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2024. Available at: immunisationhandbook.health.gov.au.