📋 Key Information Summary
- Primary membranous nephropathy (MN) is the most common cause of nephrotic syndrome in non-diabetic Caucasian adults aged 40–60 years
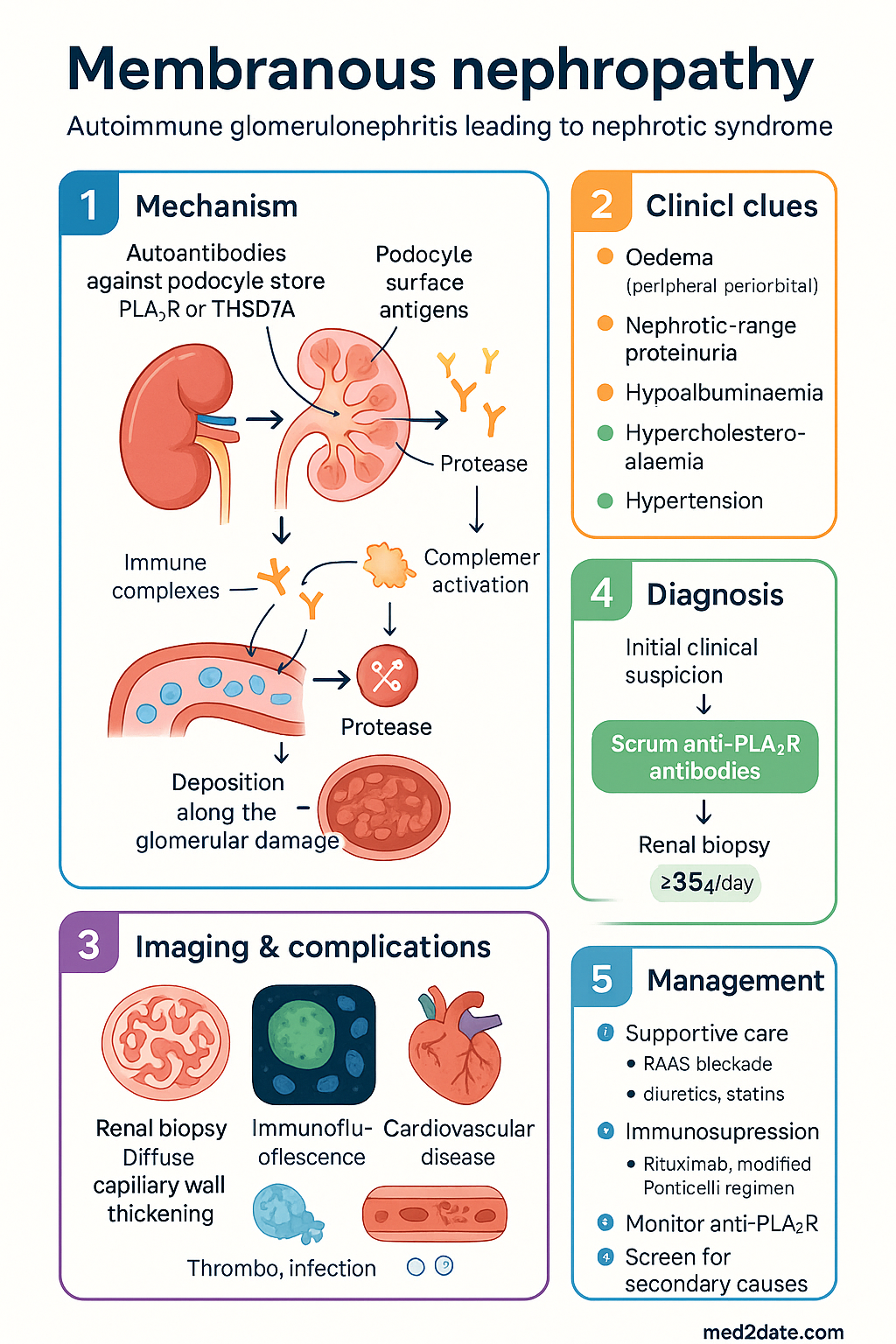
- Anti-PLA2R antibodies are detectable in ~70–80% of primary MN and are both diagnostic and prognostic; anti-THSD7A antibodies account for a further 3–5%
- Clinical presentation: insidious nephrotic syndrome (oedema, heavy proteinuria >3.5 g/day, hypoalbuminaemia, hypercholesterolaemia)
- The classic "Rule of Thirds": ~⅓ spontaneous remission, ⅓ persistent proteinuria, ⅓ progressive to ESKD over 10 years
- All patients require supportive care with RAAS blockade, diuretics, SGLT2 inhibitors, and statins regardless of immunosuppression decision
- Immunosuppressive therapy is indicated for patients at high risk of progressive disease per the KDIGO risk algorithm (persistent proteinuria >3.5 g/day despite 6 months supportive therapy)
- Rituximab has emerged as a preferred first-line immunosuppressive agent, supported by the MENTOR trial, replacing the older Ponticelli regimen in many centres
- The modified Ponticelli regimen (alternating corticosteroids + cyclophosphamide over 6 months) remains an effective alternative where rituximab is unavailable or contraindicated
- Calcineurin inhibitors (tacrolimus, ciclosporin) are second-line options; cyclophosphamide is PBS Authority Required for nephrotic syndrome
- Anti-PLA2R antibody titre correlates with disease activity — serial monitoring guides treatment response and relapse detection
- Renal biopsy remains the gold standard: shows diffuse capillary wall thickening with sub-epithelial immune complex deposits; immunofluorescence shows granular IgG4 ± C3
- Thromboembolism risk is significantly elevated in MN — consider prophylactic anticoagulation if albumin <25 g/L
- Screen for secondary causes (malignancy, autoimmune disease, hepatitis B/C, medications) in all patients before diagnosing primary MN
- Aboriginal and Torres Strait Islander peoples may present later, have reduced access to specialist nephrology care, and require culturally safe management pathways
Introduction & Australian Epidemiology
Primary membranous nephropathy (MN) is an autoimmune glomerulonephritis characterised by the formation of immune complexes along the glomerular basement membrane (GBM), resulting in thickening of the capillary wall and progressive podocyte injury. It is the leading cause of nephrotic syndrome in non-diabetic Caucasian adults and the second most common primary glomerulopathy diagnosed on renal biopsy in Australia after IgA nephropathy.
The discovery of anti-phospholipase A2 receptor (PLA2R) antibodies in 2009 revolutionised the understanding and management of primary MN, providing a serological biomarker for diagnosis, prognostication, and treatment monitoring. Subsequent identification of anti-thrombospondin type-1 domain-containing 7A (THSD7A) antibodies has further refined the immunopathological classification.
Australian Epidemiology
- Incidence in Australia: estimated at 8–12 per million population per year, with higher rates in Caucasian populations
- Peak incidence: 40–60 years of age; male-to-female ratio approximately 2:1
- Primary MN accounts for approximately 20–25% of all nephrotic syndrome biopsies in Australian adults
- The Australia and New Zealand Dialysis and Transplant (ANZDATA) Registry reports MN as a significant contributor to incident ESKD, though outcomes have improved with modern immunosuppression
- Secondary MN (related to malignancy, lupus, hepatitis B, medications) must be excluded in all cases — particularly important given the higher burden of hepatitis B in Aboriginal and Torres Strait Islander communities
- Anti-PLA2R antibody testing is available through major Australian pathology services (Sullivan Nicolaides, Douglass Hanly Moir, SA Pathology) and is MBS-rebatable
Pathophysiology — PLA2R & THSD7A Antibodies
Anti-PLA2R Antibodies
The M-type phospholipase A2 receptor (PLA2R) is a transmembrane glycoprotein expressed on the surface of glomerular podocytes. In approximately 70–80% of primary MN cases, IgG4 autoantibodies target the PLA2R antigen, forming sub-epithelial immune complexes in situ. This is distinct from secondary MN, where immune complexes are typically deposited from the circulation.
- Antigen: PLA2R — a 185 kDa transmembrane receptor belonging to the mannose receptor family
- Antibody subclass: Predominantly IgG4 (pathognomonic); IgG1 and IgG3 may co-exist and may indicate more active disease
- Target epitopes: Multiple epitope domains have been identified (CysR, CTLD1, CTLD7); epitope spreading is associated with disease persistence and poorer prognosis
- Mechanism: Anti-PLA2R IgG4 binds podocyte surface PLA2R → complement-independent podocyte injury (C5b-9 membrane attack complex may play a secondary role) → loss of glomerular permselectivity → proteinuria
- Genetic associations: HLA-DQA1 polymorphism confers susceptibility; environmental triggers (infections, malignancy) may initiate autoimmune response in genetically predisposed individuals
Anti-THSD7A Antibodies
Anti-thrombospondin type-1 domain-containing 7A (THSD7A) antibodies account for a further 3–5% of primary MN cases that are PLA2R-negative. THSD7A is also a transmembrane protein expressed on podocytes.
- Antigen: THSD7A — a 250 kDa transmembrane protein
- Antibody subclass: IgG4 (predominantly)
- Clinical significance: THSD7A-positive MN is associated with a higher incidence of concurrent or subsequent malignancy — thorough cancer screening is mandatory
- Mechanism: Similar in situ immune complex formation as PLA2R-mediated MN
Immune Complex Formation & Complement Activation
The pathogenic sequence in primary MN involves:
- Autoantibody production against podocyte surface antigens (PLA2R or THSD7A)
- In situ sub-epithelial immune complex formation along the GBM
- Activation of the complement cascade — primarily via the lectin pathway and C5b-9 membrane attack complex
- Podocyte injury and effacement of foot processes
- Loss of glomerular permselectivity leading to heavy proteinuria
- GBM thickening from immune complex incorporation ("spike" appearance on silver stain)
- Progressive podocyte depletion and tubulointerstitial fibrosis in advanced disease
Clinical Features & Natural History — Rule of Thirds
Clinical Presentation
Primary MN typically presents insidiously with the full nephrotic syndrome, though the degree of proteinuria varies considerably at presentation. Key clinical features include:
- Oedema: Peripheral, periorbital, and/or generalised (anasarca in severe cases) — often the presenting complaint
- Proteinuria: Nephrotic-range (>3.5 g/day or >200 mg/mmol on urine PCR) — may be sub-nephrotic at presentation in some cases
- Hypoalbuminaemia: Serum albumin <30 g/L (often <20 g/L in severe nephrotic syndrome)
- Hypercholesterolaemia: Due to hepatic lipoprotein synthesis in response to hypoalbuminaemia
- Frothy urine: Due to heavy proteinuria
- Haematuria: Microscopic haematuria in ~30% of cases; gross haematuria is uncommon and should prompt consideration of other diagnoses
- Hypertension: Present in approximately 30–50% at diagnosis
- Renal function: Often preserved at presentation; declining eGFR suggests advanced or progressive disease
The Classic "Rule of Thirds"
The natural history of untreated primary MN is classically described by the "Rule of Thirds":
Complications
- Thromboembolism: MN confers the highest thrombotic risk among glomerulonephritides. Renal vein thrombosis occurs in ~10–30%; pulmonary embolism in ~5–10%. Risk is highest when serum albumin <25 g/L
- Infection: Urinary tract infections, peritonitis (in ascites), and spontaneous bacterial peritonitis due to immunoglobulin loss and oedema
- Cardiovascular disease: Accelerated atherosclerosis from dyslipidaemia; volume overload
- Acute kidney injury: May occur from severe intravascular volume depletion, intercurrent illness, or use of nephrotoxic agents
- Malignancy: MN may be a paraneoplastic phenomenon — screen for malignancy especially in THSD7A-positive and older patients
Investigations
Laboratory Investigations
Secondary Cause Screening
| Category | Tests | Notes |
|---|---|---|
| Autoimmune | ANA, dsDNA, anti-Smith, C3/C4 | Lupus nephritis class V; both ANA and dsDNA positive → consider lupus |
| Infection | Hepatitis B (HBsAg, anti-HBc, HBV DNA), Hepatitis C (anti-HCV, HCV RNA) | Especially important in ATSI populations |
| Malignancy | Age-appropriate cancer screening (CT chest/abdomen/pelvis, colonoscopy if age >50) | Mandatory in THSD7A-positive, age >65, or clinical suspicion |
| Medications | Medication review | NSAIDs, gold, penicillamine, captopril, mercury exposure |
Renal Biopsy — Staging (Ehrenreich-Churg)
| Stage | Light Microscopy | Electron Microscopy | Prognosis |
|---|---|---|---|
| I (Early) | Normal GBM thickness; subtle sub-epithelial deposits | Small, discrete sub-epithelial deposits; intact GBM | Best prognosis; most responsive to therapy |
| II (Spike) | GBM thickening; "spike" projections on silver stain | GBM material grows between deposits creating spikes | Good prognosis with treatment |
| III (Dome) | GBM surrounds deposits; "dome" appearance | Deposits incorporated within GBM | Moderate; partial response to immunosuppression |
| IV (Sclerosis) | GBM thickened, lucent deposits, sclerosis | Lucent, degraded deposits; GBM irregularly thickened | Poor prognosis; irreversible damage |
Management
KDIGO Risk Stratification
Treatment decisions in MN follow the KDIGO 2021 algorithm, which categorises patients into risk groups based on proteinuria and eGFR trajectory:
Supportive / Conservative Therapy
All patients with MN — regardless of immunosuppression decision — require comprehensive supportive care:
- RAAS blockade: ACE inhibitor (e.g. perindopril 4–8 mg PO daily) or ARB (e.g. irbesartan 150–300 mg PO daily). Titrate to maximum tolerated dose. Reduces proteinuria by 30–50% and controls blood pressure.
- SGLT2 inhibitor: Dapagliflozin 10 mg PO daily (Forxiga®) — now PBS-listed for CKD regardless of diabetes status. Reduces proteinuria and slows CKD progression (DAPA-CKD, EMPA-KIDNEY trials).
- Diuretics: Loop diuretics (furosemide 20–80 mg PO daily) for oedema management. Combination with thiazide for resistant oedema.
- Statin: Atorvastatin 10–40 mg PO daily or rosuvastatin 5–20 mg PO daily for dyslipidaemia. PBS General Benefit.
- Anticoagulation: Consider prophylactic warfarin (INR 2.0–2.5) or LMWH if serum albumin <25 g/L with additional risk factors
- Sodium restriction: <2 g/day sodium intake
- Dietary protein: Avoid high-protein diets; aim for 0.8 g/kg/day unless malnourished
- Pneumococcal and influenza vaccination: Annual influenza; pneumococcal (Prevenar 13 then Pneumovax 23)
First-Line Immunosuppression — Rituximab
Rituximab has emerged as the preferred first-line immunosuppressive agent for moderate-to-high risk primary MN, based on the landmark MENTOR trial (Fervenza et al., 2019) and subsequent GEMRITUX trial.
Alternative Immunosuppression — Modified Ponticelli Regimen
The modified Ponticelli regimen (alternating corticosteroids with alkylating agent) remains an effective alternative, particularly where rituximab is unavailable, contraindicated, or unaffordable.
Second-Line & Adjunctive Agents
Treatment Response Criteria
| Response | Definition | Significance |
|---|---|---|
| Complete remission | uPCR <50 mg/mmol (proteinuria <0.3 g/day) × 2 consecutive measurements | Best long-term renal outcome; 10-year renal survival >95% |
| Partial remission | uPCR 50–350 mg/mmol (0.3–3.5 g/day) with >50% reduction from peak | Good prognosis; 10-year renal survival ~80–90% |
| No response | <50% reduction in proteinuria after 6 months of therapy | Consider alternative agent or second-line therapy |
| Relapse | uPCR returns to >350 mg/mmol after prior complete/partial remission | May require re-treatment with rituximab or alternative agent |
Anti-PLA2R Guided Treatment Monitoring
Serial anti-PLA2R antibody titres are now the cornerstone of treatment monitoring in primary MN:
- Check anti-PLA2R at baseline, then every 3 months during and after treatment
- Serological remission (PLA2R negativity) typically precedes clinical remission by 6–12 months
- Rising PLA2R titres after treatment cessation predict clinical relapse — consider pre-emptive re-treatment
- Persistent high titres despite therapy may indicate treatment-resistant disease; consider switching agent
- In PLA2R-negative MN, rely on proteinuria and eGFR for monitoring
Relapsed or Refractory Disease
- First relapse after rituximab: Re-induction with rituximab 1000 mg × 2 doses; most patients respond to re-treatment
- Rituximab-refractory: Consider switch to modified Ponticelli regimen or combination rituximab + low-dose ciclosporin
- Cyclophosphamide-refractory: Rituximab is the preferred alternative
- Maintenance therapy: Some centres use low-dose rituximab (500 mg every 6 months) as maintenance in relapsing patients
- Novel agents: Ongoing clinical trials with ofatumumab (anti-CD20), obinutuzumab, and complement inhibitors (iptacopan, narsoplimab) show promise
Special Populations
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander peoples experience a higher burden of kidney disease compared to non-Indigenous Australians, with glomerulonephritis contributing significantly to the disparity. While membranous nephropathy is less common than IgA nephropathy or diabetic kidney disease in ATSI populations, specific considerations apply:
📚 References
- 1. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International. 2021;100(4S):S1–S276.
- 2. Fervenza FC, Appel GB, Barbour SJ, et al. Rituximab or Cyclosporine in the Treatment of Membranous Nephropathy. New England Journal of Medicine. 2019;381(1):36–46. (MENTOR Trial)
- 3. Beck LH Jr, Bonegio RGB, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. New England Journal of Medicine. 2009;361(1):11–21.
- 4. Tomas NM, Beck LH Jr, Meyer-Schwesinger C, et al. Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy. New England Journal of Medicine. 2014;371(24):2277–2287.
- 5. Dahan K, Debiec H, Plaisier E, et al. Rituximab for Severe Membranous Nephropathy: A 6-Center Trial. Journal of the American Society of Nephrology. 2017;28(8):2509–2518. (GEMRITUX Trial)
- 6. Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney International. 2021;100(4):753–779.
- 7. Ponticelli C, Zucchelli P, Passerini P, et al. A 10-year follow-up of a randomized study with methylprednisolone and chlorambucil in membranous nephropathy. Kidney International. 1995;48(5):1600–1604.
- 8. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 221. Canberra: AIHW; 2023.
- 9. Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). 46th Annual Report. Adelaide: ANZDATA; 2023.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 11. Fernandez-Juarez G, Rojas-Rivera J, Logt AV, et al. The STARMEN trial indicates that alternating treatment with corticosteroids and cyclophosphamide is superior to sequential treatment with tacrolimus and rituximab in primary membranous nephropathy. Kidney International. 2021;99(4):986–998.
- 12. Ponticelli C, Glassock RJ. Glomerular diseases: membranous nephropathy — A modern view. Clinical Journal of the American Society of Nephrology. 2014;9(3):609–616.