📋 Key Information Summary
- Essential tremor (ET) is the most common movement disorder worldwide, affecting approximately 4% of adults over 40 years in Australia; prevalence increases with age.
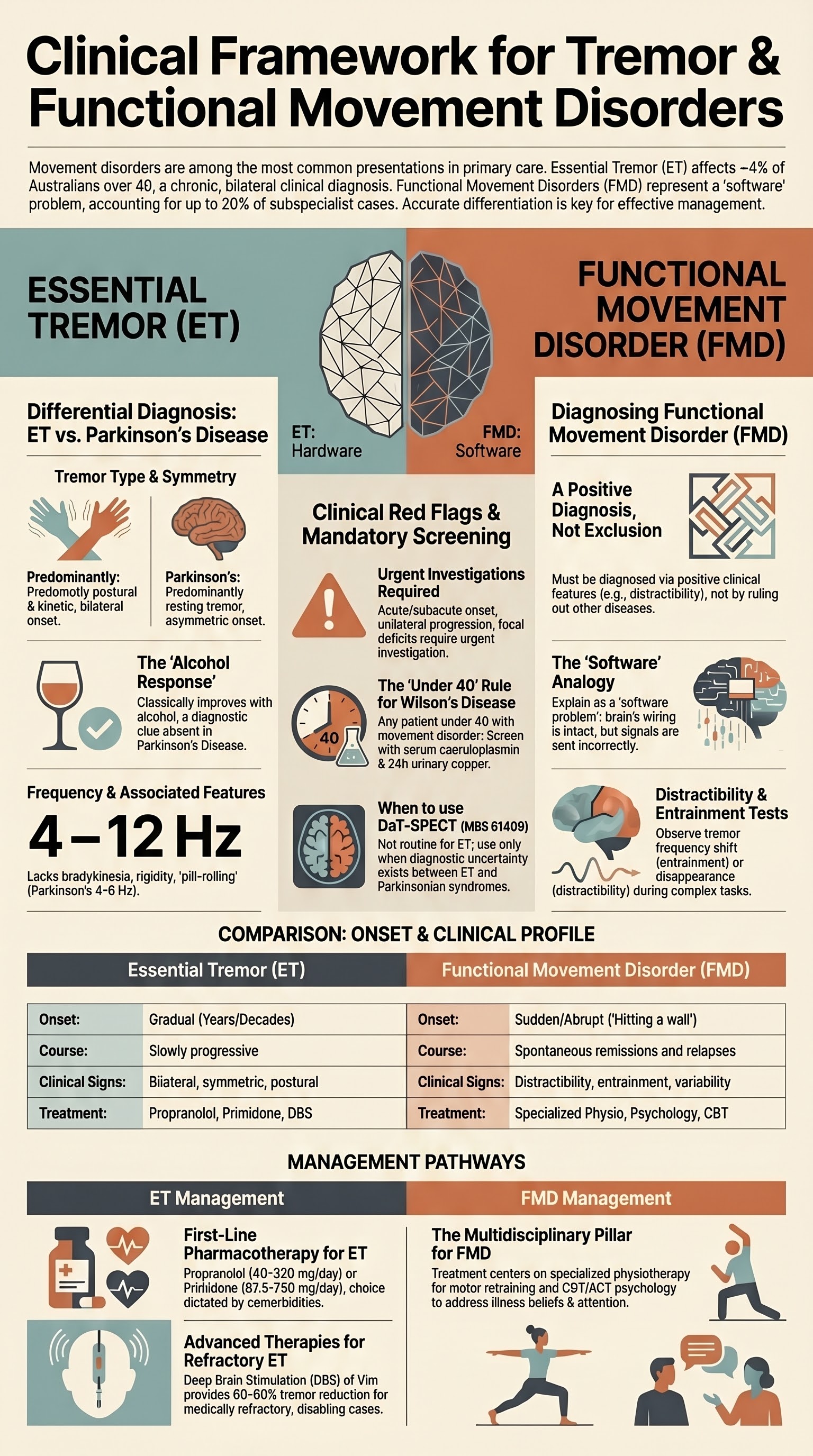
- ET is a clinical diagnosis — bilateral, symmetric postural and/or kinetic tremor of the hands and forearms lasting ≥3 years, with or without head/voice tremor, in the absence of other neurological signs.
- Key differentiating features from Parkinson's disease (PD) tremor: ET is predominantly postural/kinetic (not resting), symmetric (not unilateral), improves with small amounts of alcohol, and is not associated with bradykinesia or rigidity.
- Neuroimaging (MRI brain) is not routinely required for classic ET — consider imaging when atypical features are present (asymmetry, focal neurological signs, acute onset, age of onset <40 years).
- First-line pharmacotherapy for ET is propranolol (40–320 mg/day PO) or primidone (62.5–750 mg/day PO); choice depends on comorbidities, patient preference, and contraindications.
- Propranolol is contraindicated in severe asthma/COPD, heart block, and decompensated heart failure; start low (20 mg BD) and titrate slowly.
- Primidone should be initiated at a very low dose (62.5 mg nocte) and titrated slowly to minimise acute sedation, dizziness, and ataxia — up to 30% of patients cannot tolerate it.
- Second-line agents include topiramate, gabapentin, clonazepam, and botulinum toxin A (for head/voice tremor or refractory hand tremor); deep brain stimulation (DBS) of the ventral intermediate nucleus (Vim) is reserved for medically refractory, functionally disabling tremor.
- Functional movement disorders (FMD) are characterised by inconsistency, distractibility, entrainment, and positive clinical signs (e.g., Hoover's sign, co-contraction sign) — they are not diagnoses of exclusion.
- Diagnose FMD with confidence using positive clinical features; communicate the diagnosis clearly, explain the mechanism, and avoid language that implies the symptoms are feigned or "all in your head."
- Functional tremor — look for distractibility (tapping contralateral hand or performing mental arithmetic changes tremor amplitude), entrainment (tremor frequency shifts to match a cued rhythm), and variable amplitude that does not fit a classic neurological pattern.
- Referral to specialised physiotherapy (movement disorder-focused) and psychology (CBT, acceptance and commitment therapy) is the mainstay of FMD management — pharmacotherapy has limited evidence.
- Functional impact assessment is critical in both ET and FMD — use standardised tools (ET rating scales, PDQ-39 equivalent, WHODAS 2.0) to guide treatment decisions and determine eligibility for advanced therapies.
- Aboriginal and Torres Strait Islander Australians may face barriers to specialist assessment; consider telehealth-supported movement disorder clinics and culturally safe communication when discussing functional neurological symptoms.
Introduction & Australian Epidemiology
Tremor is defined as an involuntary, rhythmic, oscillatory movement of a body part and is the most common movement symptom encountered in primary care. Movement symptoms encompass a broader spectrum including tremor, myoclonus, dystonia, chorea, tics, and functional (psychogenic) movement disorders. This guideline focuses on essential tremor, its differentiation from Parkinsonian tremor, evidence-based treatment, and functional movement disorders — a frequently misdiagnosed but important cause of disabling movement symptoms.
In Australia, essential tremor affects an estimated 4–5% of adults aged over 40 years, with prevalence rising to 10–15% in those over 65 years. It is approximately four to ten times more prevalent than Parkinson's disease. The condition is associated with significant functional impairment, reduced quality of life, increased fall risk, and higher rates of social isolation, particularly in elderly populations.
Functional movement disorders account for approximately 2–5% of referrals to Australian movement disorder clinics and up to 15–20% of patients seen in subspecialist practice. They affect younger adults (mean age of onset 30–40 years) more frequently and are associated with significant disability and healthcare utilisation. Misdiagnosis rates remain high, and the average time from symptom onset to correct diagnosis exceeds 2–5 years in many series.
This article provides an Australian clinical framework for the assessment and management of essential tremor and functional movement disorders, aligned with current Therapeutic Guidelines (eTG), Australian and international movement disorder society recommendations, and PBS-listed treatment options.

Essential Tremor — Clinical Diagnosis
Definition & Diagnostic Criteria
Essential tremor (ET) is a chronic, bilateral, primarily symmetric postural and/or kinetic tremor involving the hands and forearms. The International Parkinson and Movement Disorder Society (MDS) consensus criteria (2018) classify ET into:
- ET — "Classic": Bilateral upper limb tremor (postural or kinetic) lasting ≥3 years, with or without tremor in other locations (head, voice, lower limbs), and no other neurological signs.
- ET-plus: ET with additional neurological signs of uncertain significance (e.g., mildly impaired tandem gait, questionable dystonic posturing, subtle memory complaints) — this category acknowledges the phenotypic heterogeneity of ET.
Clinical Assessment
A focused history and neurological examination are essential. Key elements include:
| Assessment Domain | Key Questions / Examination |
|---|---|
| Tremor onset & evolution | Gradual onset (years to decades); usually insidious; ask about family history (50% have affected first-degree relative, autosomal dominant with variable penetrance) |
| Tremor context | Postural (hands outstretched), kinetic (finger-to-nose, pouring water, drinking from a cup), writing, eating, speaking |
| Alcohol response | Classically improves with small amounts of ethanol — useful diagnostically but NOT a treatment strategy |
| Functional impact | Writing, eating, drinking, dressing, occupational tasks, driving, social embarrassment |
| Medications & substances | Exacerbating agents: sodium valproate, lithium, β-agonists, caffeine, corticosteroids, amiodarone |
| Neurological examination | Postural tremor (arms outstretched), kinetic tremor (finger-to-nose), rest tremor (hands relaxed in lap), tone, bradykinesia, gait, tandem walk, dystonic posturing |
Differentiation from Parkinson's Disease Tremor
| Feature | Essential Tremor | Parkinson's Disease Tremor |
|---|---|---|
| Tremor type | Postural and kinetic (predominantly); may have mild rest component in advanced disease | Resting (predominantly); may have postural component (re-emergent tremor) |
| Symmetry | Bilateral and symmetric | Asymmetric onset (ipsilateral to initial bradykinesia) |
| Frequency | 4–12 Hz (typically 6–8 Hz) | 4–6 Hz |
| Pill-rolling | No | Classic (thumb-index) |
| Alcohol response | Often improves | No improvement |
| Associated features | Head/voice tremor (may occur in isolation); no rigidity or bradykinesia | Bradykinesia, rigidity, postural instability, micrographia, masked facies |
| Family history | Positive in ~50% | Positive in ~15% |
| Head tremor | Common (yes-yes or no-no) | Uncommon |
When to Image
Neuroimaging is not routinely required for classic ET with typical features. Consider MRI brain when:
- Atypical features — asymmetric tremor, focal neurological signs, acute onset
- Age of onset <40 years (consider Wilson's disease, other structural causes)
- Diagnostic uncertainty between ET and PD — DaT-SPECT (dopamine transporter scan) may be considered to confirm nigrostriatal denervation in suspected PD; normal DaT-SPECT supports ET (available at major Australian nuclear medicine centres, MBS item 61409)
- Suspected structural cause (e.g., midbrain lesion, cerebellar pathology)
Investigations
Treatment of Essential Tremor
Principles of Management
Treatment should be guided by functional impact, not tremor amplitude alone. Many patients with mild ET require no pharmacotherapy. Treatment initiation is indicated when tremor interferes with activities of daily living (writing, eating, drinking, occupational tasks) or causes significant social distress. A shared decision-making approach, incorporating patient goals and preferences, is essential.
Functional Impact Assessment
Assess the functional impact of tremor before and during treatment using validated tools:
- Essential Tremor Rating Assessment Scale (TETRAS): Clinician-rated and patient-rated scales capturing performance and ADL impact — recommended by the MDS
- Quality of Life in Essential Tremor (QUEST): Patient-reported outcome measure for tremor-specific quality of life
- Functional Assessment: Ask specifically about writing, drinking from a cup, eating with utensils, using tools, using a smartphone, dressing, grooming, driving, and social/occupational participation
First-Line Pharmacotherapy
Second-Line Agents
Advanced / Surgical Therapy
Non-Pharmacological Strategies
- Weighted utensils and writing devices (weighted pens, adaptive cups)
- Occupational therapy for adaptive strategies and workplace modifications
- Avoidance of tremorogenic substances (caffeine, sympathomimetics)
- Stress management and anxiety treatment (anxiety worsens ET)
- Physiotherapy for balance and fall prevention in elderly patients with gait involvement
- Psychological support for social withdrawal and embarrassment
Functional Movement Disorders
Overview
Functional movement disorders (FMD), also termed psychogenic movement disorders, are characterised by involuntary movements that are clinically inconsistent, incompatible with recognised neurological disease, and associated with positive clinical signs. FMD is not a diagnosis of exclusion — it should be diagnosed on the basis of positive clinical features that demonstrate the functional nature of the symptoms. The DSM-5 classifies these as "Functional Neurological Symptom Disorder (Conversion Disorder)" with the specifier "with abnormal movement."
Clinical Clues to Diagnosis — Positive Signs
The following positive clinical signs help identify FMD with specificity. A single positive sign is supportive; multiple signs strengthen the diagnosis significantly.
| Positive Sign | Description | How to Elicit |
|---|---|---|
| Distractibility | Tremor amplitude decreases, changes character, or disappears during complex contralateral motor or cognitive tasks | Ask patient to tap fingers of the opposite hand in a complex rhythm, perform serial 7s, or name animals while observing tremor |
| Entrainment | Functional tremor changes frequency to match an externally cued rhythm | Ask patient to tap with the unaffected hand at a given frequency (e.g., 3 Hz, then 5 Hz); functional tremor will shift to match |
| Hoover's sign | Involuntary hip extension on the "weak" side is activated by contralateral hip flexion against resistance | Supine: test hip extension on the affected side (weak/absent); then ask patient to flex the contralateral hip against resistance — extension on the affected side re-emerges |
| Co-contraction sign | Simultaneous contraction of agonist and antagonist muscles producing rigidity that is not velocity-dependent | Passive movement of the affected limb — feel for co-contraction of both muscle groups simultaneously (unlike true rigidity which has a velocity-dependent quality) |
| Tremor variability | Tremor amplitude, frequency, or distribution changes significantly between observation periods or with attention directed to the affected limb | Observe tremor with the patient aware and unaware of being watched; compare tremor during conversation versus focused attention |
| Arm drop | When the affected arm is lifted and released, it falls slowly and avoids the face/body (inconsistent with true weakness) | Lift the patient's arm above the face and release — a genuinely weak arm falls onto the face; a functional arm diverts |
| Thigh abductor sign | In a patient with apparent leg weakness, hip abduction against resistance is possible when tested with the patient supine and the contralateral leg performing a different task | Test hip abduction strength in isolation (weak) versus during contralateral hip adduction against resistance |
Functional Tremor — Specific Features
- Sudden onset (often can recall the exact moment) with maximal severity at onset ("hitting a wall") — contrast with the gradual onset of ET
- Resting tremor that is also prominent on posture and kinetic tasks — does not follow a classical neurological pattern
- Spontaneous remissions and relapses with inconsistent distribution
- Associated with other functional neurological symptoms (weakness, sensory disturbance, non-epileptic seizures, gait disorder)
- Tremor may cease during contralateral rhythmic tapping (entrainment) or when attention is diverted
- Classic features of ET (symmetric postural/kinetic, family history, alcohol-responsive) are typically absent
Communication Strategies
The diagnostic conversation is the most important therapeutic intervention. Research consistently shows that a well-communicated diagnosis reduces symptoms, healthcare utilisation, and diagnostic uncertainty.
Investigations in FMD
The primary role of investigations is to exclude co-existing organic pathology, not to "diagnose" FMD (which is a clinical diagnosis). Avoid unnecessary or repeated investigations, which can reinforce health anxiety.
- Routine blood tests if not recently performed (TFTs, FBC, EUC, LFTs, glucose, calcium, magnesium)
- Brain MRI if any atypical features or diagnostic uncertainty
- EEG if non-epileptic seizures are part of the presentation
- Video recording of the movement disorder (with patient consent) — invaluable for demonstration of positive signs and for specialist review
- Avoid using investigations as the sole basis for diagnosis — a normal MRI does not confirm FMD any more than a normal MRI in ET
Management — Referral & Multidisciplinary Approach
The mainstay of FMD management is multidisciplinary rehabilitation. Evidence supports physiotherapy and psychological therapy as the two pillars of treatment.
Physiotherapy
- Referral to a physiotherapist with experience in neurological/functional movement disorders (not general physiotherapy)
- Focus on retraining automatic motor control — using attention-diverting strategies, graded motor relearning, and movement reprogramming
- Goals-based approach with measurable functional outcomes
- Sessions typically 1–2 times per week for 8–12 weeks with reassessment
- Available through public hospital outpatient departments (variable wait times 4–12 weeks) or privately (Medicare chronic disease management plan — 5 allied health sessions per year, MBS item 10950)
Psychology
- Referral to a psychologist experienced in functional neurological disorders
- Cognitive Behavioural Therapy (CBT) — evidence for functional neurological symptoms; addresses illness beliefs, avoidance behaviour, and symptom-focused attention
- Acceptance and Commitment Therapy (ACT) — emerging evidence; helps patients develop psychological flexibility around symptoms
- Trauma-informed assessment — some patients have comorbid PTSD, anxiety, or depression that may benefit from treatment
- Mental Health Treatment Plan (MHTP) — Medicare rebate for up to 10 psychology sessions per year (MBS item 80110)
- Avoid reflexive psychotropic prescribing — antidepressants are not first-line for FMD unless comorbid mood/anxiety disorder is present
Specialist Neurology Referral
- Referral to a movement disorder neurologist is recommended for diagnostic confirmation and ongoing management
- Many movement disorder specialists run dedicated FMD clinics in Australian capital cities
- Telehealth referral may be appropriate for regional and remote patients (MBS telehealth items available)
Pharmacotherapy in FMD
There is no established pharmacological treatment for FMD. Medications should target specific comorbidities:
- Comorbid depression: SSRI (e.g., sertraline 50–200 mg/day PO) — PBS General Benefit
- Comorbid anxiety: SSRI or SNRI; avoid benzodiazepines long-term
- Sleep disturbance: Sleep hygiene, address anxiety; short-term melatonin if needed
- Pain: Multimodal analgesia; avoid opioids
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Bhatia KP, Bain P, Bajaj N, et al. Consensus Statement on the classification of tremors. From the task force on tremor of the International Parkinson and Movement Disorder Society. Mov Disord. 2018;33(1):75-87.
- 2. Louis ED, Ferreira JJ. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor. Mov Disord. 2010;25(5):534-541.
- 3. Deuschl G, Raethjen J, Hellriegel H, Elble R. Treatment of essential tremor. Lancet Neurol. 2011;10(6):582-590.
- 4. Espay AJ, Lang AE, Erro R, et al. Essential pitfalls in "essential" tremor. Mov Disord. 2017;32(3):325-331.
- 5. Edwards MJ, Stone J, Lang AE. From psychogenic movement disorder to functional movement disorder: it's time to change the name. Mov Disord. 2014;29(7):849-852.
- 6. Espay AJ, Aybek S, Carson A, et al. Current concepts in diagnosis and treatment of functional neurological disorders. JAMA Neurol. 2018;75(9):1132-1141.
- 7. Stone J, Carson A, Duncan R, et al. Which neurologic diseases are most likely to be misdiagnosed? The "functional" neurological disorders. Neurology. 2016;86(4):396-397.
- 8. National Health and Medical Research Council (NHMRC). Australian Guidelines for the Prevention and Control of Infection in Healthcare. Canberra: NHMRC; 2019. [Referenced for national clinical governance frameworks].
- 9. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023. [Accessed for ATSI health data and service delivery context].
- 10. Zesiewicz TA, Elble R, Louis ED, et al. Evidence-based guideline update: Treatment of essential tremor. Neurology. 2011;77(19):1752-1755.
- 11. Carson A, Stone J, Hibberd C, et al. Disability, distress and unemployment in neurology outpatients with symptoms "unexplained by organic disease." J Neurol Neurosurg Psychiatry. 2011;82(7):810-813.
- 12. Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: a consensus recommendation. J Neurol Neurosurg Psychiatry. 2015;86(10):1113-1119.
- 13. Royal Australian College of General Practitioners (RACGP). Management of neurological conditions in general practice. East Melbourne: RACGP; 2020.
- 14. National Stroke Foundation. Clinical Guidelines for Stroke Management. Melbourne: Stroke Foundation; 2022. [Referenced for functional neurological symptom differential context].
- 15. Paviour DC, Jäger HR, Wilkinson L, Jahanshahi M, Lees AJ. Is the cervical dystonia tremor clinically distinguishable from essential tremor? Eur J Neurol. 2006;13(7):735-740.