📋 Key Information Summary
- Idiopathic hypercalciuria (IH) is defined as urinary calcium excretion >7.5 mmol/day (men) or >6.25 mmol/day (women) on a normal calcium diet, in the absence of identifiable secondary causes such as hyperparathyroidism, sarcoidosis, or malignancy.
- IH is the most common metabolic abnormality detected in patients with calcium oxalate and calcium phosphate nephrolithiasis, present in approximately 40–60% of recurrent stone formers in Australia.
- Three subtypes — absorptive (Type I and II), renal leak, and resorptive — differ in mechanism and have distinct management implications; absorptive Type I is the most prevalent.
- Nephrocalcinosis (NC) denotes diffuse calcium salt deposition within the renal parenchyma, distinguished from nephrolithiasis by imaging characteristics on ultrasound or CT.
- Medullary nephrocalcinosis accounts for >95% of cases and is most often associated with distal renal tubular acidosis, medullary sponge kidney, and IH; cortical NC is rare and suggests chronic glomerular disease, oxalosis, or cortical necrosis.
- A properly collected 24-hour urine collection (ideally two separate collections) is the cornerstone of metabolic evaluation, measuring calcium, oxalate, citrate, urate, sodium, phosphate, volume, and creatinine (for adequacy check).
- First-line lifestyle modification for all subtypes is a low-sodium diet (<6 g NaCl/day or <100 mmol Na/day), adequate fluid intake (>2.5 L/day), and normal calcium intake (1,000–1,200 mg/day) — restriction of dietary calcium paradoxically increases stone risk.
- Thiazide diuretics (hydrochlorothiazide, indapamide, chlorthalidone) are the first-line pharmacotherapy for IH, reducing urinary calcium by 30–50% by enhancing proximal and distal tubular reabsorption.
- Thiazides require concurrent potassium or potassium-sparing agent supplementation to prevent hypokalaemia, which itself reduces urinary citrate and promotes stones.
- ATSI Australians have a rising prevalence of nephrolithiasis linked to dietary transition, remote healthcare access limitations, and higher rates of chronic kidney disease — all factors that alter management priorities.
- Paediatric IH presenting with nephrocalcinosis requires specialist nephrology referral; thiazides may be used in children but monitoring of growth, electrolytes, and bone density is essential.
- Patients with nephrocalcinosis warrant ongoing surveillance with renal ultrasound and annual estimated glomerular filtration rate (eGFR) to detect progressive parenchymal damage.
Introduction & Australian Epidemiology
Idiopathic hypercalciuria (IH) is the most common metabolic risk factor for calcium oxalate and calcium phosphate kidney stones. It is characterised by excessive urinary calcium excretion in the absence of identifiable secondary causes such as primary hyperparathyroidism, granulomatous disease, vitamin D excess, or malignancy. Nephrocalcinosis refers to diffuse deposition of calcium salts within the renal parenchyma, as distinct from nephrolithiasis, which describes discrete calculi within the collecting system.
Australian context: Kidney stones affect approximately 10–15% of the Australian population over a lifetime, with an age-standardised incidence of approximately 150 per 100,000 person-years. Calcium-containing stones (calcium oxalate and calcium phosphate) account for over 75% of all urinary calculi analysed in Australian laboratories. IH is identified in 40–60% of recurrent calcium stone formers referred to nephrology or urology clinics. Hospitalisation rates for urinary stone disease are highest in men aged 30–60 years and are increasing, particularly in tropical and subtropical regions of Queensland and the Northern Territory, where chronic dehydration contributes to supersaturation.
Nephrocalcinosis, though less common than nephrolithiasis, carries greater prognostic significance because parenchymal calcium deposition may lead to progressive tubulointerstitial fibrosis, impaired concentrating ability, and chronic kidney disease. Medullary nephrocalcinosis is far more common than cortical nephrocalcinosis and is associated with distal renal tubular acidosis (dRTA), medullary sponge kidney, and IH. The prevalence of nephrocalcinosis in paediatric populations is estimated at 0.5–1.7% by renal ultrasound screening.
This guideline reviews the classification, investigation, and evidence-based management of IH and nephrocalcinosis, with emphasis on Australian prescribing practices, Pharmaceutical Benefits Scheme (PBS) access, and Indigenous health considerations.
Pathophysiology
Calcium homoeostasis depends on the interplay of intestinal absorption, renal tubular reabsorption, and skeletal turnover. In IH, one or more of these pathways is dysregulated, leading to elevated filtered calcium load or impaired tubular recovery. The pathophysiology differs by subtype:
- Intestinal hyperabsorption: Enhanced active transcellular calcium transport (mediated by TRPV6 channels and calbindin-D9k in duodenal enterocytes) increases fractional calcium absorption to >30% (normal ~20%). This elevates serum ionised calcium, suppresses parathyroid hormone (PTH), increases filtered calcium load, and may decrease proximal tubular phosphate reabsorption, causing mild hypophosphataemia and secondary 1,25-dihydroxyvitamin D elevation.
- Renal calcium leak: A primary defect in distal tubular calcium reabsorption (TRPV5 channel dysfunction or claudin-14 dysregulation) leads to obligatory hypercalciuria. Compensatory secondary hyperparathyroidism maintains serum calcium but further increases bone turnover and urinary calcium.
- Bone resorption (resorptive): Increased osteoclast-mediated calcium release from bone (distinct from hyperparathyroidism) contributes to the filtered load. This subtype overlaps with osteoporosis and may respond poorly to thiazides alone.
Regardless of the initiating mechanism, hypercalciuria increases urinary supersaturation with respect to calcium oxalate and calcium phosphate. Supersaturation drives nucleation, crystal growth, and aggregation — the prerequisites for stone formation. In nephrocalcinosis, crystals deposit within the tubular lumen and interstitium of the medulla, triggering an inflammatory cascade (NALP3 inflammasome activation, osteopontin and Tamm–Horsfall protein deposition) that culminates in fibrosis.
Types of Idiopathic Hypercalciuria
Although historically divided into absorptive, renal, and resorptive subtypes based on calcium-loading (fasting and calcium-supplemented) tests, most Australian centres now rely on 24-hour urine biochemistry and serum profiles for pragmatic classification.
| Subtype | Mechanism | Serum Ca²⁺ | Serum PTH | 24h Urine Ca | Fasting Urine Ca | Prevalence |
|---|---|---|---|---|---|---|
| Absorptive Type I | Primary intestinal hyperabsorption | Normal–high | Low–normal | Markedly elevated | Normal | ~50–60% of IH |
| Absorptive Type II | Intestinal hyperabsorption (diet-modifiable) | Normal | Normal | Elevated on normal diet; normalises on low-Ca diet | Normal | ~15–20% of IH |
| Renal Leak | Primary renal tubular Ca²⁺ wasting | Normal–low | Elevated (secondary) | Elevated | Elevated | ~15–20% of IH |
| Resorptive | Bone Ca²⁺ release (non-PTH) | Normal–high | Low–normal | Elevated | Elevated | ~5–10% of IH |
Absorptive Type I (Classic)
The most common and clinically significant subtype. Patients exhibit hypercalciuria on both normal and restricted calcium diets. Serum calcium is normal to high-normal; PTH is suppressed or low-normal. Fractional calcium absorption (if measured) exceeds 30%. These patients are typically resistant to dietary calcium restriction alone and usually require thiazide therapy.
Absorptive Type II (Diet-Modifiable)
Hypercalciuria is present on a normal calcium diet but normalises when dietary calcium is restricted to 400 mg/day. This form is managed primarily with dietary modification. Importantly, both Type I and Type II respond to reduced sodium intake, which lowers the filtered calcium load.
Renal Leak Hypercalciuria
A primary defect in renal tubular calcium reabsorption results in obligatory urinary calcium loss regardless of intake. Secondary hyperparathyroidism develops to maintain serum calcium but perpetuates the leak. Thiazides are particularly effective in this subtype because they directly enhance distal tubular calcium reabsorption.
Resorptive Hypercalciuria
Least common subtype; involves increased skeletal calcium mobilisation independent of PTH. Patients may have concurrent osteopaenia or osteoporosis. Investigation should exclude myeloma, immobilisation, thyrotoxicosis, and Paget disease. Treatment may require bone-protective agents (bisphosphonates) in addition to thiazides.
Investigations & 24-Hour Urine Collection
Metabolic evaluation is indicated for all patients with recurrent calcium stones (≥2 episodes), a single stone with high-risk features (solitary kidney, renal transplant, paediatric age), or nephrocalcinosis on imaging.
Baseline Serum Investigations
24-Hour Urine Collection — The Cornerstone
Two separate 24-hour urine collections (ideally 4–6 weeks apart while the patient is on their usual diet) are recommended to improve reliability. Collections must be performed on an unrestricted diet and fluid intake.
| Parameter | Normal Range | Relevance |
|---|---|---|
| Urinary calcium | <7.5 mmol/day (M)<br><6.25 mmol/day (F) | Diagnosis of IH; targets for therapy |
| Urinary oxalate | <0.5 mmol/day | Identifies concurrent hyperoxaluria |
| Urinary citrate | >2.5 mmol/day (M); >3.0 mmol/day (F) | Hypocitraturia promotes crystallisation |
| Urinary urate | <4.0 mmol/day | Urate promotes CaOx nucleation |
| Urinary sodium | <200 mmol/day (ideally <100) | High Na⁺ intake directly increases urinary Ca²⁺ |
| Urinary phosphate | 15–50 mmol/day | Phosphaturia in absorptive IH |
| Urinary volume | >2.5 L/day | Inadequate volume is the most common preventable risk factor |
| Urinary creatinine | ≥8.8 mmol/day (M); ≥6.6 mmol/day (F) | Adequacy check — collection invalid if below threshold |
Stone Composition Analysis
Infrared spectroscopy or X-ray diffraction of passed or retrieved stones is essential. Australian pathology laboratories (e.g., Douglass Hanly Moir, Sullivan Nicolaides, Laverty) routinely perform stone analysis at no out-of-pocket cost through Medicare. Calcium oxalate monohydrate (whewellite), calcium oxalate dihydrate (weddellite), and calcium phosphate (apatite, brushite) have distinct risk profiles and therapeutic implications.
Imaging
Clinical Presentation & Diagnostic Criteria
Idiopathic Hypercalciuria
Most patients with IH are asymptomatic until they develop their first kidney stone episode, typically presenting with:
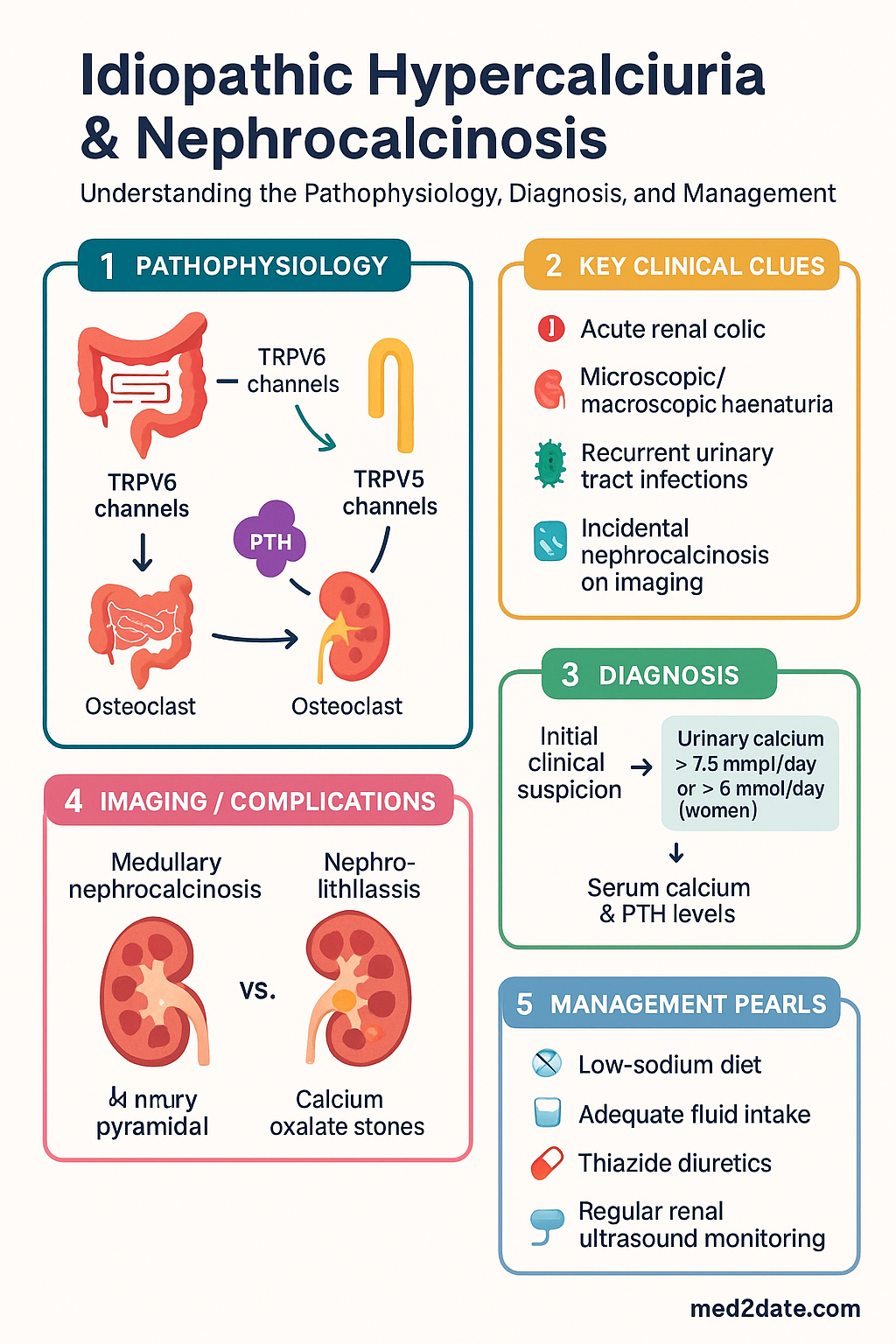
- Acute renal colic — severe, colicky flank pain radiating to the groin or labia/testis, often with nausea and haematuria
- Microscopic or macroscopic haematuria
- Recurrent urinary tract infections (staghorn calculi may predispose)
- Incidental nephrocalcinosis or urolithiasis on imaging
In children, IH may present with haematuria (macroscopic or microscopic), dysuria, abdominal pain, or failure to thrive. Haematuria alone, without stone passage, may be the only manifestation in paediatric patients.
Diagnostic Criteria for IH
IH is a diagnosis of exclusion. The following criteria apply:
- 24-hour urinary calcium excretion above the upper limit of normal on at least two collections, on a normal diet (>7.5 mmol/day in men, >6.25 mmol/day in women, or >0.1 mmol/kg/day in children)
- Normal serum calcium (corrected for albumin)
- Absence of secondary causes (hyperparathyroidism, sarcoidosis, malignancy, vitamin D excess, thyrotoxicosis, immobilisation, distal RTA, frusemide use)
Nephrocalcinosis
Nephrocalcinosis is typically an imaging diagnosis. Patients may be asymptomatic or present with:
- Polyuria and polydipsia (impaired urinary concentrating ability from tubulointerstitial injury)
- Renal colic or stone passage
- Haematuria
- Progressive chronic kidney disease (in advanced cases)
- Metabolic alkalosis or acidosis depending on the underlying aetiology
On ultrasound, nephrocalcinosis appears as hyperechoic medullary pyramids (medullary form) or increased cortical echogenicity (cortical form). Non-contrast CT demonstrates high-attenuation foci (>200 Hounsfield units) within the parenchyma.
Nephrocalcinosis: Medullary vs Cortical
Nephrocalcinosis is classified by the anatomical location of calcium deposition within the kidney. This distinction has important aetiological and prognostic implications.
Medullary Nephrocalcinosis (>95% of cases)
Calcium deposits are confined to the renal medulla — specifically the loops of Henle, vasa recta, and collecting ducts. The medullary interstitium is supersaturated due to countercurrent multiplication, acidic pH, and high local concentrations of calcium and phosphate.
| Aetiology | Key Features |
|---|---|
| Distal renal tubular acidosis | Hyperchloremic metabolic acidosis, alkaline urine, hypercalciuria, hypocitraturia. Most common cause of medullary NC in children. Can be primary or secondary (Sjögren syndrome, SLE, amphotericin B). |
| Medullary sponge kidney | Cystic dilatation of medullary collecting ducts; bilateral in >70% of cases. Often presents in 30–50-year-olds with recurrent stones and NC. Diagnosed by IVU or CT urogram (brush-like blush of contrast in medullary pyramids). |
| Idiopathic hypercalciuria | The most common cause in adults. Medullary supersaturation drives intratubular crystal deposition. |
| Primary hyperparathyroidism | Hypercalcaemia + hypercalciuria → medullary calcium deposition. Important exclusion (treatable cause). |
| Papillary necrosis | Diabetes, NSAIDs, sickle cell disease/trait. Calcified necrotic papillae simulate NC on imaging. |
| Hyperoxaluria (primary or enteric) | Oxalate crystallisation in medulla. Enteric hyperoxaluria occurs after bariatric surgery, small bowel resection, or malabsorption states. |
| Bartter and Gitelman syndromes | Inherited tubulopathies. Bartter: hypokalaemic metabolic alkalosis, hypercalciuria, NC. Gitelman: hypocalciuria, hypomagnesaemia (typically no NC). |
| Prematurity | Up to 40% of preterm neonates develop transient medullary NC, usually resolving by age 2 years. Associated with frusemide therapy and low phosphate intake. |
Cortical Nephrocalcinosis (Rare)
Calcium deposition within the renal cortex. This is a distinct entity with a more limited differential and generally worse prognosis, as it reflects irreversible cortical damage.
- Acute cortical necrosis — post-partum haemorrhage, septic shock, snakebite, HELLP syndrome. Diffuse cortical calcification develops weeks to months after the acute insult.
- Chronic glomerulonephritis — end-stage kidneys may develop cortical calcification.
- Primary hyperoxaluria — Type 1 (AGXT deficiency) and Type 2 (GRHPR deficiency). Systemic oxalosis may deposit in cortex, bones, retina, myocardium, and vessels.
- Alport syndrome and chronic allograft nephropathy
Risk Stratification
Not all patients with IH or a single stone event require the same intensity of investigation or treatment. Risk stratification guides the metabolic work-up and therapy intensity.
Management
Management of IH and nephrocalcinosis is multimodal, combining dietary modification (first-line for all patients), pharmacotherapy (for moderate-to-high-risk patients), and surveillance. The overarching goals are to reduce urinary calcium excretion, decrease urinary supersaturation, prevent further stone formation, and slow nephrocalcinosis progression.
Dietary & Lifestyle Modification
Pharmacotherapy — Thiazide Diuretics
Thiazide diuretics are the first-line pharmacotherapy for IH. They enhance calcium reabsorption in the distal convoluted tubule (via the NCC transporter and downstream effects on TRPV5 channels), reducing urinary calcium by 30–50%. Thiazides also reduce bone turnover and may improve bone mineral density.
Potassium-Sparing Agents & Supplements
Second-Line & Adjunctive Agents
Management Algorithm Summary
Monitoring
Long-term monitoring is essential to assess treatment efficacy, detect adverse drug effects, and identify progressive nephrocalcinosis or CKD.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Worcester EM, Coe FL. Clinical practice. Calcium kidney stones. N Engl J Med. 2010;363(10):954–963.
- 2. Gambaro G, Croppi E, Coe F, et al. Metabolic diagnosis and medical prevention of calcium nephrolithiasis and its systemic manifestations: a consensus statement. J Nephrol. 2016;29(6):715–734.
- 3. Curhan GC, Willett WC, Knight EL, Stampfer MJ. Dietary factors and the risk of incident kidney stones in younger women: Nurses' Health Study II. Arch Intern Med. 2004;164(8):885–891.
- 4. Fink HA, Akornor JW, Garimella PS, et al. Diet, fluid, or supplements for secondary prevention of nephrolithiasis: a systematic review and meta-analysis of randomized trials. Eur Urol. 2009;56(1):72–80.
- 5. Australian Institute of Health and Welfare (AIHW). Kidney disease in Australia. Cat. no. PHE 229. Canberra: AIHW; 2021.
- 6. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th edn. East Melbourne: RACGP; 2024.
- 7. Sayer JA, Carr G, Simmons NL. Nephrocalcinosis: molecular insights from calcium crystallisation in the kidney. Clin Sci (Lond). 2020;134(12):1489–1506.
- 8. Pak CY, Poindexter JR, Adams-Huet B, Pearle MS. Predictive value of kidney stone composition in the detection of metabolic abnormalities. Am J Med. 2003;115(1):26–32.
- 9. Escribano J, Balaguer A, Pagone F, Roqué i Figuls M, Feliu A. Pharmacological interventions for preventing complications in idiopathic hypercalciuria. Cochrane Database Syst Rev. 2009;(1):CD004754.
- 10. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020.
- document.querySelectorAll('.topic-toc a[href^="#"]').forEach(o=>{o.addEventListener("click",i=>{const t=o.getAttribute("href")||"",e=document.querySelector(t);if(!e)return;i.preventDefault();const n=e.getBoundingClientRect().top+window.scrollY-70;window.scrollTo({top:n,behavior:"smooth"}),history.replaceState(null,"",t)})});const r=new Map;document.querySelectorAll(".topic-toc a").forEach(o=>{const i=o.getAttribute("href")?.slice(1);i&&r.set(i,o)});if(r.size>0&&"IntersectionObserver"in window){const o=new IntersectionObserver(i=>{let t=null;for(const e of i)if(e.isIntersecting){t=e.target.id;break}t&&r.forEach((e,n)=>e.classList.toggle("active",n===t))},{rootMargin:"-80px 0px -40% 0px",threshold:0});r.forEach((i,t)=>{const e=document.getElementById(t);e&&o.observe(e)})}window.matchMedia("(max-width: 900px)").matches&&document.querySelector(".topic-rail-collapsible")?.removeAttribute("open");const c=document.querySelector(".topic-rail-details");function s(){c&&(window.matchMedia("(max-width: 900px)").matches?c.open=!1:c.open=!0)}s();let l;window.addEventListener("resize",()=>{clearTimeout(l),l=window.setTimeout(s,120)});