📋 Key Information Summary
- Radiocontrast nephropathy (RCN), also termed contrast-induced acute kidney injury (CI-AKI), is defined as a rise in serum creatinine (sCr) ≥26.5 µmol/L within 48 hours or a ≥50% increase within 7 days of iodinated contrast administration, after excluding other causes.
- Pre-existing chronic kidney disease (eGFR <60 mL/min/1.73 m²) is the single strongest risk factor; risk increases proportionally with declining renal function.
- Diabetes mellitus, particularly with concurrent CKD, dehydration, heart failure (EF <40%), nephrotoxic drug exposure (NSAIDs, aminoglycosides, ACE inhibitors), and large contrast volumes are major independent risk factors.
- The Mehran score is the most validated pre-procedural risk-scoring tool; a score ≥16 confers >25% risk of CI-AKI and >12% risk of requiring dialysis.
- Isotonic intravenous crystalloid (0.9% sodium chloride or balanced crystalloid such as Plasma-Lyte 148®) at 1–1.5 mL/kg/hr for 6–12 hours pre- and post-procedure is the single most evidence-based prevention strategy.
- Use the lowest effective dose of low-osmolar (iohexol, iopamidol) or iso-osmolar (iodixanol) contrast; a contrast volume >100 mL or a contrast volume/eGFR ratio >1.1 significantly raises CI-AKI risk.
- N-acetylcysteine (NAC, Mucomyst®) 1200 mg PO BD for 48 hours (2 doses pre + 2 post) is widely used in Australian practice; evidence is mixed (AMACING, PRESERVE trials) but the safety profile and low cost support continued use in high-risk patients.
- Avoid nephrotoxic agents (NSAIDs, aminoglycosides) for ≥48 hours before and after contrast exposure where clinically feasible.
- Withhold metformin for 48 hours post-contrast if eGFR <30 mL/min/1.73 m² or if CI-AKI develops, to prevent metformin-associated lactic acidosis (MALA).
- Serum creatinine should be measured at baseline, 48 hours, and 5–7 days post-contrast; early detection of CI-AKI enables prompt nephrology referral.
- Consider alternative imaging (MRI without gadolinium, ultrasound, low-dose CT without contrast) when the risk of CI-AKI outweighs diagnostic benefit.
- Aboriginal and Torres Strait Islander patients have disproportionately higher rates of CKD and diabetes, placing them at elevated CI-AKI risk; culturally safe counselling and point-of-care eGFR testing in remote settings are essential.
- Most CI-AKI is self-limiting (nadir sCr at day 3–5, recovery by day 7–10), but severe cases can cause tubular necrosis requiring temporary dialysis and are associated with increased long-term cardiovascular events and mortality.
Introduction & Australian Epidemiology
Radiocontrast nephropathy (RCN), increasingly referred to as contrast-induced acute kidney injury (CI-AKI), represents the third most common cause of hospital-acquired AKI after hypoperfusion and nephrotoxic medications. It is defined as an acute decline in renal function occurring within 48 hours of intravascular iodinated contrast administration, in the absence of an alternative aetiology.
In Australia, approximately 80 million diagnostic imaging and interventional procedures involving iodinated contrast are performed annually across public and private sectors. With the ageing population and rising burden of chronic kidney disease (CKD) — affecting an estimated 1.7 million Australians (AIHW, 2023) — the population at risk of CI-AKI continues to expand. The incidence of CI-AKI varies from 2–5% in patients with normal renal function to 20–50% in those with pre-existing CKD complicated by diabetes.
CI-AKI carries significant clinical and economic consequences. It is associated with prolonged hospital stays (median 3–7 additional days), increased in-hospital mortality (adjusted OR 4.0–6.0 for dialysis-requiring CI-AKI), and accelerated progression of CKD to end-stage kidney disease (ESKD). Australian data from the ANZDATA registry and state-based hospital morbidity datasets indicate that CI-AKI contributes to approximately 10–15% of AKI episodes requiring renal replacement therapy in metropolitan centres.
This guideline provides an evidence-based framework for risk assessment, prevention, diagnosis, and management of CI-AKI in the Australian healthcare setting, aligned with National Safety and Quality Health Service (NSQHS) Standards, the Kidney Disease: Improving Global Outcomes (KDIGO) 2024 update, and Australian Therapeutic Guidelines.
Pathophysiology & Risk Factors
Pathophysiology
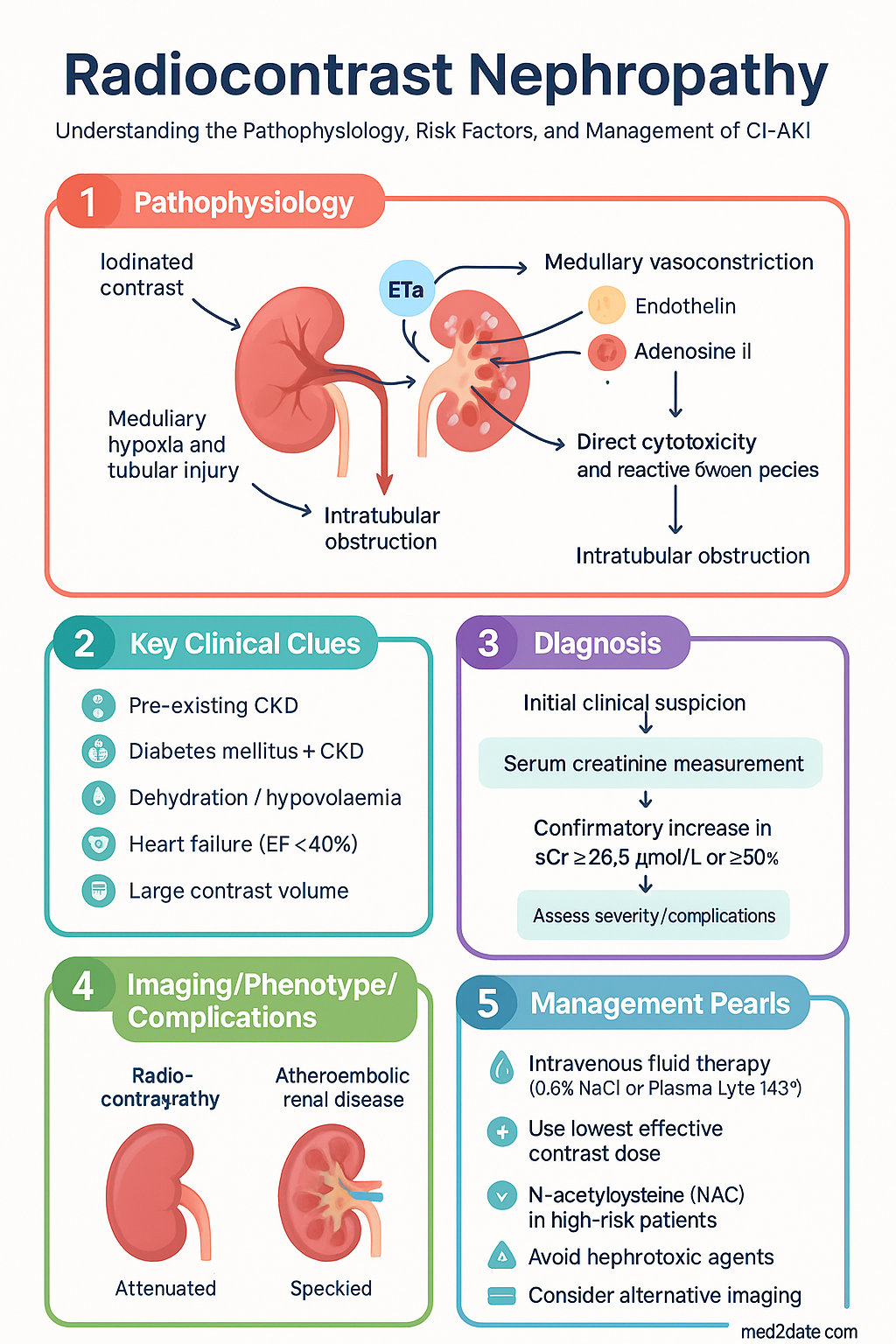
CI-AKI results from the synergistic interaction of three principal mechanisms affecting the renal medulla, which is normally operating at the hypoxic threshold (pO₂ 10–20 mmHg):
- Medullary vasoconstriction: Iodinated contrast triggers an initial transient vasodilation followed by sustained vasoconstriction of the vasa recta via endothelin, adenosine, and angiotensin II, reducing medullary blood flow by up to 50%.
- Medullary hypoxia and tubular injury: Contrast-induced increases in oxygen consumption (from active tubular reabsorption of the osmotic load) combined with reduced delivery create severe regional hypoxia, leading to proximal tubular epithelial cell vacuolisation, apoptosis, and necrosis — a pattern termed osmotic nephropathy with iohexol and tubular necrosis with high-dose iodixanol.
- Direct cytotoxicity and reactive oxygen species (ROS): Contrast media directly generate superoxide and hydroxyl radicals, causing peroxidation of membrane lipids, mitochondrial dysfunction, and complement activation within tubular cells.
- Intratubular obstruction: Precipitation of Tamm–Horsfall mucoprotein with contrast in the distal nephron contributes to intratubular cast formation and obstruction, particularly in dehydrated states.
Major Risk Factors
| Risk Factor | Mechanism / Notes | Relative Risk |
|---|---|---|
| Pre-existing CKD (eGFR <60) | Reduced medullary reserve, impaired contrast excretion | 5.5–15× |
| Diabetes mellitus + CKD | Microvascular disease amplifies medullary ischaemia | 8–20× |
| Dehydration / hypovolaemia | Increased contrast viscosity in tubular lumen, enhanced vasoconstriction | 3–5× |
| Heart failure (EF <40%) | Reduced renal perfusion, RAAS activation | 3–4× |
| Contrast volume >100 mL | Dose-dependent nephrotoxicity | 2–5× |
| Contrast volume/eGFR ratio >1.1 | Stronger predictor than absolute volume alone | 4–6× |
| Age >70 years | Declining nephron mass, comorbidity burden | 2–3× |
| Concurrent nephrotoxins (NSAIDs, aminoglycosides) | Additive tubular injury | 2–4× |
| Multiple myeloma | Light-chain precipitation with contrast | Variable |
| Previous CI-AKI episode | Residual nephron loss | 6–10× |
Mehran Risk Score for CI-AKI
The Mehran score assigns points to pre-procedural variables to stratify risk prior to percutaneous coronary intervention (PCI) or other intra-arterial contrast procedures. It has also been validated for intravenous contrast studies.
| Variable | Points |
|---|---|
| Hypotension (SBP <80 mmHg requiring inotropes ≥1 hr) | 5 |
| Intra-aortic balloon pump | 5 |
| CHF (EF <40% or pulmonary oedema) | 5 |
| Age >75 years | 4 |
| Anaemia (Hct <39% M, <36% F) | 3 |
| Diabetes mellitus | 3 |
| Contrast volume (per 100 mL) | 1 per 100 mL |
| eGFR 40–60 | 2 |
| eGFR 20–39 | 4 |
| eGFR <20 or dialysis | 6 |
Prevention Strategies
Intravenous Fluid Therapy — First-Line Prevention
The PRESERVE trial (N Engl J Med 2018) demonstrated that sodium bicarbonate was not superior to sodium chloride, and NAC was not superior to placebo, for prevention of CI-AKI. However, balanced crystalloid showed non-inferiority to normal saline with potential advantage regarding acid–base balance. Australian practice typically uses either 0.9% NaCl or Plasma-Lyte 148® based on local availability.
N-Acetylcysteine (NAC)
Contrast Agent Selection & Volume Minimisation
- Low-osmolar contrast media (LOCM): Iohexol (Omnipaque®), iopamidol (Isovue®) — standard of care in Australia; lower nephrotoxicity than high-osmolar agents.
- Iso-osmolar contrast media (IOCM): Iodixanol (Visipaque®) — iso-osmolar with plasma; may offer marginal advantage in diabetic CKD (NEPHRIC trial); higher viscosity requires slower injection rates.
- Volume minimisation: Target contrast volume <100 mL where feasible. Calculate the maximum safe volume using the formula: Safe volume (mL) = 5 × body weight (kg) / sCr (mg/dL), or use the contrast volume/eGFR ratio target of <1.1.
- Low-dose protocols: Use low-kVp CT angiography (80–100 kVp), automated tube current modulation, and iterative reconstruction algorithms to reduce contrast volume by 30–50%.
Agents to Withhold or Avoid
- Metformin: Withhold for 48 hours post-contrast if eGFR <30 mL/min/1.73 m² or if CI-AKI develops. Resume only after renal function confirmed stable. Risk: metformin-associated lactic acidosis (MALA) in setting of AKI.
- NSAIDs: Cease ≥24 hours pre-contrast and avoid for ≥48 hours post-contrast. Risk: additive vasoconstriction, prostaglandin inhibition reduces medullary perfusion.
- ACE inhibitors / ARBs: Consider withholding on the day of procedure in high-risk patients (eGFR <30, volume-depleted). Evidence is mixed; the RAAS blockade removal reduces efferent arteriolar tone and may reduce GFR acutely. Restart when euvolaemic and creatinine stable.
- Aminoglycosides: Avoid concurrent administration; if essential, ensure therapeutic drug monitoring and aggressive hydration.
- SGLT2 inhibitors: Withhold ≥3 days pre-contrast due to euglycaemic DKA risk in setting of reduced oral intake/procedural fasting.
Agents NOT Recommended for CI-AKI Prevention
- Sodium bicarbonate infusion — no superiority over NaCl 0.9% in PRESERVE trial; not routinely recommended.
- Furosemide or mannitol — potentially harmful (volume depletion); contraindicated.
- Dopamine or fenoldopam — no benefit; not recommended by KDIGO.
- Theophylline / aminophylline — inconsistent evidence; not routinely recommended.
- Ascorbic acid (Vitamin C) — small trials insufficient to support routine use.
- Statins — some evidence of pleiotropic anti-inflammatory effect; not yet standard of care for CI-AKI prevention alone.
Diagnosis & Clinical Course
Diagnostic Criteria (KDIGO 2024)
CI-AKI is diagnosed when any of the following occur within 48 hours of contrast exposure, after excluding other causes:
- Absolute increase in serum creatinine ≥26.5 µmol/L (≥0.3 mg/dL) within 48 hours, OR
- Relative increase in serum creatinine ≥50% (1.5× baseline) within 7 days, OR
- Urine output <0.5 mL/kg/hr for ≥6 hours (in context of known contrast exposure)
Typical Clinical Course
Investigations
Management
Acute Management of Established CI-AKI
Post-Discharge Follow-Up
- Recheck serum creatinine and eGFR at 1 week and 3 months post-discharge.
- If eGFR remains <60 mL/min/1.73 m², establish ongoing CKD management with GP and consider nephrology follow-up.
- Document CI-AKI episode prominently in medical records and My Health Record (if patient-consented) to alert future treating clinicians.
- Educate patient regarding risk of recurrence with future contrast exposure; provide written alert card.
- Restart previously withheld medications (metformin, ACEi/ARB, SGLT2i) only after confirming stable renal function (≥48 hrs of stable creatinine).
- Screen for progression to CKD at 3 months using ACR (albumin-to-creatinine ratio) and eGFR.
Special Populations
ATSI Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of chronic kidney disease, diabetes, and cardiovascular disease — all major risk factors for contrast-induced acute kidney injury. The AIHW reports that ATSI Australians are 2.5 times more likely to have CKD and 3.8 times more likely to develop ESKD than non-Indigenous Australians. These disparities demand specific attention in CI-AKI risk assessment and prevention.
📚 References
- 1. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney International Supplements. 2024;14(1):S1–S144. doi:10.1016/j.kisu.2024.01.001.
- 2. Weisbord SD, Gallagher M, Jneid H, et al. Outcomes after angiography with sodium bicarbonate and acetylcysteine (PRESERVE). N Engl J Med. 2018;378(7):603–614. doi:10.1056/NEJMoa1710933.
- 3. Nijssen EC, Rennenberg RJ, Nelemans PJ, et al. Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING). Lancet. 2017;389(10076):1312–1322. doi:10.1016/S0140-6736(17)30057-0.
- 4. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention. J Am Coll Cardiol. 2004;44(7):1393–1399. doi:10.1016/j.jacc.2004.06.068.
- 5. Aspelin P, Aubry P, Fransson SG, et al. Nephrotoxicity in high-risk patients study of iso-osmolar and low-osmolar nonionic contrast media (NEPHRIC). N Engl J Med. 2003;348(6):491–499. doi:10.1056/NEJMoa021833.
- 6. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 228. Canberra: AIHW; 2023.
- 7. Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). 46th Annual Report 2023. Adelaide: SA Health and Medical Research Institute; 2023.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 9. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 10th ed. East Melbourne: RACGP; 2024.
- 10. Kidney Health Australia. Chronic kidney disease (CKD) management in primary care. 4th ed. Melbourne: Kidney Health Australia; 2020.
- 11. Subramaniam RM, Wilson RF, Engelmann T, et al. ACR Manual on Contrast Media. Version 2024. Reston, VA: American College of Radiology; 2024.
- 12. van der Molen AJ, Reimer P, Dekkers IA, et al. Post-contrast acute kidney injury — Part 1: Definition, clinical features, incidence, role of contrast medium and risks. Eur Radiol. 2018;28(7):2845–2855. doi:10.1007/s00330-017-5246-5.