📋 Key Information Summary
- Acute interstitial nephritis (AIN) accounts for approximately 15–27% of unexplained acute kidney injury (AKI) cases in Australian hospital settings and is frequently underdiagnosed.
- Drugs are the most common aetiology in adults, responsible for 70–80% of cases — proton-pump inhibitors (PPIs), NSAIDs, and antibiotics (penicillins, cephalosporins, trimethoprim) are the leading culprits.
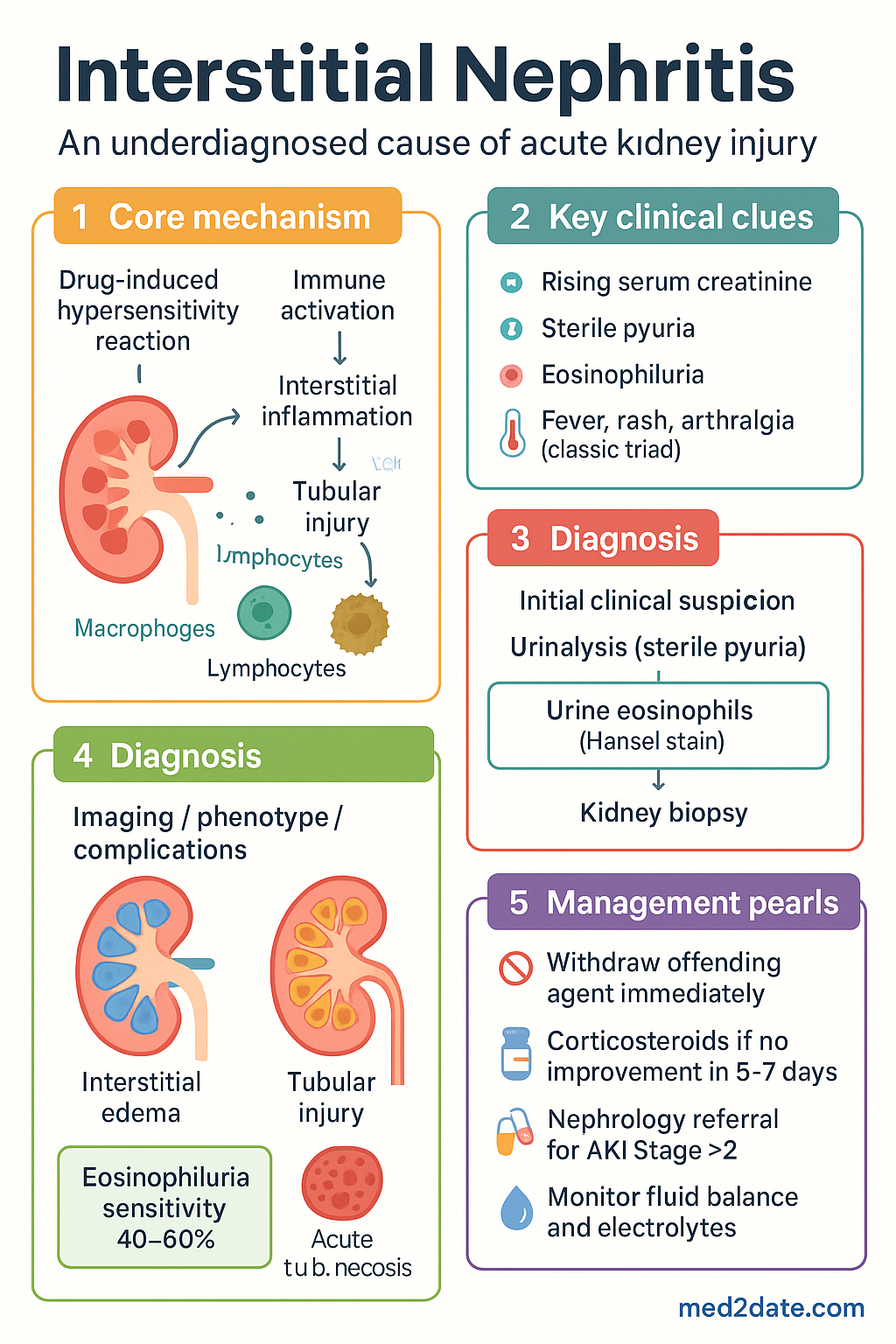
- The classic triad is: (1) rising serum creatinine, (2) sterile pyuria, and (3) eosinophiluria — though the full triad is present in fewer than one-third of cases.
- Early identification and withdrawal of the offending agent is the single most important management step; delays correlate with increased risk of chronic kidney disease (CKD).
- Urine eosinophils (Hansel stain preferred over Wright stain) are supportive but not pathognomonic; the sensitivity of urine eosinophiluria is approximately 40–60%.
- Kidney biopsy remains the gold standard for diagnosis when the clinical picture is uncertain or when there is no improvement after drug withdrawal.
- Corticosteroids are indicated in drug-induced AIN where renal function fails to recover within 5–7 days of offending agent cessation.
- Typical corticosteroid regimen: prednisolone 0.5–1 mg/kg/day (max 60 mg) orally for 2–4 weeks, followed by a taper over 4–6 weeks.
- Infectious AIN (bacterial pyelonephritis, leptospirosis, CMV) requires treatment of the underlying infection rather than immunosuppression.
- Sarcoid-associated and IgG4-related tubulointerstitial nephritis are important immune-mediated causes requiring specialist rheumatology/nephrology co-management.
- Nephrology referral is indicated for all patients with AIN and AKI Stage ≥2 (KDIGO criteria), biopsy-proven disease, or when dialysis may be required.
- Aboriginal and Torres Strait Islander peoples have higher rates of renal disease generally; consider AIN in the differential of unexplained AKI in remote settings where polypharmacy is common.
Introduction & Australian Epidemiology
Acute interstitial nephritis (AIN) is an inflammatory disorder of the renal tubulointerstitium characterised by interstitial oedema, tubular injury, and infiltration by inflammatory cells — predominantly lymphocytes, macrophages, eosinophils, and occasionally plasma cells. It is an important and potentially reversible cause of acute kidney injury (AKI).
Historically considered a rare entity, AIN is now recognised as the cause of 15–27% of intrinsic AKI cases in hospital-based cohorts, with autopsy and biopsy series suggesting it is significantly underdiagnosed. The rising incidence parallels increased use of implicated medications, particularly proton-pump inhibitors (PPIs), which have emerged over the past decade as one of the most common offending agents.
In Australia, data from the ANZDATA registry and tertiary centre renal biopsy series (including Westmead Hospital and Royal Adelaide Hospital series) confirm that drug-induced AIN predominates in adult practice, while post-infectious and immune-mediated causes are important in paediatric and immunocompromised populations. The condition affects all age groups but is most common in adults aged 40–75 years, with a slight male predominance (M:F ≈ 1.5:1).
Early recognition and prompt withdrawal of the causative agent are critical, as delayed diagnosis is associated with irreversible tubular atrosis, interstitial fibrosis, and progression to CKD requiring dialysis. This guideline covers the aetiology, clinical features, investigation, and management of AIN in the Australian setting.
Aetiology: Drug-Induced, Infectious, Immune
Drug-Induced AIN (70–80% of cases)
Drug-induced AIN is a type IV (delayed-type) hypersensitivity reaction. It is typically not dose-dependent, may occur after days to months of exposure, and can recur upon re-challenge. The most commonly implicated drug classes in Australia include:
| Drug Class | Examples | Approximate Relative Risk |
|---|---|---|
| Proton-pump inhibitors | Omeprazole, esomeprazole, pantoprazole, lansoprazole | High — now the most common single-class cause |
| Antibiotics | β-lactams (penicillins, cephalosporins), trimethoprim-sulfamethoxazole, fluoroquinolones, rifampicin | High — β-lactams historically the most recognised |
| NSAIDs | Ibuprofen, naproxen, diclofenac, indomethacin, COX-2 inhibitors | Moderate — may also cause minimal-change nephrotic syndrome |
| Diuretics | Thiazides, frusemide, ethacrynic acid | Low–Moderate |
| Anticonvulsants | Carbamazepine, phenytoin, lamotrigine, valproate | Low–Moderate |
| Immune checkpoint inhibitors | Nivolumab, pembrolizumab, ipilimumab | Emerging — checkpoint inhibitor-related nephrotoxicity |
| Other | Allopurinol, 5-ASA (mesalazine), cimetidine, indinavir | Low |
Infectious AIN
Infection-related AIN may result from direct renal parenchymal invasion or immune-mediated injury:
- Bacterial: Escherichia coli, Proteus, Klebsiella (ascending pyelonephritis); Leptospira spp. (tropical regions including northern Australia); Streptococcus (scarlatina-associated AIN); Brucella
- Viral: CMV (especially immunocompromised), HIV-associated nephropathy, hantavirus, polyomavirus (BK virus), Epstein–Barr virus (EBV)
- Fungal: Candida spp., Aspergillus spp. — predominantly in immunosuppressed patients
- Rickettsial: Q fever (Coxiella burnetii) — relevant in rural Australia
- Parasitic: Leishmania, Toxoplasma — imported cases
Immune-Mediated AIN
Systemic autoimmune conditions may present with isolated or predominant tubulointerstitial inflammation:
- Sarcoidosis: Non-caseating granulomatous interstitial nephritis; may cause hypercalcaemia-related renal impairment
- IgG4-related tubulointerstitial nephritis: Part of IgG4-related systemic disease; characteristic storiform fibrosis and IgG4+ plasma cell infiltration on biopsy
- Sjögren syndrome: Tubulointerstitial nephritis in up to 30% of patients, though often subclinical
- Systemic lupus erythematosus: Lupus interstitial nephritis (class III/IV often have interstitial component)
- Tubulointerstitial nephritis with uveitis (TINU) syndrome: Idiopathic; predominantly in young females
Clinical Features & Classic Triad
The Classic Triad
The classic triad of AIN — fever, rash, and arthralgia — was originally described with methicillin-associated AIN. However, the full triad is present in fewer than 10% of contemporary cases. In practice, AIN more commonly presents insidiously with:
- Rising serum creatinine (unexplained AKI) — the most consistent finding
- Sterile pyuria — white blood cells on urine microscopy with negative culture
- Eosinophiluria — present in only 40–60% of cases
Symptoms & Signs
| Feature | Frequency | Notes |
|---|---|---|
| Oliguria / rising creatinine | 80–100% | Usually non-oliguric initially; AKI may progress |
| Sterile pyuria | 70–80% | WBC casts or free WBCs; urine culture negative |
| Fever | 30–50% | May be low-grade; often absent with NSAIDs |
| Maculopapular rash | 15–30% | Typically truncal; coincides with drug exposure |
| Arthralgia | 15–25% | Non-specific; may accompany rash |
| Flank pain | 10–20% | Dull, bilateral; renal capsule stretching |
| Peripheral eosinophilia | 25–40% | Blood eosinophil count >0.5 × 10⁹/L |
| Eosinophiluria | 40–60% | Hansel stain >1% eosinophils of urinary WBCs |
Timing of Onset
Drug-induced AIN typically presents 7–21 days after drug initiation, but may occur within days (antibiotics) or months to years (PPIs, NSAIDs). Re-exposure to a previously offending agent may produce symptoms within 24–48 hours.
Investigations
Laboratory Investigations
Renal Biopsy — Gold Standard
Percutaneous renal biopsy is the definitive diagnostic test and should be performed when:
- Clinical suspicion is high but the diagnosis remains uncertain
- No improvement in renal function 5–7 days after cessation of suspected offending agent
- Immune-mediated aetiology is suspected (sarcoidosis, IgG4-related disease, lupus)
- To exclude alternative diagnoses (ANCA vasculitis, anti-GBM disease, acute tubular necrosis)
| Biopsy Finding | Interpretation |
|---|---|
| Dense interstitial lymphocytic infiltrate (CD4+ and CD8+ T cells) | Most common pattern in drug-induced AIN |
| Eosinophilic infiltrate | Characteristic of drug-induced; may also be seen in parasites |
| Non-caseating granulomas | Sarcoidosis; also consider mycobacterial/fungal infection |
| Storiform fibrosis + IgG4+ plasma cells | IgG4-related tubulointerstitial nephritis |
| Tubulitis (lymphocyte invasion of tubular basement membrane) | Confirms active interstitial inflammation |
| Interstitial fibrosis >50% | Chronicity — poor prognostic indicator; less likely to respond to steroids |
Imaging
- Renal ultrasound: First-line imaging; kidneys may be enlarged with increased echogenicity (oedema). Helps exclude obstruction and assess renal size.
- CT abdomen (non-contrast): If biopsy planned — evaluates kidney position and excludes cystic/mass lesions.
Management: Drug Withdrawal, Steroids
Principle 1: Immediate Withdrawal of Offending Agent
In most drug-induced AIN cases, renal function begins to improve within 5–14 days of drug cessation. If no improvement is seen by day 5–7, corticosteroid therapy should be initiated (see below). Document the offending drug clearly in the patient's allergy/adverse drug reaction list and notify their GP.
Principle 2: Supportive Care
- Fluid balance management — avoid nephrotoxins (contrast, aminoglycosides)
- Electrolyte monitoring and correction (hyperkalaemia, metabolic acidosis)
- Dialysis if indicated — severe AKI Stage 3 (KDIGO), refractory hyperkalaemia, fluid overload, uraemic symptoms
- Medication dose adjustment for renal impairment (renal dosing)
- Blood pressure control; avoid ACEi/ARB during acute phase if haemodynamically unstable
Principle 3: Corticosteroids
Corticosteroids are the mainstay of immunosuppressive therapy for drug-induced AIN when withdrawal of the offending agent alone is insufficient. The optimal timing, dose, and duration remain debated, but the following regimen is consistent with Australian nephrology practice and international consensus:
Intravenous pulse methylprednisolone (500 mg–1 g IV daily for 3 days) may be considered for severe AIN with dialysis-dependent AKI or biopsy showing minimal fibrosis, followed by oral prednisolone taper. This should be initiated in consultation with nephrology.
Principle 4: Management of Specific Aetiologies
| Aetiology | First-Line Treatment | Notes |
|---|---|---|
| Drug-induced AIN | Withdraw offending agent + ± corticosteroids | Steroids if no recovery in 5–7 days |
| Bacterial pyelonephritis | IV antibiotics per culture & sensitivity; ceftriaxone 1–2 g IV daily empirically | Do NOT use corticosteroids |
| Leptospirosis | IV benzylpenicillin 1.2 g 4–6 hourly or IV ceftriaxone 1–2 g daily | Early treatment (within 5 days of onset) reduces complications |
| CMV-related AIN | IV ganciclovir 5 mg/kg 12-hourly or oral valganciclovir 900 mg BD | Immunocompromised patients; adjust for renal function |
| Sarcoid-associated AIN | Prednisolone 0.5–1 mg/kg/day; consider steroid-sparing agent (azathioprine, mycophenolate) | Nephrology + rheumatology co-management |
| IgG4-related TIN | Prednisolone 0.6 mg/kg/day × 4 weeks, taper over 3–6 months | Relapse common; rituximab for refractory cases |
| TINU syndrome | Corticosteroids ± NSAIDs for uveitis | Ophthalmology + nephrology co-management |
Second-Line / Steroid-Sparing Agents
For steroid-dependent, steroid-refractory, or chronic interstitial nephritis, consider in consultation with nephrology:
Monitoring & Follow-Up
Special Populations
ATSI Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of kidney disease, with rates of end-stage kidney disease (ESKD) approximately 8–10 times higher than non-Indigenous Australians (AIHW 2023). While AIN has not been studied separately in ATSI populations, several factors increase both the risk and diagnostic challenge:
📚 References
- 1. Perazella MA, Markowitz GS. Drug-induced acute interstitial nephritis. Nat Rev Nephrol. 2010;6(8):461-470. doi:10.1038/nrneph.2010.71
- 2. Muriithi AK, Leung N, Valeri AM, et al. Biopsy-proven acute interstitial nephritis, 1993–2011: a case series. Am J Kidney Dis. 2014;64(4):558-566. doi:10.1053/j.ajkd.2014.04.027
- 3. Clarkson MR, Giblin L, O'Connell FP, et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004;19(11):2778-2783. doi:10.1093/ndt/gfh485
- 4. Praga M, González E. Acute interstitial nephritis. Kidney Int. 2010;77(11):956-961. doi:10.1038/ki.2010.89
- 5. Raghavan R, Eknoyan G. Acute interstitial nephritis — a reappraisal and update. Clin Nephrol. 2014;82(3):149-162. doi:10.5414/CN108362
- 6. Moledina DG, Perazella MA. PPI-associated acute interstitial nephritis. Clin J Am Soc Nephrol. 2021;16(4):604-612. doi:10.2215/CJN.15751020
- 7. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 223. Canberra: AIHW; 2023.
- 8. Saeki T, Kawano M, Mizushima I, et al. The clinical course of patients with IgG4-related kidney disease. Kidney Int. 2013;84(4):826-833. doi:10.1038/ki.2013.191
- 9. Cortazar FB, Kibbelaar ZA, Glezerman IG, et al. Clinical features and outcomes of immune checkpoint inhibitor–associated AKI: a multicenter study. J Am Soc Nephrol. 2020;31(2):435-446. doi:10.1681/ASN.2019070676
- 10. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(1):1-138. doi:10.1038/kisup.2012.1
- 11. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease (3rd edition). Darwin: Menzies School of Health Research; 2020.
- 12. Kitching AR, Hutton HL. The macrophage in AIN — friend or foe? Kidney Int. 2021;100(3):511-514. doi:10.1016/j.kint.2021.05.027