📋 Key Information Summary
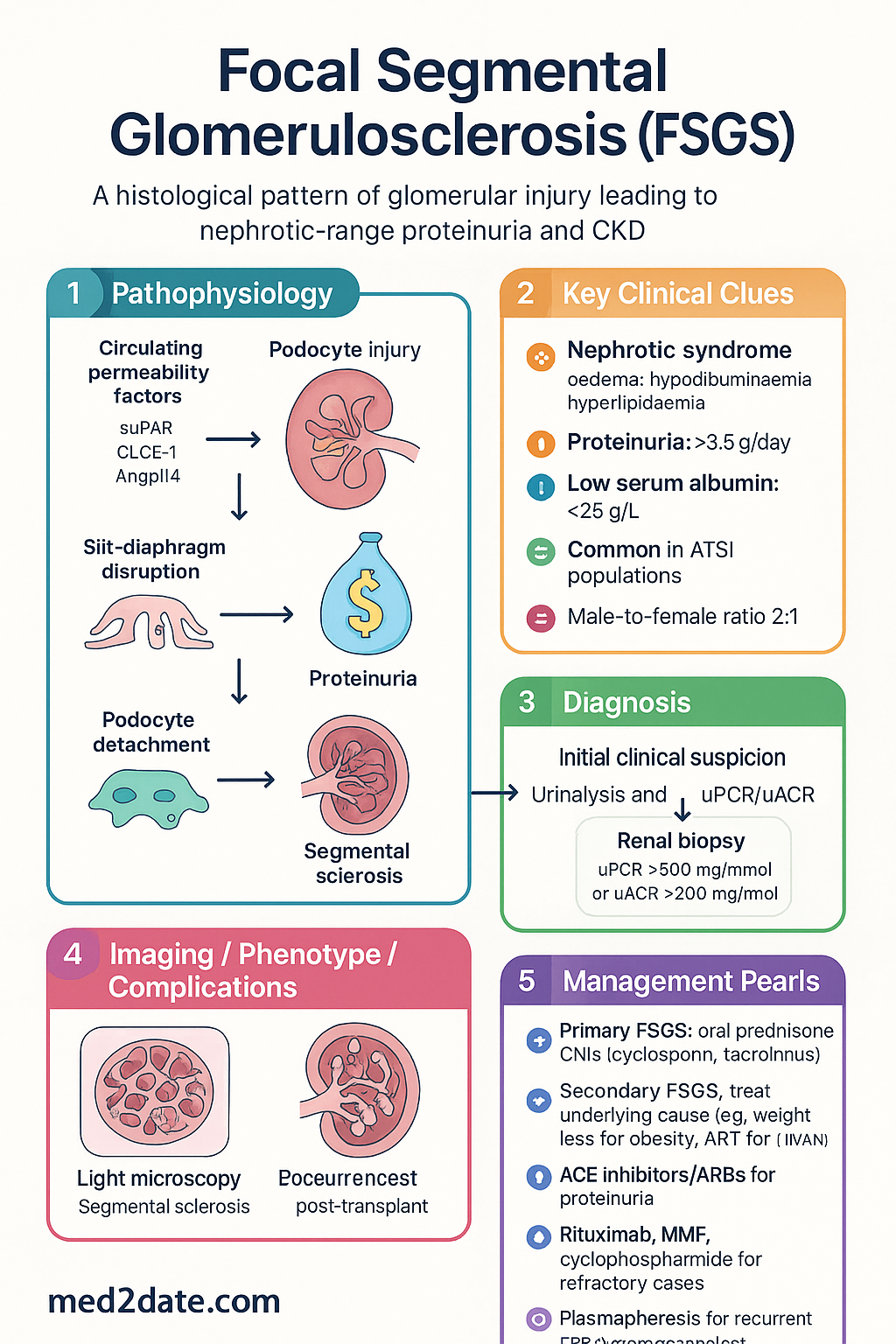
- Focal segmental glomerulosclerosis (FSGS) is a histological pattern of glomerular injury characterised by focal (some glomeruli) and segmental (part of a glomerulus) scarring, leading to nephrotic-range proteinuria and progressive chronic kidney disease (CKD).
- Primary (idiopathic) FSGS is mediated by circulating permeability factors causing podocyte injury and slit-diaphragm disruption; secondary FSGS arises from adaptive, genetic, or toxin-mediated glomerular overload.
- Key secondary causes include obesity-related glomerulomegaly, HIV-associated nephropathy (HIVAN), heroin nephropathy, reflux nephropathy, reduced nephron mass, and drug exposures (e.g., lithium, sirolimus, pamidronate, interferon-α).
- Incidence in Australia is approximately 7 per million population per year; FSGS is the leading cause of nephrotic syndrome in Aboriginal and Torres Strait Islander (ATSI) adults and accounts for ~15–20 % of primary glomerulonephritis biopsies nationally.
- Renal biopsy is essential for definitive diagnosis; light microscopy shows segmental sclerosis, immunofluorescence is typically negative or shows non-specific IgM/C3 in sclerotic segments, and electron microscopy confirms foot-process effacement in primary FSGS.
- The Columbia classification (not otherwise specified [NOS], perihilar, tip, cellular, collapsing variants) guides prognosis and, to a lesser extent, treatment response.
- Primary FSGS with nephrotic syndrome is treated with oral prednisone 1 mg/kg/day (max 60 mg) for a minimum of 16 weeks (minimum 4 weeks at full dose after remission) before considering treatment failure.
- Calcineurin inhibitors (cyclosporin or tacrolimus) are first-line steroid-sparing agents or second-line therapy for steroid-dependent, steroid-resistant, or steroid-intolerant disease; cyclosporin 3–5 mg/kg/day or tacrolimus 0.05–0.1 mg/kg/day with trough monitoring.
- Secondary FSGS management targets the underlying cause — weight loss for obesity-related FSGS, antiretroviral therapy (ART) for HIVAN, drug cessation for toxin-mediated disease — rather than immunosuppression.
- ACE inhibitors or ARBs are recommended for all patients with proteinuria to reduce intraglomerular pressure and slow CKD progression; target BP <130/80 mmHg (<125/75 if protein >1 g/day).
- Rituximab, mycophenolate mofetil (MMF), and cyclophosphamide are used as second- or third-line agents in refractory primary FSGS; plasmapheresis may be considered for recurrent FSGS post-transplant.
- Approximately 30–50 % of patients with primary FSGS progress to end-stage kidney disease (ESKD) within 10 years; recurrence post-transplant occurs in 20–40 % of cases, often within days to weeks.
- ATSI Australians have disproportionately higher rates of FSGS, driven by higher prevalence of obesity, diabetes, low birth weight (reduced nephron mass), and socioeconomic barriers to specialist nephrology care.
Introduction & Australian Epidemiology
Focal segmental glomerulosclerosis (FSGS) is a clinico-pathological entity characterised by a pattern of glomerular injury in which some (focal) glomeruli show scarring of a portion (segment) of the capillary tuft. It represents a final common pathway of podocyte injury from diverse aetiologies and is classified histologically rather than as a single disease. FSGS is a leading cause of the nephrotic syndrome in adults and an increasingly important cause of progressive chronic kidney disease (CKD) worldwide.
Australian Epidemiology
Data from the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) and Australian kidney biopsy registries indicate that FSGS accounts for approximately 15–20 % of all primary glomerulonephritis biopsies. The overall population incidence is estimated at 7 per million per year, but this figure is rising, reflecting increasing obesity and metabolic syndrome prevalence. In Aboriginal and Torres Strait Islander populations, FSGS is disproportionately more common and is frequently associated with secondary aetiologies including obesity, type 2 diabetes, and low birth weight. FSGS is the most common primary glomerular disease leading to ESKD in Indigenous Australians under 50 years of age.
The male-to-female ratio is approximately 2:1 for primary FSGS. Peak incidence occurs in the third to fourth decades for primary FSGS, while secondary forms are seen across all age groups. The incidence of FSGS in children in Australia is approximately 2 per 100,000 per year, accounting for 10–15 % of childhood nephrotic syndrome.
Primary vs Secondary FSGS
Distinguishing primary (idiopathic) FSGS from secondary FSGS is critical because treatment strategies differ fundamentally. Primary FSGS is presumed immune-mediated and responds to immunosuppression; secondary FSGS requires management of the underlying cause.
| Feature | Primary FSGS | Secondary FSGS |
|---|---|---|
| Aetiology | Circulating permeability factor(s); idiopathic | Adaptive, genetic, viral, or toxin-mediated |
| Presentation | Nephrotic syndrome (oedema, hypoalbuminaemia, hyperlipidaemia) | Subnephrotic or nephrotic proteinuria; oedema less prominent |
| Proteinuria | Usually >3.5 g/day (nephrotic range) | Variable; often 1–3 g/day |
| Serum albumin | Low (<25 g/L) | Often near-normal or mildly reduced |
| Electron microscopy | Diffuse foot-process effacement (>80 %) | Focal or mild foot-process effacement |
| Treatment | Immunosuppression (steroids, CNIs) | Treat underlying cause; avoid unnecessary immunosuppression |
| Prognosis | 30–50 % progress to ESKD within 10 years | Depends on aetiology and response to cause-specific therapy |
Secondary FSGS — Key Causes in Australia
Obesity-Related Glomerulopathy (ORG)
With over 65 % of Australian adults classified as overweight or obese (AIHW 2023), ORG is the most common secondary cause of FSGS in Australia. Glomerulomegaly with or without FSGS lesions results from increased glomerular capillary pressure driven by hyperfiltration in a setting of excess body mass. Characteristic findings include glomerulomegaly (glomerular volume >3.5 × normal), relatively preserved foot processes, and a perihilar pattern of sclerosis. Treatment centres on weight loss (target BMI <30 kg/m²), ACE inhibitor or ARB therapy, and management of metabolic comorbidities. Bariatric surgery may be considered for BMI >40 kg/m² (or >35 with significant comorbidity) with refractory proteinuria.
HIV-Associated Nephropathy (HIVAN)
HIVAN, caused by direct viral infection of renal tubular epithelial cells and podocytes, presents with collapsing FSGS — the most aggressive histological variant. Australia has approximately 29,000 people living with HIV (Kirby Institute 2023); HIVAN is more common in those of African descent and in people with advanced immunosuppression (CD4 <200 cells/µL). The single most effective intervention is combination antiretroviral therapy (cART), which dramatically reduces progression to ESKD. Immunosuppression with corticosteroids is not recommended for HIVAN. ACE inhibitors or ARBs provide additional renoprotection.
Drug-Induced FSGS
Several drugs are recognised causes of FSGS or FSGS-like injury in the Australian context:
- Lithium: Long-term lithium use (common in Australian psychiatric practice) can cause chronic tubulointerstitial nephropathy with secondary FSGS. Monitor serum creatinine and eGFR every 6–12 months; consider switching mood stabiliser if eGFR declines significantly.
- Pamidronate / zoledronic acid: Bisphosphonate-associated collapsing FSGS is rare but well described. Discontinue the offending agent; kidney function may partially recover.
- Sirolimus / everolimus (mTOR inhibitors): Used in transplant immunosuppression; may cause de novo or worsening FSGS, particularly in those with pre-existing proteinuria.
- Interferon-α: Historically used in hepatitis C treatment; causes podocyte dedifferentiation and collapsing FSGS. With the advent of direct-acting antivirals, this exposure has decreased.
- Anabolic steroids and heroin: Heroin-associated nephropathy (now uncommon in Australia) classically produces FSGS; anabolic steroid use in bodybuilding communities is an under-recognised cause.
Adaptive / Maladaptive FSGS
Reduced nephron number (low birth weight, unilateral renal agenesis, reflux nephropathy, cortical necrosis, surgical nephrectomy) or increased metabolic demand (sickle cell disease, cyanotic congenital heart disease) leads to compensatory glomerular hyperfiltration, capillary hypertension, and eventual segmental sclerosis. Management involves treating the primary condition, ACE inhibitor/ARB therapy, and avoiding nephrotoxins.
Pathophysiology — Podocyte Injury
Podocytes are terminally differentiated visceral epithelial cells that interdigitate with foot processes bridged by the slit diaphragm, forming the final size-selective barrier of the glomerular filtration apparatus. FSGS pathogenesis converges on podocyte injury, detachment, and depletion below a critical threshold, triggering segmental adhesion (synechia) to Bowman's capsule, capillary collapse, and sclerosis.
Primary FSGS — Circulating Permeability Factor Hypothesis
Evidence from rapid recurrence of FSGS post-transplant (within hours to days), the efficacy of plasmapheresis, and in vitro assays demonstrating increased albumin permeability of isolated glomeruli exposed to patient sera supports the existence of one or more circulating factors. Candidates include soluble urokinase plasminogen activator receptor (suPAR), cardiotrophin-like cytokine factor 1 (CLCF-1), and angiopoietin-like 4 (Angptl4). suPAR has received the most attention, although its specificity remains debated. These factors target the podocyte slit-diaphragm complex, disrupting αvβ3 integrin signalling and nephrin expression, leading to foot-process effacement, cytoskeletal rearrangement, and podocyte detachment.
Genetic FSGS
Monogenic causes account for approximately 5–10 % of adult and 20–30 % of paediatric FSGS. Key genes encode slit-diaphragm proteins (NPHS1/nephrin, NPHS2/podocin), cytoskeletal regulators (ACTN4/α-actinin-4, INF2/inverted formin-2), mitochondrial proteins (COQ2, COQ6), and nuclear lamina components (LMNA/lamin A/C). Genetic testing is indicated in familial FSGS, steroid-resistant nephrotic syndrome in children, or when histology suggests a genetic aetiology (e.g., diffuse mesangial sclerosis). In Australia, genomic testing can be accessed through the Medicare-funded Genomic Medicine programme (MBS item 73343) at participating genetic health services.
Secondary FSGS — Haemodynamic Mechanisms
In secondary FSGS, the primary insult is glomerular hypertension and hyperfiltration rather than a circulating permeability factor. Obesity, reduced nephron mass, and conditions increasing metabolic demand lead to afferent arteriolar vasodilation, increased glomerular capillary pressure, and mechanical stress on podocytes. This manifests histologically as glomerulomegaly with perihilar sclerosis and relatively preserved foot processes — contrasting with the diffuse foot-process effacement of primary FSGS.
The Sclerosis Cascade
Investigations & Biopsy Findings
Baseline Investigations
Renal Biopsy
Light Microscopy
Segmental solidification of the glomerular tuft with increased extracellular matrix, obliteration of capillary lumina, and frequently hyalinosis (insudation of plasma proteins). In early disease, only a minority of glomeruli are affected (hence "focal"), and only a portion of each glomerulus is involved (hence "segmental"). As the disease progresses, global sclerosis supervenes. Tubulointerstitial fibrosis and tubular atrophy correlate more strongly with prognosis than the percentage of globally sclerosed glomeruli.
Immunofluorescence (IF)
Typically negative or shows non-specific trapping of IgM and C3 within sclerotic segments. Granular capillary-loop staining for IgG should prompt consideration of membranous nephropathy or IgA nephropathy superimposed on FSGS. Staining for IgA in mesangial areas is characteristic of IgA nephropathy, not primary FSGS.
Electron Microscopy (EM)
The key finding distinguishing primary from secondary FSGS is the extent of foot-process effacement: >80 % diffuse effacement favours primary FSGS; focal or mild effacement (<50 %) with glomerulomegaly favours secondary FSGS. EM also identifies immune-complex deposits, fibrillary structures, or organised deposits that may suggest an alternative or superimposed diagnosis.
Columbia Histological Classification of FSGS
| Variant | Key Features | Prognosis |
|---|---|---|
| Not Otherwise Specified (NOS) | Segmental increase in matrix without qualifying for other variants | Intermediate; most common variant |
| Perihilar | Segmental sclerosis at the vascular pole; hyalinosis common | Better prognosis; associated with secondary FSGS |
| Tip | Sclerotic lesion at the urinary pole (tip of proximal tubule) | Best prognosis; highest steroid response rate (60–70 %) |
| Cellular | Endocapillary hypercellularity with foam cells; no sclerosis required | Variable; may progress rapidly |
| Collapsing | Collapse of glomerular tuft with hypertrophic podocytes | Worst prognosis; associated with HIVAN, viral infections |
Clinical Presentation & Diagnostic Criteria
Primary FSGS
Primary FSGS most commonly presents with the full nephrotic syndrome: generalised peripheral oedema (often periorbital and lower limb), frothy urine, weight gain from fluid retention, and features of hypoalbuminaemia (ascites, pleural effusions). Hypertension is present in approximately 30–50 % of patients at diagnosis. Haematuria (microscopic) may be present in up to 40 %. Kidney function at presentation ranges from normal to severely impaired; elevated serum creatinine at presentation is a poor prognostic sign. Thromboembolic complications (renal vein thrombosis, pulmonary embolism) occur in 10–30 % of patients with nephrotic syndrome.
Secondary FSGS
Secondary FSGS often presents insidiously with asymptomatic proteinuria detected on routine health screening or during investigation of declining eGFR. Overt nephrotic syndrome is less common. Clinical clues to a secondary aetiology include obesity (BMI >30 kg/m²), known HIV infection, history of reflux nephropathy or solitary kidney, and medication history (lithium, bisphosphonates, mTOR inhibitors).
Diagnostic Approach
Risk Stratification
Prognosis in FSGS is determined by histological variant, degree of proteinuria, kidney function at presentation, tubulointerstitial fibrosis on biopsy, and treatment response.
Management — Immunosuppressive Therapy
Immunosuppressive therapy is indicated for primary FSGS with nephrotic syndrome. Secondary FSGS should be managed by treating the underlying cause; immunosuppression is generally not beneficial and may be harmful.
First-Line: Corticosteroids
Second-Line: Calcineurin Inhibitors (CNIs)
CNIs are first-line steroid-sparing agents for steroid-dependent, steroid-resistant, or steroid-intolerant primary FSGS. They are also used as initial therapy when corticosteroids are contraindicated.
Third-Line and Refractory Disease
Supportive Therapy (All Patients)
SGLT2 Inhibitors
Emerging evidence from DAPA-CKD and EMPA-KIDNEY trials supports the use of SGLT2 inhibitors (dapagliflozin 10 mg PO daily or empagliflozin 10 mg PO daily) in non-diabetic CKD with proteinuria. SGLT2 inhibitors reduce intraglomerular pressure through tubuloglomerular feedback and have shown benefit in slowing eGFR decline and reducing proteinuria in a broad range of proteinuric kidney diseases, including FSGS. They are now recommended by Kidney Health Australia for CKD with uACR >22 mg/mmol regardless of diabetic status.
Monitoring
Definitions of Treatment Response
| Response Category | Definition |
|---|---|
| Complete remission (CR) | uPCR <50 mg/mmol (proteinuria <0.3 g/day) with stable or improving eGFR |
| Partial remission (PR) | uPCR 50–300 mg/mmol (proteinuria 0.3–3.5 g/day) with ≥50 % reduction from baseline and stable or improving eGFR |
| Relapse | Return to nephrotic-range proteinuria after prior complete remission |
| Steroid-dependent | Relapse during steroid taper or within 2 weeks of cessation |
| Steroid-resistant | Failure to achieve CR or PR after ≥16 weeks of high-dose prednisone |
| Frequently relapsing | ≥2 relapses within 6 months or ≥3 relapses within 12 months |
Recommended Monitoring Schedule
| Parameter | Frequency (Active Treatment) | Frequency (Remission Maintenance) |
|---|---|---|
| uPCR or uACR | Every 2–4 weeks | Every 1–3 months for 2 years, then every 6 months |
| Serum creatinine / eGFR | Every 2–4 weeks | Every 1–3 months |
| Serum albumin | Every 2–4 weeks | Every 3 months |
| Lipid profile | At diagnosis, then every 3–6 months | Every 6–12 months |
| Fasting glucose / HbA1c | Monthly during steroid therapy | As per standard diabetic care |
| CNI trough levels | Every 1–2 weeks initially, then monthly | Every 1–3 months |
| Blood pressure | Every visit | Every visit; home BP monitoring encouraged |
Special Populations
FSGS Recurrence Post-Transplant
Recurrent FSGS is a significant complication following renal transplantation and is the most common cause of early graft failure in FSGS patients. Recurrence rates are 20–40 % for primary FSGS and can be as high as 80–100 % after a prior graft lost to recurrence.
Risk Factors for Recurrence
- Prior recurrence in a previous transplant graft
- Rapid progression to ESKD (<3 years from diagnosis)
- Younger age at onset
- White race
- Collapsing FSGS variant
- Absence of FSGS in native kidneys (donor-derived FSGS is rare)
Management of Recurrent FSGS
🇦🇹 Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. D'Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. New England Journal of Medicine. 2011;365(25):2398–2411.
- 2. Rosenberg AZ, Kopp JB. Focal segmental glomerulosclerosis. Clinical Journal of the American Society of Nephrology. 2017;12(3):502–517.
- 3. De Vriese AS, Sethi S, Nath KA, Glassock RJ, Fervenza FC. Differentiating primary, genetic, and secondary FSGS in adults: a clinicopathologic approach. Journal of the American Society of Nephrology. 2018;29(3):759–774.
- 4. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International. 2021;100(4S):S1–S276.
- 5. Briganti EM, Dowling J, Finlay M, et al. The incidence of biopsy-proven glomerulonephritis in Australia. Nephrology Dialysis Transplantation. 20