📋 Key Information Summary
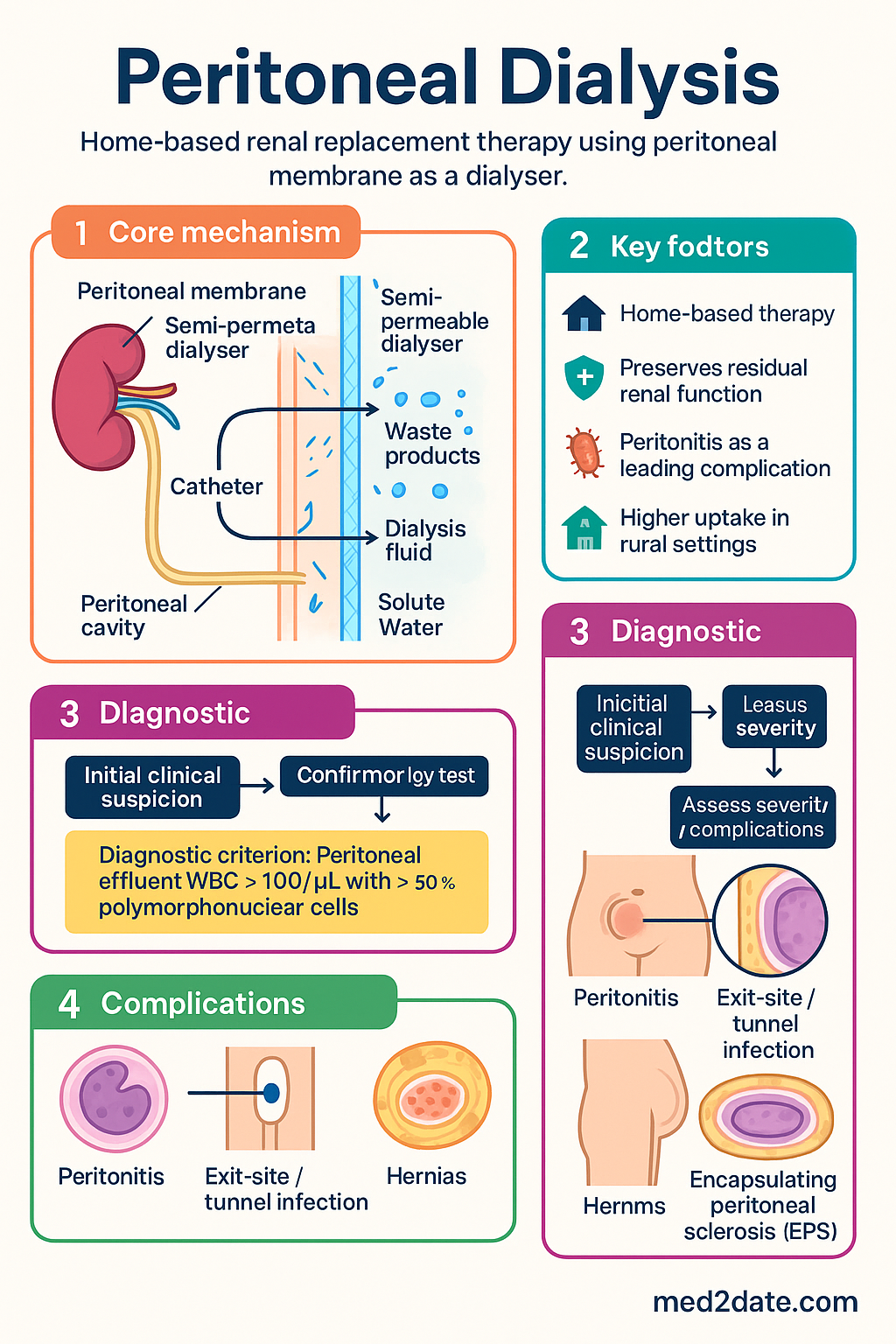
- Peritoneal dialysis (PD) uses the peritoneal membrane as a semipermeable dialyser, enabling home-based renal replacement therapy that preserves residual renal function more effectively than facility haemodialysis.
- Two main modalities exist: continuous ambulatory peritoneal dialysis (CAPD) — 4–5 manual exchanges daily, and automated peritoneal dialysis (APD) — overnight cycling with a cycler machine.
- Australia has ~1,900 prevalent PD patients (ANZDATA 2023); PD accounts for ~12% of all dialysis, with higher uptake in rural and remote settings due to home-based delivery.
- Peritonitis remains the leading complication — incidence ~0.22 episodes per patient-year in Australia — and the primary reason for technique failure.
- Coagulase-negative staphylococci and Staphylococcus aureus cause ~60% of peritonitis episodes; Gram-negative and polymicrobial peritonitis are increasing in frequency.
- Peritonitis empiric therapy: intraperitoneal vancomycin (loading dose 30 mg/kg, max 2 g in 1 L bag) PLUS intraperitoneal gentamicin or ceftazidime, adjusted for local antibiogram.
- Dialysis adequacy targets Kt/V ≥ 1.7 weekly for both CAPD and APD; total (residual + PD) Kt/V ≥ 2.0 per week preferred.
- Peritoneal access via Tenckhoff catheter insertion — surgical open technique or laparoscopic placement — with a break-in period of ≥2 weeks before use.
- Exit-site care with daily topical mupirocin (or gentamicin) cream reduces catheter-related infection by up to 50%.
- Cardinal PD complications include peritonitis, exit-site/tunnel infection, hernias, encapsulating peritoneal sclerosis (EPS), and membrane failure.
- Aboriginal and Torres Strait Islander peoples have higher rates of ESKD and PD-related peritonitis; culturally safe training, remote support, and community nursing improve outcomes.
- Pregnancy is feasible on PD with close multidisciplinary monitoring; dialysis prescriptions require frequent modification, and APD may be preferred in later trimesters.
Introduction & Australian Epidemiology
Peritoneal dialysis (PD) is a home-based renal replacement therapy that harnesses the peritoneal membrane — a large (1.7–2.0 m²) serosal surface lining the abdominal cavity — as a biological dialyser. A sterile dialysate is instilled into the peritoneal cavity via a surgically implanted Tenckhoff catheter, and solute clearance occurs via diffusion and convection, while water removal (ultrafiltration) is driven by osmotic gradients created by dextrose or icodextrin.
PD is a well-established modality in Australia and New Zealand. According to the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA 2023), approximately 1,900 patients are on prevalent PD in Australia, representing roughly 12% of the total dialysis population. PD utilisation is disproportionately higher in regional and remote communities where facility haemodialysis access is limited.
Key advantages of PD over facility haemodialysis include: preservation of residual renal function, dietary and fluid flexibility, reduced need for vascular access, greater patient autonomy, and comparable survival outcomes in the first 2–4 years (particularly in non-diabetic patients). The two principal modalities — continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis (APD) — offer flexibility to suit lifestyle, transport, and clinical requirements.
Principles: CAPD vs APD
Mechanisms of Solute and Water Transport
PD relies on two fundamental transport processes:
- Diffusion: Solutes move down concentration gradients across the peritoneal membrane. Small molecules (urea, potassium, creatinine) equilibrate quickly; larger molecules (β₂-microglobulin) clear more slowly.
- Ultrafiltration (UF): Osmotic agents in dialysate — dextrose (1.36%, 2.27%, 3.86%) or icodextrin 7.5% — draw water into the peritoneal cavity. Net UF depends on dwell time, membrane transport status (PET category), and lymphatic absorption.
Continuous Ambulatory Peritoneal Dialysis (CAPD)
CAPD involves 4–5 manual exchanges per day with dwell times of 4–6 hours during the day and a single overnight dwell of 8–10 hours. Each exchange uses 1.5–3 L of dialysate.
Automated Peritoneal Dialysis (APD)
APD uses a cycler machine to deliver multiple short exchanges overnight (6–10 h). During the day, the patient may remain "dry" (tidal mode) or carry a day dwell (continuous cycling PD / CCPD). APD is the most common PD modality in Australia (~65% of PD patients).
CAPD vs APD — Comparative Overview
| Feature | CAPD | APD |
|---|---|---|
| Exchanges | 4–5 manual | 5–9 overnight (cycler) |
| Day freedom | 4 h dwell in situ | Dry or single day dwell |
| Equipment | Minimal (bags, stand) | Cycler, power supply, storage |
| Cost (PBS) | Lower consumable cost | Higher consumable + cycler hire |
| Solute clearance | Adequate for most | Superior small-molecule clearance |
| Peritoneal membrane | High transporters less suited | Better for high transporters |
| Lifestyle | Flexible daytime | Free days; tied to cycler nights |
| Peritonitis risk | Similar (exposure to open exchanges) | Similar (closed system, fewer connections) |
Peritoneal Equilibration Test (PET)
The PET stratifies patients by membrane transport characteristics using a 2.27% dextrose exchange with 4-hour dwell. Dialysate-to-plasma creatinine ratio (D/P Cr) at 4 hours classifies transporters:
- High: D/P Cr ≥ 0.81 — rapid solute equilibration; benefits from short dwell APD
- High-average: D/P Cr 0.65–0.80
- Low-average: D/P Cr 0.50–0.64
- Low: D/P Cr < 0.50 — slow equilibration; suits CAPD with long dwells
A standard PET should be performed at 4–6 weeks post-initiation and repeated annually or when adequacy declines.
Peritoneal Access & Catheter Placement
Tenckhoff Catheter
The straight or coiled double-cuff Tenckhoff catheter is the standard PD access device in Australia. Cuffs (Dacron felt) promote tissue ingrowth and anchor the catheter subcutaneously, providing a bacterial barrier.
Insertion Techniques
| Technique | Details | Advantages |
|---|---|---|
| Surgical (open) | Mini-laparotomy, direct vision placement | Most common in Australia; precise positioning |
| Laparoscopic | Under direct camera vision ± omentopexy | Hernia repair concurrent; reduced catheter migration |
| Peritoneoscopic | Needle-guided trocar insertion | Minimally invasive; local anaesthesia |
| Image-guided | Fluoroscopic-assisted placement | Rescue for malpositioned catheters |
Pre-Operative Preparation
- Nasal Staphylococcus aureus decolonisation: mupirocin nasal ointment 2% BID for 5 days pre-procedure (reduces S. aureus exit-site infection by 60–80%)
- Peri-operative antibiotics: single-dose IV first-generation cephalosporin (cefazolin 2 g IV) or vancomycin 1 g IV if MRSA colonised
- Bowel preparation: routine use is centre-dependent; some recommend low-residue diet + stool softeners
- Bladder decompression: ensure patient voids or insert catheter pre-operatively to reduce bowel/bladder injury risk
- Pre-operative PET not required — perform after break-in
Break-In Period & Initial Exchanges
- Minimum 2-week healing period before routine PD use (reduce pericatheter leak)
- Day 0–14: flush-and-fill with 500–1,000 mL heparinised saline (500 U/L) 2–3 times per week (or daily), draining immediately — this trains the patient while avoiding intraperitoneal pressure
- If urgent dialysis needed before break-in completes, low-volume APD (1–1.5 L) may be attempted with caution
- Avoid constipation (stool softeners, macrogol) — straining increases hernia and catheter migration risk
Exit-Site Care
Daily exit-site care with topical antibiotic cream is a standard of care in Australia:
- First-line: Mupirocin 2% cream applied to exit site daily (reduces exit-site infection by ~50%)
- Alternative: Gentamicin 0.1% cream if mupirocin resistance suspected
- Keep exit site dry; cover with sterile dressing post-shower until healed
- Secure catheter to avoid traction; use a catheter belt
Peritonitis: Diagnosis & Management
Peritonitis is the most common serious complication of PD and the leading cause of catheter loss and transfer to haemodialysis. The International Society for Peritoneal Dialysis (ISPD) 2022 guidelines and Australian PD unit protocols form the basis of management.
Diagnostic Criteria
Peritonitis is diagnosed when at least two of the following are present:
- Clinical features: abdominal pain, cloudy effluent, fever, nausea/vomiting
- Peritoneal effluent WBC > 100/μL (or > 0.1 × 10⁹/L) with ≥ 50% polymorphonuclear cells
- Positive effluent culture (may be negative in 15–20% of cases)
Specimen Collection
- Obtain effluent sample before administering antibiotics
- Send for cell count (WBC, differential), Gram stain, culture (aerobic + anaerobic), and sensitivity
- Use blood culture bottles: inoculate 10 mL effluent into each of aerobic and anaerobic bottles at bedside (increases culture yield by ~20%)
- If cloudy effluent with negative culture, consider fungal culture, TB culture, unusual organisms, or chemical peritonitis
Causative Organisms — Australian Patterns
| Organism Category | Common Organisms | Approximate % |
|---|---|---|
| Gram-positive cocci | Coagulase-negative staphylococci (CNS), S. aureus, Streptococcus spp. | 45–55% |
| Gram-negative bacilli | E. coli, Klebsiella, Pseudomonas, Proteus | 20–30% |
| Polymicrobial | Mixed flora (consider bowel perforation) | 10–15% |
| Fungal | Candida spp., Aspergillus | 3–5% |
| Culture-negative | — | 15–20% |
Empiric Antibiotic Therapy
Commence empiric antibiotics immediately after effluent collection. In Australia, ISPD 2022–compliant regimens use intraperitoneal (IP) delivery as standard:
Directed Therapy (Post-Culture)
| Organism | Directed Treatment | Duration |
|---|---|---|
| CNS (methicillin-sensitive) | Cephazolin 1 g IP daily (or oral cephalexin if mild) | 14 days total |
| CNS (methicillin-resistant) | Vancomycin IP (continue current regimen) | 14 days total |
| S. aureus (MSSA) | Flucloxacillin 2 g IV TDS or cephazolin 1 g IP daily | 21 days (check for tunnel infection) |
| S. aureus (MRSA) | Vancomycin IP | 21 days |
| Pseudomonas aeruginosa | Ceftazidime 1 g IP daily + oral ciprofloxacin 500 mg BD | 21 days (dual therapy) |
| Enterococcus spp. | Ampicillin 125 mg/L IP (or IV 1 g TDS) ± gentamicin | 14 days |
| Polymicrobial | Broaden per sensitivities; CT abdomen if bowel perforation suspected | 14–21 days |
| Fungal (Candida spp.) | Catheter removal + fluconazole 200 mg PO daily or amphotericin B IP | Catheter removal is essential |
Catheter Removal Indications
- Refractory peritonitis: no clinical improvement after 5 days of appropriate antibiotics
- Relapsing peritonitis (same organism within 4 weeks of completing therapy)
- Fungal peritonitis — remove catheter immediately
- Concurrent exit-site/tunnel infection (refractory or S. aureus)
- Bowel perforation with peritonitis
- Recurrent peritonitis (>3 episodes)
Exit-Site & Tunnel Infection
Defined by purulent or serous discharge ± erythema at the catheter exit site; tunnel infection involves tenderness/erythema along the subcutaneous tunnel.
- Swab discharge for culture before starting treatment
- Empiric: oral cephalexin 500 mg QID or flucloxacillin 500 mg QID (MSSA); add oral rifampicin 300 mg BD if MRSA suspected
- Pseudomonas: oral ciprofloxacin 500 mg BD ± IP ceftazidime
- Consider catheter removal if no response at 2–3 weeks or concurrent peritonitis
Adequacy & Complications
Dialysis Adequacy Assessment
PD adequacy is measured by urea clearance (Kt/V) and creatinine clearance (CrCl), normalised to body water and body surface area respectively. Targets are set by ISPD and adapted in Australian PD units:
| Parameter | CAPD Target | APD Target |
|---|---|---|
| Weekly Kt/V (PD alone) | ≥ 1.7 | ≥ 1.7 |
| Weekly Kt/V (total: PD + residual) | ≥ 2.0 (preferred) | ≥ 2.0 (preferred) |
| Weekly CrCl (L/1.73 m²) | ≥ 50 L | ≥ 60 L (if residual function present) |
| Ultrafiltration | ≥ 750 mL/day (clinically) | ≥ 750 mL/day |
| Anuria threshold | UUV < 200 mL/day | UUV < 200 mL/day |
Prescription Modification for Inadequate Clearance
- Increase fill volume (e.g. 2.0 → 2.5 L per exchange)
- Add an extra exchange (CAPD: 4 → 5 exchanges)
- For APD: increase cycle number, use tidal mode, add a daytime exchange
- Use icodextrin for long dwells to improve UF without dextrose load
- Preserve residual renal function: avoid nephrotoxins (NSAIDs, aminoglycosides systemically), avoid hypotension
- If anuric and Kt/V remains below target despite maximising prescription, consider transfer to haemodialysis
Complications of PD
Membrane Failure
Peritoneal membrane failure may manifest as:
- Loss of ultrafiltration (< 400 mL/4h with 3.86% dextrose)
- High transporter status on repeat PET (D/P Cr > 0.81) — suggests membrane damage
- Inadequate solute clearance despite maximal prescription
Options: modify prescription (shorter dwells, icodextrin), add APD, or consider conversion to haemodialysis or renal transplantation.
Nutritional Considerations
- Protein intake: 1.0–1.2 g/kg/day (higher than HD due to peritoneal losses of 5–15 g/day protein + amino acids)
- Energy intake: 25–35 kcal/kg/day (including dextrose absorbed from dialysate)
- Potassium: generally liberal unless hyperkalaemic (PD removes potassium)
- Sodium restriction: 80–100 mmol/day for volume management
- Phosphate: dietary restriction + phosphate binders (sevelamer, lanthanum, calcium carbonate — PBS-listed)
- Regular dietitian review (minimum 6-monthly)
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience end-stage kidney disease (ESKD) at rates approximately 7–10 times higher than non-Indigenous Australians (AIHW 2023). PD is an important modality in remote and very remote communities where facility haemodialysis is unavailable or requires relocation to urban centres, causing significant social and cultural disruption.
Key Considerations
📚 References
- 1. Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). 46th Annual Report 2023. Adelaide: ANZDATA; 2023.
- 2. Li PKT, Chow KM, Cho Y, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Peritoneal Dialysis International. 2022;42(2):110–153.
- 3. Li PKT, Chow KM, Van de Luijtgaarden MWM, et al. Changes in the worldwide epidemiology of peritoneal dialysis. Nature Reviews Nephrology. 2017;13(2):90–103.
- 4. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 229. Canberra: AIHW; 2023.
- 5. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th ed. Melbourne: Kidney Health Australia; 2020.
- 6. Remote Area Health Corps / RHDAustralia. Remote Dialysis Handbook: Peritoneal Dialysis. Darwin: RHDAustralia; 2022.
- 7. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 8. Boudville N, Kemp A, Clayton P, et al. Recent peritonitis associates with mortality among patients treated with peritoneal dialysis. Journal of the American Society of Nephrology. 2012;23(8):1398–1405.
- 9. Cho Y, Boudville N, Palmer SC, et al. Practice of peritoneal dialysis catheter flushing in Australia and New Zealand: multi-centre cross-sectional survey. Nephrology. 2018;23(2):167–173.
- 10. Johnson DW, Brown FG, Clarke M, et al. Effects of biocompatible versus standard fluid on peritoneal dialysis outcomes. Journal of the American Society of Nephrology. 2012;23(6):1097–1107.
- 11. Korte MR, Sampimon DE, Betjes MG, Krediet RT. Encapsulating peritoneal sclerosis: the state of affairs. Nature Reviews Nephrology. 2011;7(9):528–538.
- 12. McDonald SP, Russ GR. Burden of end-stage renal disease among indigenous peoples in Australia and New Zealand. Kidney International Supplements. 2003;(83):S123–S127.
- 13. Radhakrishnan J, Remuzzi G, Saran R, et al. Taming the chronic kidney disease epidemic: a global view of surveillance efforts. Kidney International. 2014;86(2):246–250.
- 14. National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking Alcohol. Canberra: NHMRC; 2020.
- 15. Ranganathan D, John GT, Jose M, et al. Australian peritoneal dialysis outcomes: a multicentre study. Nephrology. 2021;26(10):802–810.