📋 Key Information Summary
- Myeloma kidney (cast nephropathy) is the most common renal pathology in multiple myeloma, caused by intratubular light-chain casts and occurring in 20–50 % of patients at diagnosis.
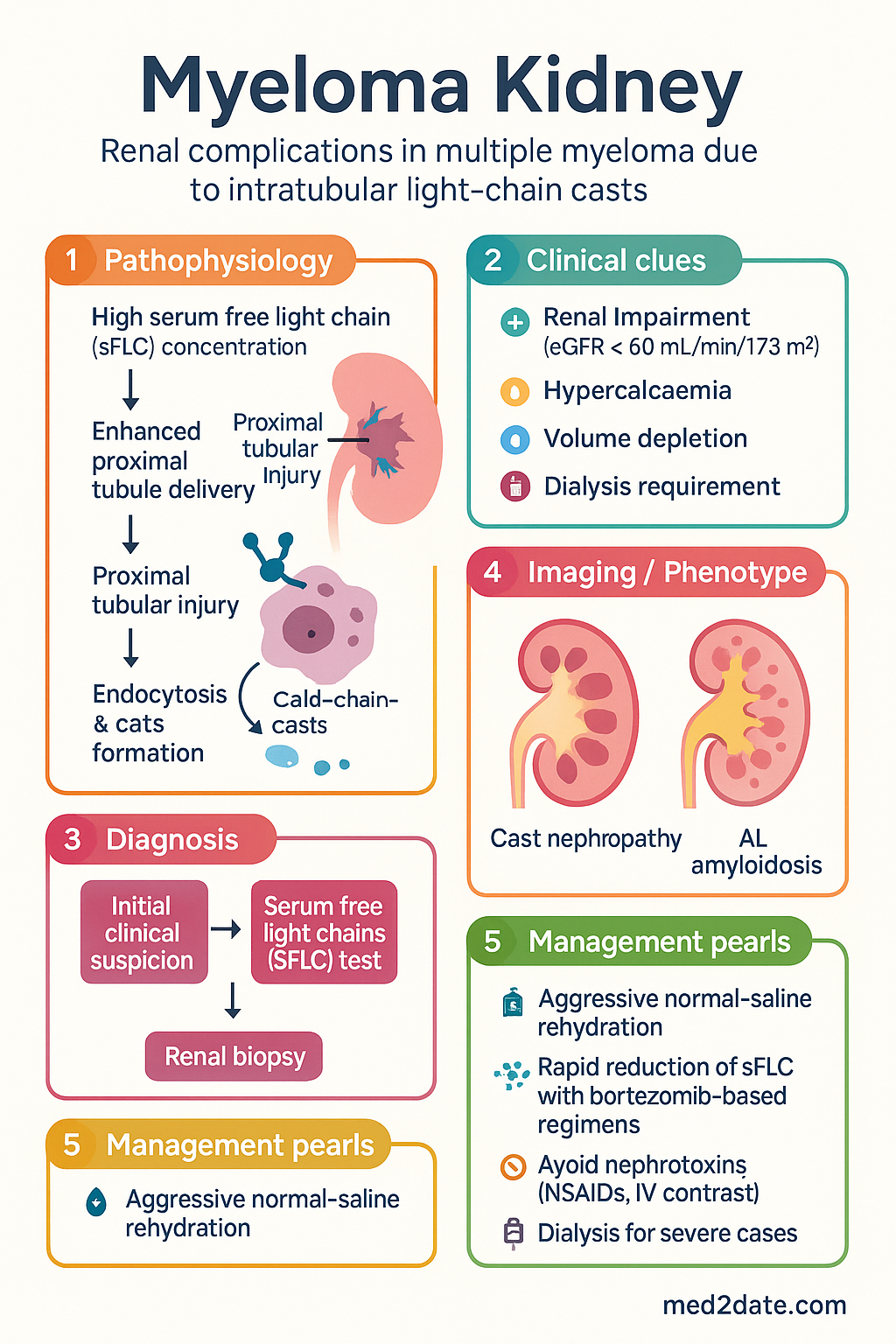
- Renal impairment (eGFR < 60 mL/min/1.73 m²) is present in up to 50 % of newly diagnosed myeloma patients; 20–25 % require dialysis at some point.
- Cast nephropathy requires two simultaneous factors: high serum free light chain (sFLC) concentration AND enhanced proximal tubule delivery (volume depletion, nephrotoxins).
- Hypercalcaemia worsens renal function through volume depletion and vasoconstriction; aggressive normal-saline rehydration is first-line therapy.
- AL amyloidosis is a distinct renal mechanism (amyloid fibrils from monoclonal light chains); differentiated from cast nephropathy by Congo-red staining on renal biopsy.
- Rapid reduction of pathogenic sFLC is the cornerstone of treatment — bortezomib-based regimens (e.g., CyBorD, VTD) achieve fastest sFLC responses.
- High cut-off (HCO) haemodialysis or extended haemodiafiltration to remove sFLC remains investigational in Australia; not standard-of-care.
- Avoid nephrotoxins — NSAIDs, IV contrast, aminoglycosides — in all myeloma patients with renal impairment.
- Renal biopsy is indicated when the aetiology of renal impairment is uncertain or AL amyloidosis is suspected.
- Dialysis-dependent patients can achieve dialysis independence with early, aggressive anti-myeloma therapy.
- Daratumumab-based quadruple regimens are emerging as first-line in transplant-eligible and ineligible patients; PBS Authority Required.
- Aboriginal and Torres Strait Islander peoples have higher rates of myeloma diagnosed at advanced stages with renal impairment, requiring culturally safe, locally accessible nephrology and haematology services.
Introduction & Australian Epidemiology
Multiple myeloma (MM) is a malignant proliferation of monoclonal plasma cells producing abnormal immunoglobulin or free light chains (FLCs). Renal involvement — collectively termed myeloma kidney — is one of the most frequent and impactful complications, present in 20–50 % of patients at diagnosis and contributing significantly to morbidity, mortality, and health-system cost.
In Australia, the estimated age-standardised incidence of MM is approximately 6–7 per 100 000 person-years, with around 1 800 new diagnoses annually. Renal impairment (eGFR < 60 mL/min/1.73 m²) is documented in up to half of newly diagnosed patients, and 20–25 % develop dialysis-dependent kidney failure during their disease course. Myeloma is more common in males, Aboriginal and Torres Strait Islander peoples, and individuals aged > 65 years.
The mechanisms of myeloma kidney are multifactorial and include:
- Cast nephropathy (myeloma kidney) — the most common and specific mechanism, involving precipitation of monoclonal light chains with Tamm–Horsfall protein in distal tubules.
- Hypercalcaemia — causes renal vasoconstriction, volume depletion, and nephrocalcinosis.
- AL amyloidosis — deposition of amyloid fibrils derived from monoclonal light chains in glomeruli and vessels.
- Direct tubular toxicity — free light chains are endocytosed by proximal tubular epithelial cells, triggering cytokine release, NF-κB activation, and apoptosis.
- Monoclonal immunoglobulin deposition disease (MIDD) — non-amyloid deposits of light or heavy chains in glomerular and tubular basement membranes.
- Cryoglobulinaemia and crystal-storing histiocytosis — rare mechanisms.
Early recognition and rapid intervention — particularly prompt reduction of pathogenic free light chains — remain the strongest modifiable determinants of renal recovery.
Cast Nephropathy (Myeloma Kidney)
Cast nephropathy is the hallmark renal lesion of multiple myeloma, accounting for the majority of myeloma-associated acute kidney injury (AKI). It results from the intratubular precipitation of monoclonal free light chains with Tamm–Horsfall protein (uromodulin) in the thick ascending limb of the loop of Henle.
Pathophysiology
Two concurrent conditions are required for cast formation:
- High serum free light chain concentration — typically > 500 mg/L, often > 1 000 mg/L. The monoclonal FLC must be of a restricted charge–hydrophobicity profile that favours binding to uromodulin.
- Enhanced distal delivery of FLC — promoted by volume depletion, hypercalcaemia, loop diuretics, NSAIDs, IV contrast, or any cause of reduced proximal tubular reabsorption.
The resulting casts obstruct tubular lumens, trigger interstitial inflammation, and produce a pattern of “flame-shaped” multinucleated giant cell reaction on histology. Progressive tubular atrophy and interstitial fibrosis lead to irreversible kidney damage if the FLC burden is not rapidly reduced.
Histological Features
Renal biopsy — when clinically indicated — demonstrates:
- Dense, fractured, eosinophilic casts within distal tubules.
- Giant cell reaction surrounding casts (foreign-body type).
- Tubular rupture and interstitial inflammation.
- Immunofluorescence staining for a single light chain type (κ or λ) within casts.
- Absent glomerular deposits (distinguishes from amyloidosis / MIDD).
Renal Biomarkers
| Biomarker | Role in Cast Nephropathy | Australian Availability |
|---|---|---|
| Serum free light chains (sFLC) | Diagnostic and prognostic; FLC ratio identifies monoclonality; absolute level predicts cast risk | Freelite® assay; MBS item 69494 |
| Serum & urine protein electrophoresis | Confirms monoclonal protein (M-spike) | MBS items 69488, 69491 |
| eGFR / serum creatinine | Tracks AKI severity and response to therapy | Standard pathology |
| Urine protein-to-creatinine ratio | Quantifies proteinuria; disproportionately high in myeloma kidney | Standard pathology |
| NGAL / KIM-1 (urine) | Research biomarkers of tubular injury; not routine in Australia | Research use only |
Hypercalcaemia & Direct Tubular Toxicity
Hypercalcaemia
Hypercalcaemia occurs in approximately 15–30 % of MM patients at diagnosis and is a major reversible contributor to renal impairment. Elevated calcium promotes:
- Renal vasoconstriction and reduced glomerular filtration rate.
- Volume depletion through nephrogenic diabetes insipidus (calcium blocks aquaporin-2 channels).
- Nephrocalcinosis and medullary calcium deposition.
- Enhanced Tamm–Horsfall protein–light chain binding, synergistically promoting cast nephropathy.
Hypercalcaemia Management
Direct Tubular Toxicity
Free light chains are freely filtered at the glomerulus and reabsorbed by proximal tubular epithelial cells via megalin/cubilin receptor-mediated endocytosis. Intracellular accumulation triggers:
- Activation of NF-κB signalling → pro-inflammatory cytokine release (IL-6, IL-8, TNF-α).
- Lysosomal overload and cathepsin-B release → tubular cell apoptosis and necrosis.
- Complement activation via the alternative pathway on tubular cell surfaces.
- Reactive oxygen species generation and mitochondrial dysfunction.
This mechanism contributes to AKI independently of cast formation and is particularly relevant in patients with modest sFLC elevation but significant tubular injury biomarkers (e.g., elevated urine NGAL).
AL Amyloidosis vs Other Mechanisms
AL Amyloidosis
Systemic AL (immunoglobulin light chain) amyloidosis occurs when misfolded monoclonal light chains — most commonly λ (lambda) — form β-pleated-sheet amyloid fibrils that deposit in organs including the kidney, heart, liver, and peripheral nerves. It is distinct from cast nephropathy and is present in approximately 5–10 % of myeloma patients.
| Feature | Cast Nephropathy | AL Amyloidosis | MIDD |
|---|---|---|---|
| Primary lesion | Intratubular light chain casts | Glomerular & vascular amyloid deposits | Glomerular & tubular basement membrane deposits |
| Typical presentation | Acute kidney injury | Nephrotic syndrome, gradual eGFR decline | Proteinuria, renal impairment, often monoclonal gammopathy |
| Light chain isotype | κ or λ (often κ) | Mostly λ (λ:κ ~ 3:1) | Mostly κ |
| Congo-red staining | Negative | Apple-green birefringence | Negative |
| Biopsy features | Fractured casts, giant cells | Congo-red positive amorphous deposits in mesangium, vessels | PAS-positive linear deposits on GBM / TBM by EM |
| Ultrastructure (EM) | Dense amorphous casts | Randomly oriented fibrils (8–12 nm) | Powdery electron-dense deposits |
| Nephrotic-range proteinuria | Uncommon | Common | Common |
| Cardiac involvement | Rare | Frequent (major prognostic determinant) | Rare |
Other Renal Mechanisms in Myeloma
- Monoclonal immunoglobulin deposition disease (MIDD): Non-amyloid, Congo-red-negative deposits of light chains (LCDD), heavy chains (HCDD), or both (LHCDD) on glomerular and tubular basement membranes. Produces nodular sclerosing glomerulopathy resembling diabetic nephropathy.
- Cryoglobulinaemic glomerulonephritis: Type I cryoglobulins (monoclonal IgG or IgM) can cause membranoproliferative GN. Managed with anti-myeloma therapy and plasma exchange.
- Crystal-storing histiocytosis: Rare; intracellular crystal accumulation of monoclonal light chains in histiocytes, occasionally involving the kidney.
- Proximal tubular dysfunction (Fanconi syndrome): Light chain-mediated damage to proximal tubule causing glycosuria, aminoaciduria, phosphaturia, and type 2 (proximal) RTA.
- Direct plasma cell infiltration: Rare; renal parenchymal infiltration by myeloma cells causing mass lesions and AKI.
Management — Hydration, Myeloma Treatment, Dialysis
1. Supportive Measures & Hydration
Immediate supportive care is critical to limit ongoing renal injury and optimise the chance of renal recovery:
2. Anti-Myeloma Therapy — Rapid FLC Reduction
The primary goal is rapid and sustained reduction of pathogenic serum free light chains. Bortezomib-based regimens produce the fastest FLC responses (median time to best FLC response: 21 days).
First-Line Regimens (Transplant-Ineligible or Transplant-Eligible Induction)
3. Plasmapheresis & High Cut-Off Dialysis
The role of plasma exchange (PLEX) to remove circulating FLCs remains uncertain. The largest RCT (Clark et al., 2005) showed no significant benefit of PLEX over standard care, but was underpowered. Meta-analyses suggest a possible trend toward reduced dialysis dependence. Australian practice: PLEX may be considered in severe AKI (eGFR < 15 or dialysis-dependent) with very high sFLC levels (> 10 000 mg/L), in conjunction with anti-myeloma therapy.
High cut-off (HCO) haemodialysis using membranes with a 45–60 kDa molecular weight cut-off can remove FLCs more efficiently than standard HD. The European EuLITE trial demonstrated improved dialysis independence rates with HCO dialysis + bortezomib vs conventional HD + bortezomib. However, HCO dialysis is not currently standard-of-care in Australia and is available only at select tertiary centres as part of clinical research protocols.
4. Renal Replacement Therapy (Dialysis)
Indications for dialysis in myeloma kidney are the same as for other causes of AKI:
- Refractory hyperkalaemia (> 6.5 mmol/L despite medical therapy).
- Severe metabolic acidosis (pH < 7.1) unresponsive to bicarbonate.
- Pulmonary oedema / fluid overload unresponsive to diuretics.
- Uraemic symptoms (encephalopathy, pericarditis, intractable nausea).
- Refractory hypercalcaemia (> 3.5 mmol/L).
Modality: Intermittent haemodialysis (IHD) is standard. Extended haemodiafiltration (HDF) may offer improved FLC clearance. Continuous renal replacement therapy (CRRT) is used in haemodynamically unstable patients in ICU.
Prognosis on dialysis: With effective anti-myeloma therapy, approximately 20–40 % of dialysis-dependent patients achieve dialysis independence, usually within 2–6 months. Factors predicting renal recovery include early initiation of bortezomib therapy, sFLC reduction ≥ 50 % within 21 days, and shorter duration of dialysis dependence (< 30 days).
5. Monitoring Response
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a higher incidence of myeloma compared with non-Indigenous Australians, with evidence of later-stage presentation, higher rates of renal impairment at diagnosis, and poorer survival outcomes. Myeloma kidney in this population is compounded by the high background prevalence of chronic kidney disease (CKD), diabetes, and limited access to specialist haematology and nephrology services in regional and remote areas.
📚 References
- 1. Bridoux F, Fermand JP. Optimising treatment strategies for myeloma cast nephropathy: rationale for a randomised prospective trial. Advances in Chronic Kidney Disease. 2012;19(5):333–341.
- 2. Dimopoulos MA, Sonneveld P, Leung N, et al. International Myeloma Working Group recommendations for the diagnosis and management of myeloma-related renal impairment. Journal of Clinical Oncology. 2016;34(13):1544–1557.
- 3. Clark WF, Stewart AK, Rock GA, et al. Plasma exchange when myeloma presents as acute renal failure: a randomized, controlled trial. Annals of Internal Medicine. 2005;143(11):777–784.
- 4. Hutchison CA, Bradwell AR, Cook M, et al. Treatment of acute renal failure secondary to multiple myeloma with chemotherapy and extended high cut-off hemodialysis. Clinical Journal of the American Society of Nephrology. 2009;4(4):745–754.
- 5. Haynes R, Leung N, Kyle S, Winearls CG. Myeloma kidney: improving clinical outcomes. Advances in Chronic Kidney Disease. 2012;19(5):324–332.
- 6. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia: Myeloma. Canberra: AIHW; 2023. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 7. RACGP. Red Book — Investigation of suspected monoclonal gammopathy. In: Guidelines for Preventive Activities in General Practice. 9th ed. Melbourne: RACGP; 2016.
- 8. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. The Lancet Oncology. 2014;15(12):e538–e548.
- 9. Rajkumar SV, Jacobus S, Callander NS, et al. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial. The Lancet Oncology. 2010;11(1):29–37.
- 10. Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. New England Journal of Medicine. 2019;380(22):2104–2115.
- 11. Morie A, Gertz MA, Dispenzieri A. End-stage renal disease in AL amyloidosis: clinical characteristics and outcomes. Blood Cancer Journal. 2021;11:152.
- 12. RHDAustralia. National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People. 3rd ed. Darwin: RACGP; 2018.
- 13. Singhal S, Mehta J, Desikan R, et al. Antitumor activity of thalidomide in refractory multiple myeloma. New England Journal of Medicine. 1999;341(21):1565–1571.
- 14. Corso A, Barbarano L, Mangiacavalli S, et al. Bortezomib plus dexamethasone can improve stem cell collection and overcome the need for additional chemotherapy before autologous transplant in patients with myeloma. Leukemia & Lymphoma. 2010;51(2):236–242.