📋 Key Information Summary
- Chronic kidney disease (CKD) is defined as abnormalities of kidney structure or function present for >3 months, with implications for health — staged by GFR (G1–G5) and albuminuria (A1–A3) using the KDIGO 2012 classification.
- CKD prevalence in Australia is approximately 11% of the adult population; rates are significantly higher among Aboriginal and Torres Strait Islander peoples.
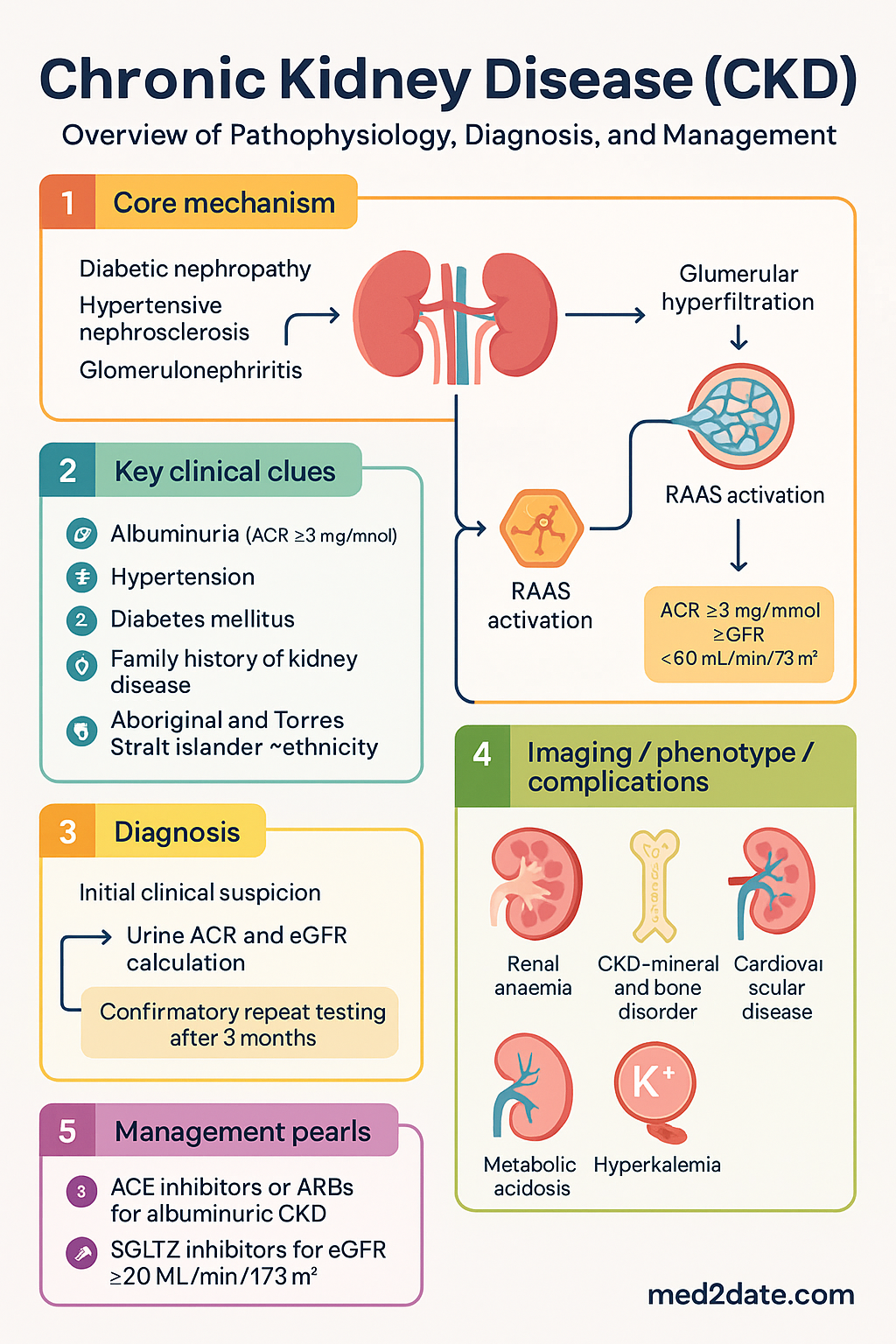
- The leading causes of CKD in Australia are diabetic nephropathy, hypertensive nephrosclerosis, and glomerulonephritis — identification of the underlying aetiology is critical for targeted management.
- Albuminuria (ACR ≥3 mg/mmol) is an independent risk factor for CKD progression, cardiovascular events, and all-cause mortality — it must be quantified at diagnosis and monitored regularly.
- Key complications include renal anaemia (EPO deficiency), CKD-mineral and bone disorder (CKD-MBD), cardiovascular disease, metabolic acidosis, and hyperkalaemia.
- ACE inhibitors or ARBs are first-line renoprotective agents in albuminuric CKD (A2–A3) regardless of diabetes status — monitor potassium and creatinine within 1–2 weeks of initiation.
- SGLT2 inhibitors (dapagliflozin, empagliflozin) are now PBS-listed for CKD with eGFR ≥20 mL/min/1.73 m² and provide significant renoprotective and cardioprotective benefits independent of glycaemic control.
- Finerenone (non-steroidal MRA) is PBS-listed for diabetic kidney disease and reduces CKD progression and cardiovascular risk on top of standard therapy.
- Blood pressure target <130/80 mmHg is recommended for most CKD patients with albuminuria; treat with lifestyle modification and pharmacotherapy.
- Renal anaemia management uses iron repletion (ferritin >100 µg/L, TSAT >20%) before considering erythropoiesis-stimulating agents (ESAs) — haemoglobin target 100–115 g/L.
- CKD-MBD management centres on phosphate restriction, phosphate binders, vitamin D analogues, and cinacalcet for secondary hyperparathyroidism in dialysis patients.
- Timely nephrology referral is indicated for eGFR <30 mL/min/1.73 m², rapid decline (>5 mL/min/year), persistent ACR ≥30 mg/mmol, or difficult-to-manage complications.
- Progression to end-stage kidney disease (ESKD, G5D) requires renal replacement therapy — haemodialysis, peritoneal dialysis, or kidney transplantation — with advance care planning initiated well in advance.
- Cardiovascular disease is the leading cause of death in CKD patients — manage lipids, encourage smoking cessation, optimise glycaemic control, and consider antiplatelet therapy where indicated.
Introduction & Australian Epidemiology
Chronic kidney disease (CKD) is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health. CKD encompasses a broad spectrum of conditions ranging from mild dysfunction detectable only by laboratory abnormalities to end-stage kidney disease (ESKD) requiring renal replacement therapy. The condition is classified using the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 framework, which stratifies patients by estimated glomerular filtration rate (G1–G5) and albuminuria category (A1–A3).
In Australia, CKD represents a significant public health burden. According to the Australian Institute of Health and Welfare (AIHW), approximately 1.7 million Australians (11% of the adult population) have indicators of CKD, though many remain undiagnosed due to the asymptomatic nature of early disease. CKD was recorded as an associated cause of over 17,000 deaths in Australia in 2021, and it is a leading contributor to the burden of cardiovascular disease.
The prevalence of CKD rises sharply with age: approximately 30% of Australians aged ≥75 years have an eGFR <60 mL/min/1.73 m². Diabetic kidney disease is the single most common cause of CKD in Australia, followed by hypertensive nephrosclerosis and glomerulonephritis. Aboriginal and Torres Strait Islander peoples experience CKD at rates 2–4 times higher than non-Indigenous Australians, with earlier onset and faster progression to ESKD.
The economic burden of CKD in Australia is substantial, with direct healthcare costs exceeding billion annually when dialysis and transplantation are included. Early detection through targeted screening (urine albumin-to-creatinine ratio and serum creatinine with eGFR calculation) remains the cornerstone of CKD management, enabling timely intervention to slow progression and reduce complications.
CKD Classification (KDIGO G & A Staging)
The KDIGO 2012 classification system uses two orthogonal axes — glomerular filtration rate (G-stage) and albuminuria (A-stage) — to define CKD severity and prognostic risk. Both axes are independently associated with adverse outcomes including progression to ESKD, cardiovascular events, and all-cause mortality.
GFR Categories (G-Stage)
| G-Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high — with evidence of kidney damage (albuminuria, haematuria, structural abnormality) |
| G2 | 60–89 | Mildly decreased — with evidence of kidney damage |
| G3a | 45–59 | Mildly to moderately decreased |
| G3b | 30–44 | Moderately to severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | <15 | Kidney failure (ESKD if on dialysis = G5D) |
Albuminuria Categories (A-Stage)
| A-Stage | ACR (mg/mmol) | Approximate Equivalent | Description |
|---|---|---|---|
| A1 | <3 | <30 mg/g | Normal to mildly increased |
| A2 | 3–30 | 30–300 mg/g | Moderately increased (formerly "microalbuminuria") |
| A3 | >30 | >300 mg/g | Severely increased (formerly "macroalbuminuria") |
Combined Risk Stratification (G × A Grid)
The KDIGO heat-map combines G-stage and A-stage to assign overall risk:
| Risk Category | Typical G/A Combinations | Monitoring Frequency |
|---|---|---|
| Low risk | G1A1, G2A1 | Annually |
| Moderate risk | G1A2, G2A2, G3aA1 | Every 6 months |
| High risk | G3aA2, G3bA1, G3bA2, G4A1 | Every 3–4 months |
| Very high risk | G3aA3, G3bA3, G4A2–A3, G5A1–A3 | Every 1–3 months |
Pathophysiology & Causes
CKD arises from a wide range of acute and chronic insults to the kidney. Regardless of the initial aetiology, common pathophysiological pathways converge on nephron loss, interstitial fibrosis, and tubular atrophy — a process often termed the "final common pathway" of CKD progression.
Mechanisms of Progressive Nephron Loss
- Glomerular hyperfiltration: Loss of functioning nephrons causes compensatory hyperfiltration in remaining glomeruli, leading to increased intraglomerular pressure, podocyte injury, and progressive glomerulosclerosis.
- Tubulointerstitial fibrosis: Chronic hypoxia, inflammation, and activation of fibroblasts drive collagen deposition in the renal interstitium, correlating more closely with declining function than glomerular changes.
- Renin-angiotensin-aldosterone system (RAAS) activation: Sustained RAAS activation promotes vasoconstriction, sodium retention, fibrosis, and inflammation — central to both hypertensive nephrosclerosis and diabetic nephropathy.
- Chronic inflammation and oxidative stress: Uraemic toxins, advanced glycation end-products, and immune dysregulation perpetuate a pro-inflammatory milieu accelerating nephron loss.
Major Causes of CKD in Australia
| Aetiology | Proportion (approx.) | Key Features |
|---|---|---|
| Diabetic nephropathy | ~35% | Type 2 DM > Type 1; progressive albuminuria, nodular glomerulosclerosis (Kimmelstiel-Wilson) |
| Hypertensive nephrosclerosis | ~25% | Arterionephrosclerosis; risk ↑ with age, ATSI ethnicity; ACR usually A1–A2 |
| Glomerulonephritis | ~15% | IgA nephropathy most common primary GN in Australia; lupus nephritis, ANCA vasculitis |
| Polycystic kidney disease | ~5% | ADPKD — bilateral renal cysts, positive family history; ADPLD less common |
| Reflux nephropathy / chronic pyelonephritis | ~5% | Paediatric reflux leading to scarring; more common in females |
| Other / unknown | ~15% | Obstructive uropathy, NSAID nephropathy, ischaemic nephropathy, myeloma cast nephropathy |
Complications (Anaemia, Bone Disease, CVD)
CKD has systemic consequences far beyond the kidney. As GFR declines, a constellation of metabolic, haematological, cardiovascular, and musculoskeletal complications emerge, collectively driving morbidity and mortality. Identification and proactive management of these complications is central to CKD care.
Renal Anaemia
Anaemia is a common complication of CKD, affecting approximately 50% of patients with eGFR <30 mL/min/1.73 m². The primary mechanism is reduced erythropoietin (EPO) production by peritubular interstitial cells, compounded by iron deficiency (absolute or functional), uraemic inhibition of erythropoiesis, chronic inflammation (hepcidin-mediated iron sequestration), and shortened red cell survival.
Iron targets before ESA initiation: Ferritin >100 µg/L (non-dialysis) or >200 µg/L (dialysis), and transferrin saturation (TSAT) >20%.
CKD-Mineral and Bone Disorder (CKD-MBD)
CKD-MBD encompasses a spectrum of abnormalities in calcium, phosphate, parathyroid hormone (PTH), and vitamin D metabolism that lead to renal osteodystrophy, vascular calcification, and increased fracture risk. It becomes clinically significant from G3a onwards.
- Hyperphosphataemia: Reduced phosphate excretion leads to elevated serum phosphate, driving vascular calcification and secondary hyperparathyroidism. Target serum phosphate 0.9–1.5 mmol/L (G3–G4) and as close to normal as possible (G5/dialysis).
- Hypocalcaemia & vitamin D deficiency: Reduced 1-alpha hydroxylase activity impairs calcitriol synthesis, contributing to hypocalcaemia, secondary hyperparathyroidism, and osteomalacia.
- Secondary hyperparathyroidism: Sustained hyperphosphataemia, hypocalcaemia, and calcitriol deficiency drive parathyroid gland hyperplasia. Target intact PTH: 2–9 × upper limit of normal for dialysis patients.
- Adynamic bone disease: Over-suppression of PTH (excessive cinacalcet or vitamin D) can cause low-turnover bone disease with increased fracture risk.
Cardiovascular Disease in CKD
Cardiovascular disease (CVD) is the leading cause of death in CKD patients, accounting for approximately 40–50% of all deaths in this population. CKD is now recognised as an independent cardiovascular risk equivalent. The relationship between CKD and CVD is bidirectional — CVD accelerates kidney decline through renal hypoperfusion and atheroembolic disease.
- Left ventricular hypertrophy (LVH): Present in >70% of patients starting dialysis; driven by volume overload, hypertension, and anaemia.
- Heart failure: Both heart failure with reduced ejection fraction (HFrEF) and preserved ejection fraction (HFpEF) are common; cardiorenal syndrome complicates management.
- Atherosclerotic CVD: Accelerated atherosclerosis due to dyslipidaemia, chronic inflammation, oxidative stress, and vascular calcification.
- Arrhythmias: Hyperkalaemia and uraemia predispose to atrial fibrillation; sudden cardiac death is a major cause of mortality in dialysis patients.
- Vascular calcification: Medial arterial calcification (Mönckeberg type) is particularly prevalent in CKD-MBD, contributing to arterial stiffness and systolic hypertension.
Lipid management: Atorvastatin 10–80 mg daily or rosuvastatin 10–40 mg daily is recommended for CKD patients aged 50–75 years with eGFR <60 mL/min/1.73 m² (regardless of baseline LDL). No dose adjustment is required for statins in CKD, but combination with fibrates should be avoided. The SHARP trial demonstrated a 17% reduction in major atherosclerotic events with simvastatin/ezetimibe in CKD patients not on dialysis.
Management & Slowing Progression
The primary goals of CKD management are to slow the rate of GFR decline, prevent or manage complications, reduce cardiovascular risk, and prepare for renal replacement therapy if needed. Management is tailored to the underlying aetiology, CKD stage, and individual patient factors.
Blood Pressure Control
Hypertension accelerates CKD progression and is a modifiable cardiovascular risk factor. Target blood pressure is <130/80 mmHg for most CKD patients, particularly those with albuminuria (A2–A3), and <140/90 mmHg for those without albuminuria. Lifestyle modifications (sodium restriction <6 g NaCl/day, weight loss, regular exercise, limited alcohol) are first-line adjuncts to pharmacotherapy.
SGLT2 Inhibitors — A Paradigm Shift in CKD Management
SGLT2 inhibitors have emerged as a cornerstone of CKD management, offering renoprotective and cardioprotective benefits independent of glycaemic control. Landmark trials (DAPA-CKD, EMPA-KIDNEY, CREDENCE) demonstrated significant reductions in CKD progression, heart failure hospitalisation, and cardiovascular mortality.
Non-Steroidal MRA — Finerenone
Glycaemic Control in Diabetic CKD
For patients with diabetic kidney disease, individualised HbA1c targets apply. A target of ≤53 mmol/mol (7.0%) is appropriate for most patients, while less stringent targets (≤64 mmol/mol / 8.0%) may be appropriate for elderly patients or those with limited life expectancy, recurrent hypoglycaemia, or advanced CKD.
- Metformin: Safe to continue down to eGFR 30 mL/min/1.73 m²; reduce dose to 500 mg BD at eGFR 30–45. Cease at eGFR <30 due to lactic acidosis risk.
- SGLT2 inhibitors: First-line add-on therapy (see above) — glycaemic efficacy reduced in advanced CKD but renoprotective benefit persists.
- GLP-1 receptor agonists: Liraglutide (Victoza®) and semaglutide (Ozempic®) have demonstrated cardiovascular and renal benefits. Dose adjustment not required in CKD, but GI side effects may limit use.
- Insulin: Requirements may decrease in advanced CKD due to reduced renal insulin clearance — risk of hypoglycaemia increases. Monitor closely and reduce doses as GFR declines.
Metabolic Acidosis
Metabolic acidosis (serum bicarbonate <22 mmol/L) is common in CKD G4–G5 and accelerates muscle wasting, bone disease, and CKD progression. Treatment with oral sodium bicarbonate (600–1200 mg PO TDS) to maintain serum bicarbonate ≥22 mmol/L is recommended. Monitor for sodium/fluid overload and hypokalaemia during therapy.
Hyperkalaemia Management
Hyperkalaemia (K⁺ >5.5 mmol/L) is a common and potentially life-threatening complication, particularly in patients taking ACEi/ARBs, spironolactone, or finerenone. Management strategies include:
- Dietary potassium restriction (<2 g/day if recurrent hyperkalaemia)
- Sodium zirconium cyclosilicate (Lokelma®) or patiromer (Veltassa®) — novel potassium binders enabling continuation of renoprotective RAAS inhibitor therapy
- Loop diuretics (furosemide) to enhance renal potassium excretion
- Review medications — cease or reduce K⁺-sparing agents, NSAIDs, trimethoprim
Lifestyle and Dietary Measures
- Sodium restriction: <6 g NaCl/day (approximately 2.3 g sodium) — reduces blood pressure, proteinuria, and oedema.
- Protein intake: 0.75–1.0 g/kg/day for CKD G3–G4 (not on dialysis); avoid high-protein diets (>1.3 g/kg/day) which accelerate GFR decline. Increase to 1.0–1.2 g/kg/day on dialysis to prevent malnutrition.
- Phosphate restriction: 800–1000 mg/day for CKD G4–G5; avoid phosphate additives in processed foods.
- Exercise: ≥150 min/week moderate-intensity activity; improves cardiovascular fitness, blood pressure, insulin sensitivity, and quality of life.
- Smoking cessation: Essential — smoking accelerates CKD progression and doubles cardiovascular risk.
- Weight management: Target BMI 20–25 kg/m²; obesity contributes to glomerular hyperfiltration and nephropathy progression.
Nephrology Referral Criteria
- eGFR <30 mL/min/1.73 m² (G4–G5)
- Rapid decline in eGFR: >5 mL/min/1.73 m² per year, or >25% decline within 12 months
- Persistent albuminuria ACR ≥30 mg/mmol (A3), or rapidly rising albuminuria
- Uncertain aetiology — need for renal biopsy
- Resistant hypertension (≥4 agents at maximum tolerated doses)
- Recurrent nephrolithiasis or structural kidney disease
- Hereditary kidney disease (e.g., ADPKD, Alport syndrome)
- Planning for renal replacement therapy (pre-emptive transplant workup, dialysis access creation)
Renal Replacement Therapy (RRT)
When CKD progresses to ESKD (G5D, eGFR <10–15 mL/min/1.73 m² with uraemic symptoms), renal replacement therapy becomes necessary. Modality selection depends on patient preference, comorbidities, social circumstances, and geographic accessibility.
| Modality | Key Features | Access |
|---|---|---|
| Haemodialysis | Centre-based (3×/week, 4–5 hours) or home haemodialysis. Most common modality in Australia. | AV fistula (preferred), AV graft, central venous catheter |
| Peritoneal dialysis | CAPD (4 exchanges/day) or APD (overnight cycler). Home-based; better preservation of residual renal function. | Tenckhoff catheter |
| Kidney transplantation | Best long-term survival and quality of life. Living donor preferred; deceased donor waitlist 3–7 years in Australia. | Pre-emptive transplant possible before dialysis initiation |
| Conservative / supportive care | Appropriate for patients who decline RRT, have limited life expectancy, or significant comorbidities. Focus on symptom management, advance care planning, and palliative care. | N/A |
Investigations
A systematic approach to CKD investigation establishes diagnosis, identifies aetiology, stages disease severity, and assesses for complications. The following investigations should be performed at diagnosis and repeated at intervals determined by CKD stage and risk category.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements. 2013;3(1):1–150.
- 2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International. 2024;105(4S):S117–S314.
- 3. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 227. Canberra: AIHW; 2023.
- 4. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kid