📋 Key Information Summary
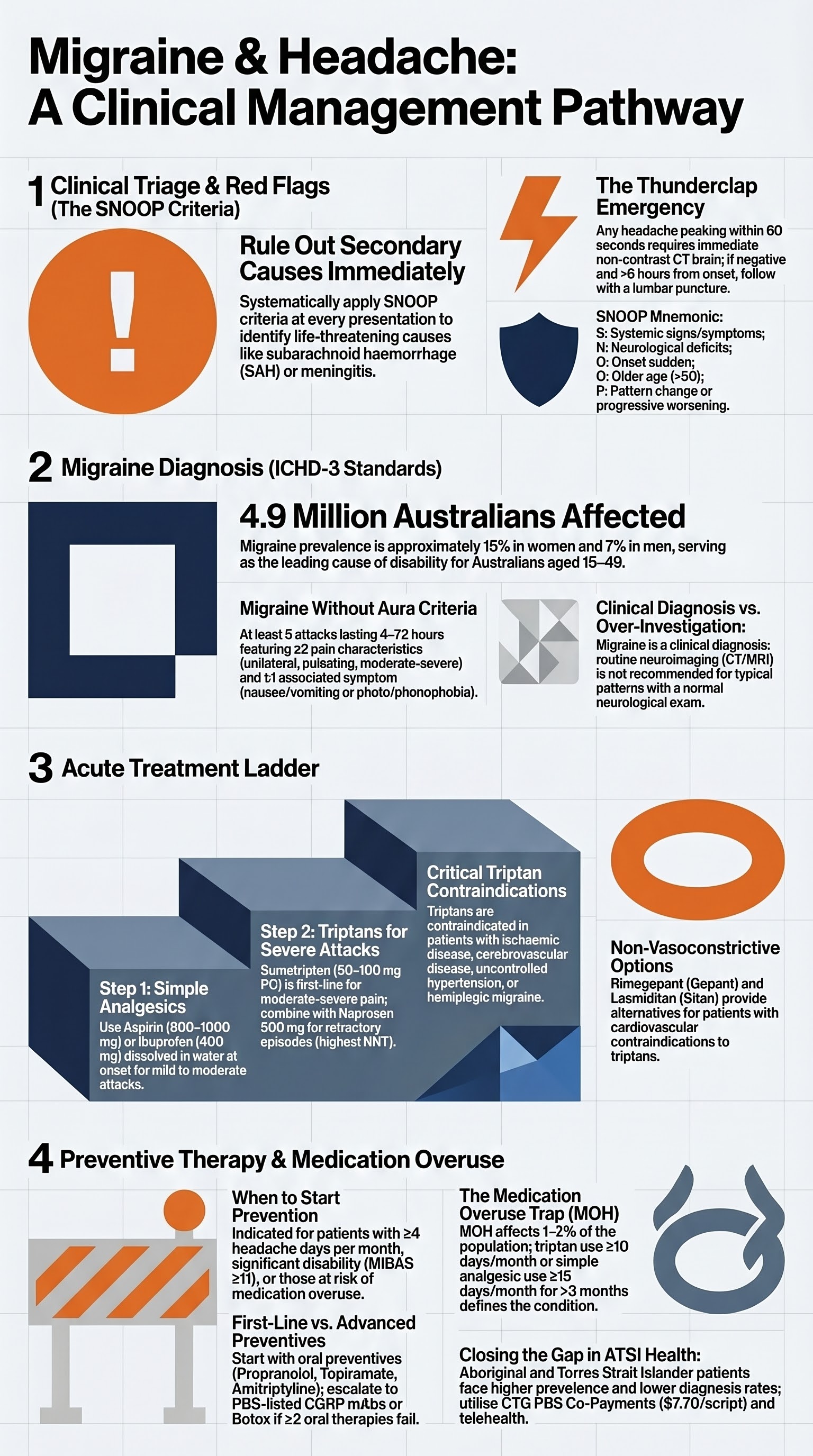
- Red flags demand urgent action: Apply SNOOP criteria (Systemic symptoms/signs, Neurological deficit, Onset sudden, Older age new onset, Pattern change) — thunderclap headache peaking within 1 minute requires immediate CT brain ± LP to exclude subarachnoid haemorrhage (SAH).
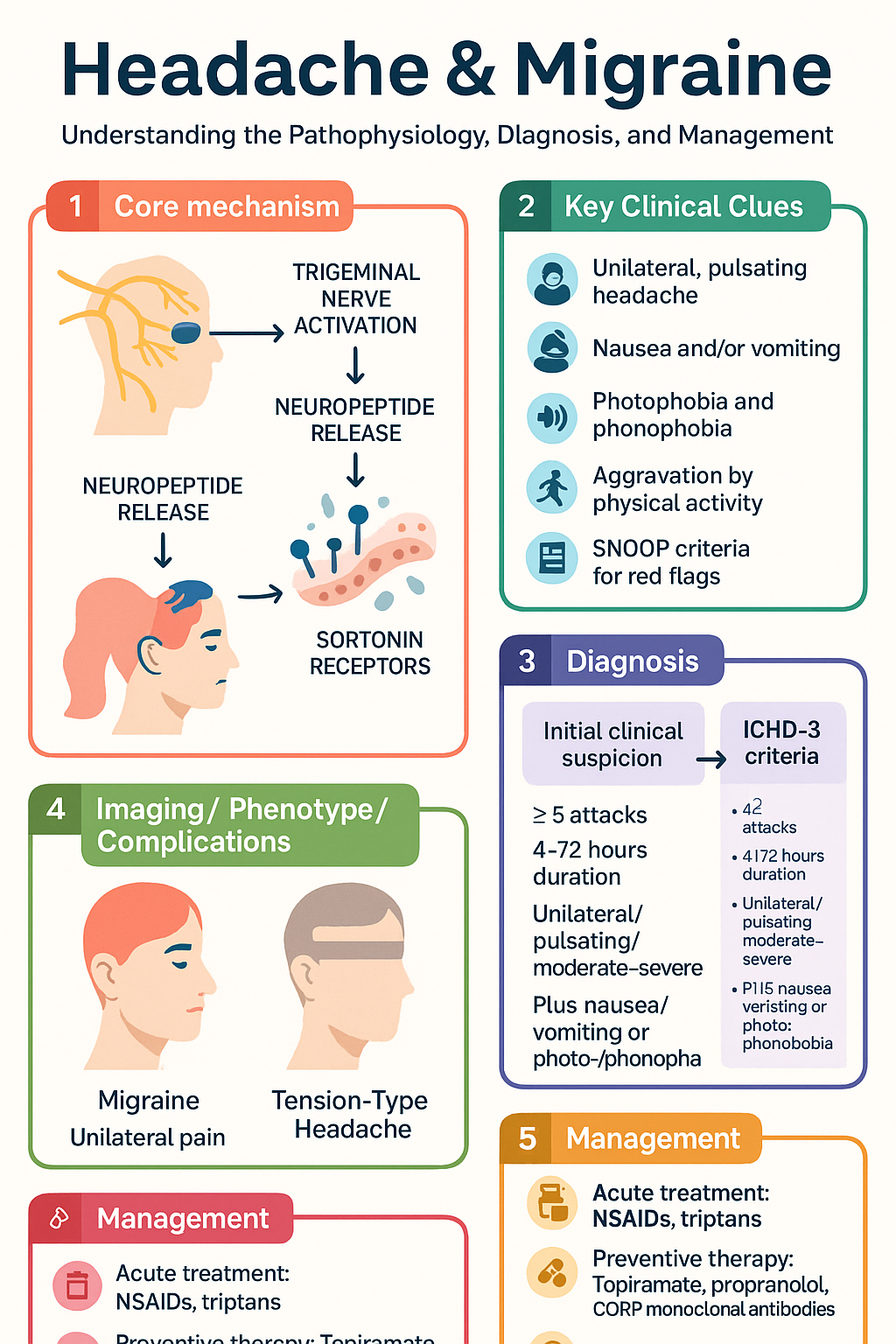
- Migraine is common in Australia: Affects approximately 4.9 million Australians (prevalence ~15% in women, ~7% in men); it is the second leading cause of years lived with disability globally and costs the Australian economy over $35 billion annually.
- ICHD-3 criteria govern diagnosis: ≥5 attacks for migraine without aura (4–72 h duration, ≥2 of unilateral/pulsating/moderate-severe/aggravated by activity, plus ≥1 of nausea/vomiting or photo-/phonophobia).
- Acute treatment ladder: Simple analgesics (aspirin 900–1000 mg or ibuprofen 400 mg) first-line; triptans (sumatriptan 50–100 mg PO or 6 mg SC) for moderate-severe attacks; combine triptan + NSAID for refractory episodes.
- Gepants and ditans expand options: Rimegepant (PBS-listed for acute and preventive use) and lasmiditan offer alternatives for patients with cardiovascular contraindications to triptans.
- Preventive therapy indicated when: ≥4 headache days/month, significant disability, or overuse of acute medications — topiramate, propranolol, amitriptyline, and CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab) are first-line preventives.
- CGRP monoclonal antibodies are PBS-listed: Available via Authority Required for chronic migraine (≥15 headache days/month, ≥8 migraine days) after failure of ≥2 oral preventives — erenumab 70–140 mg SC monthly, fremanezumab 225 mg SC monthly, galcanezumab 120 mg SC monthly.
- OnabotulinumtoxinA (Botox®) for chronic migraine: 155–195 units across 31 injection sites every 12 weeks — PBS Authority Required after ≥2 oral preventive failures.
- Medication overuse headache (MOH): Develops with ≥15 days/month use of acute medications — withdrawal of the offending agent is the cornerstone; bridge therapy with naproxen, prednisolone, or a transitional nerve block aids withdrawal.
- Triptan overuse carries highest MOH risk: ≥10 days/month of triptans, ergots, opioids, or combination analgesics; ≥15 days/month for simple analgesics — MOH affects ~1–2% of the general population and up to 50% of patients in headache clinics.
- Australian ATSI communities face disparities: Aboriginal and Torres Strait Islander peoples have higher headache prevalence, later presentation, less access to neurology and imaging, and greater use of over-the-counter analgesics — culturally safe care and GP-led management pathways are essential.
- Safety-critical: Triptans are CONTRAINDICATED in ischaemic heart disease, uncontrolled hypertension, cerebrovascular disease, and hemiplegic/basilar migraine. Always screen for cardiovascular risk before prescribing.
Introduction & Australian Epidemiology
Headache disorders are among the most common presentations in Australian primary care. Migraine alone affects approximately 4.9 million Australians and is the leading cause of disability in Australians aged 15–49 years. The Global Burden of Disease Study (2019) ranks migraine as the second highest cause of years lived with disability worldwide. In Australia, the economic burden exceeds $35 billion per year when indirect costs (lost productivity, carer burden) are included.
Despite its prevalence, migraine remains underdiagnosed and undertreated. Fewer than 50% of Australians with migraine consult a physician, and of those who do, many receive only over-the-counter analgesia without appropriate preventive strategies. Medication overuse headache (MOH) complicates management in up to 2% of the general population and represents a significant proportion of chronic daily headache presentations.
This guideline covers the recognition of headache red flags, evidence-based diagnosis of migraine according to ICHD-3 criteria, acute and preventive pharmacotherapy available on the Australian Pharmaceutical Benefits Scheme (PBS), management of medication overuse headache, and considerations for special populations including Aboriginal and Torres Strait Islander communities.
Headache Red Flags & Triage
The most critical task in headache assessment is identifying secondary causes that require urgent investigation or intervention. The SNOOP mnemonic and additional red-flag features should be systematically assessed at every presentation.
SNOOP Criteria for Headache Red Flags
| Letter | Criterion | Examples |
|---|---|---|
| S — Systemic | Systemic symptoms (fever, weight loss) or systemic risk factors (HIV, malignancy, immunosuppression) | Fever + headache → meningitis, encephalitis, brain abscess; known malignancy → brain metastases |
| N — Neurological | Focal neurological signs or altered mental status | Hemiparesis, visual field defect, ataxia, papilloedema, confusion, personality change |
| O — Onset sudden | Thunderclap headache — maximal intensity within 1 minute of onset | Subarachnoid haemorrhage, cerebral venous sinus thrombosis, arterial dissection, pituitary apoplexy, reversible cerebral vasoconstriction syndrome (RCVS) |
| O — Older age | New headache onset after age 50 years | Giant cell arteritis (temporal arteritis), space-occupying lesion, idiopathic intracranial hypertension |
| P — Pattern change | Progressive worsening, change in established headache pattern, or headache provoked by Valsalva/position/exertion | Raised intracranial pressure (worse in morning, with bending), Chiari malformation, CSF leak (positional) |
Additional Red-Flag Features Requiring Urgent Imaging or Referral
- Headache with papilloedema — suspect idiopathic intracranial hypertension (IIH) or space-occupying lesion; urgent MRI/MRV and ophthalmology review
- New headache with jaw claudication, visual disturbance, temporal tenderness, or elevated ESR/CRP in a patient >50 years — suspect giant cell arteritis (GCA); start prednisolone 1 mg/kg/day immediately, urgent rheumatology/ophthalmology referral, temporal artery biopsy
- Headache with fever, neck stiffness, and photophobia — suspect meningitis; blood cultures + empirical antibiotics (ceftriaxone 2 g IV) immediately; do not delay for CT/LP if meningococcal disease suspected
- Headache in immunocompromised patient (HIV, transplant, chemotherapy) — low threshold for CT/MRI and LP to exclude opportunistic infection, CNS lymphoma, or progressive multifocal leukoencephalopathy
- New headache with seizures — urgent CT/MRI to exclude space-occupying lesion, encephalitis, or cerebral venous sinus thrombosis
- Positional headache (worse upright, better supine) — suspect spontaneous intracranial hypotension (CSF leak); MRI brain with gadolinium, CT myelogram
When to Image — Summary Guide
| Clinical Scenario | Imaging | Urgency |
|---|---|---|
| Thunderclap headache | Non-contrast CT brain → LP if negative → CTA | Immediate (code stroke equivalent) |
| First severe headache with focal neurology | CT brain ± contrast, or MRI brain | Urgent (within 1 hour) |
| Suspected meningitis | Blood cultures → antibiotics → CT only if indicated before LP | Immediate |
| New daily persistent headache (NDPH) | MRI brain with contrast + MRV | Within 2 weeks |
| Chronic migraine without red flags — typical pattern | Imaging NOT routinely required | N/A |
| Suspected GCA | Temporal artery ultrasound or biopsy; urgent ophthalmology | Same day |
Migraine Diagnosis
Migraine diagnosis is clinical, based on the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria published by the International Headache Society (IHS). No biomarker or imaging study confirms migraine — it is diagnosed by history.
ICHD-3 Diagnostic Criteria: Migraine Without Aura
- A. ≥5 attacks fulfilling criteria B–D
- B. Headache lasting 4–72 hours (untreated or unsuccessfully treated)
- C. Headache has ≥2 of the following: unilateral location, pulsating quality, moderate or severe pain intensity, aggravation by or causing avoidance of routine physical activity
- D. During headache, ≥1 of: nausea and/or vomiting, photophobia and phonophobia
- E. Not better accounted for by another ICHD-3 diagnosis
ICHD-3 Diagnostic Criteria: Migraine With Aura
- A. ≥2 attacks fulfilling criteria B and C
- B. ≥1 of the following fully reversible aura symptoms: visual, sensory, speech/language, motor, brainstem, retinal
- C. ≥2 of: ≥1 aura symptom spreads gradually over ≥5 minutes, ≥2 aura symptoms occur in succession, each aura symptom lasts 5–60 minutes, aura accompanied or followed within 60 minutes by headache
- D. Not better accounted for by another ICHD-3 diagnosis
Migraine Subtypes
| Subtype | Definition | Key Features |
|---|---|---|
| Episodic migraine (EM) | <15 headache days/month | Low-frequency EM: <4 days/month; High-frequency EM: 4–14 days/month — high-frequency EM has highest risk of progression to chronic migraine |
| Chronic migraine (CM) | ≥15 headache days/month for >3 months, of which ≥8 are migraine days | Affects ~2% of migraineurs; significant disability; associated with medication overuse, obesity, depression, sleep disorders — eligible for PBS-listed CGRP mAbs and onabotulinumtoxinA |
| Menstrual migraine (MM) | Migraine without aura occurring on day −2 to +3 of menstruation in ≥2 out of 3 menstrual cycles | Pure menstrual migraine (attacks only around menses) vs menstrually-related migraine (also at other times); perimenstrual triptan prophaxis or frovatriptan 2.5 mg BD from day −2 to +4 |
| Hemiplegic migraine | Aura with motor weakness (familial or sporadic) | TRIPTANS CONTRAINDICATED; may require verapamil or lamotrigine; genetic testing for CACNA1A, ATP1A2, SCN1A |
| Basilar migraine | Aura with ≥2 brainstem symptoms (dysarthria, vertigo, tinnitus, diplopia, ataxia, bilateral visual symptoms) | TRIPTANS CONTRAINDICATED; now termed "migraine with brainstem aura" in ICHD-3 |
Headache Diary & Disability Assessment
Patients should maintain a headache diary for ≥8 weeks to document attack frequency, severity, duration, triggers, acute medication use, and menstrual cycle timing. Standardised tools include the Migraine Disability Assessment (MIDAS) questionnaire and the Headache Impact Test (HIT-6).
- MIDAS score 0–5: Minimal disability — acute treatment only
- MIDAS score 6–10: Mild disability — consider preventive therapy
- MIDAS score 11–20: Moderate disability — offer preventive therapy
- MIDAS score ≥21: Severe disability — initiate preventive therapy urgently
Acute Migraine Treatment
Acute migraine treatment should be stratified by attack severity. Early treatment (within 20 minutes of onset) is more effective. A stepwise approach from simple analgesics to specific anti-migraine agents is recommended.
Step 1 — Simple Analgesics (Mild to Moderate Attacks)
Step 2 — Triptans (Moderate to Severe Attacks)
Step 3 — Combination Therapy & Refractory Acute Treatment
Gepants (CGRP Receptor Antagonists)
Lasmiditan (5-HT₁F Agonist — Ditan)
Adjunctive Acute Therapies
Emergency Department Protocol for Refractory Migraine
Preventive Migraine Therapy
Preventive therapy is indicated when migraine frequency is ≥4 headache days/month, when acute treatments are insufficient or contraindicated, when quality of life is significantly impacted, or when medication overuse is developing. The goal is a ≥50% reduction in headache days per month. Treatment should be initiated at a low dose and titrated slowly over 2–3 months to minimise side effects.
First-Line Oral Preventives
CGRP Monoclonal Antibodies (PBS Authority Required)
OnabotulinumtoxinA for Chronic Migraine
Preventive Therapy Monitoring & Titration
| Parameter | Frequency | Details |
|---|---|---|
| Headache diary | Ongoing, reviewed monthly initially | Track headache days, migraine days, acute medication use, MIDAS score |
| Efficacy assessment | After 8–12 weeks at target dose | ≥50% reduction in monthly migraine days = adequate response; continue for 6–12 months then trial off |
| FBC / LFTs | Baseline, 3 months (topiramate, valproate, amitriptyline) | Valproate: FBC + LFTs; Topiramate: bicarbonate (metabolic acidosis); Amitriptyline: ECG if cardiac risk |
| Weight | Monthly for 3 months, then 3-monthly | Topiramate → weight loss (beneficial in obese patients); valproate/amitriptyline → weight gain |
| Blood pressure / HR | Baseline, 1 month, 3-monthly (β-blockers) | Propranolol: hypotension, bradycardia |
| Pregnancy test | Before each cycle (topiramate, valproate) | Both Category D — must confirm effective contraception |
Medication Overuse Headache (MOH)
Medication overuse headache (MOH) is defined by ICHD-3 as headache occurring on ≥15 days/month in a patient with a pre-existing primary headache disorder (usually migraine or tension-type headache) who has been overusing acute headache medications for >3 months. MOH affects approximately 1–2% of the general population and up to 50% of patients in tertiary headache clinics. It is the most common cause of chronic daily headache.
High-Risk Medications & Overuse Thresholds
| Medication Class | Overuse Threshold | MOH Risk |
|---|---|---|
| Simple analgesics (aspirin, paracetamol, NSAIDs) | ≥15 days/month for >3 months | Lower |
| Triptans | ≥10 days/month for >3 months | Highest — develops most quickly (median 1.7 years) |
| Ergotamines | ≥10 days/month for >3 months | High |
| Opioids | ≥10 days/month for >3 months | High — also promotes central sensitisation |
| Combination analgesics (codeine + paracetamol, caffeine-containing) | ≥10 days/month for >3 months | High — caffeine component contributes |
| Gepants | Not yet established; ≥18 days/month (provisional) | Low (emerging data) |
Withdrawal Strategy
Abrupt withdrawal is recommended for triptans, ergotamines, and simple analgesics. Gradual dose reduction over 2–4 weeks is appropriate for opioids and benzodiazepines. Patient education before withdrawal is essential to manage expectations — headache typically worsens for 1–2 weeks before improvement.
Bridge Therapy During Withdrawal
Patient Education — MOH
- The overused medication is CAUSING the chronic headache — not treating it
- Headache will temporarily worsen (for 1–2 weeks) after withdrawal before it improves
- After successful withdrawal, 50–70% of patients return to episodic headache patterns
- Restrict acute medication use to a maximum of 2 days per week (8–10 days/month)
- Initiate or optimise preventive therapy BEFORE or SIMULTANEOUSLY with withdrawal
- A headache diary is essential to track recovery and prevent relapse
Relapse Prevention
- After successful withdrawal, initiate or optimise preventive therapy (CGRP mAbs have the lowest MOH risk)
- Follow-up at 3, 6, and 12 months post-withdrawal
- Relapse rate: ~30–40% within 4 years — regular headache diary and ongoing GP follow-up essential
- Consider referral to headache specialist or neurologist for patients with refractory MOH
- Address comorbidities: anxiety, depression, sleep disorders, obesity — all independent risk factors for MOH relapse
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
Headache disorders, including migraine, are underrecognised and undertreated in Aboriginal and Torres Strait Islander communities. AIHW data indicate that First Nations Australians experience higher rates of headache-related presentations, greater use of over-the-counter analgesics, and reduced access to specialist neurology services, particularly in remote and very remote areas. Migraine prevalence in ATSI populations is estimated at 15–20%, yet fewer than 25% of those affected have received a formal migraine diagnosis.
- Utilise Aboriginal health practitioners and health workers for headache history-taking and patient education
- Complete a comprehensive MBS chronic disease management plan (item 721) that includes headache
- Access Closing the Gap PBS Co-Payment for affordable medications ($7.70/script)
- Use telehealth neurology (MBS items 99200/99203) for specialist referral where local services are unavailable
- Provide culturally adapted headache diaries and written patient information in local languages where available
- Advise on non-pharmacological approaches: sleep hygiene, stress management, regular meals, hydration — relevant to community context
- Screen for and manage comorbid mental health conditions that exacerbate migraine (MBS item 715 health assessment)
📚 References
- 1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
- 2. Steiner TJ, Stovner LJ, Jensen R, et al. Migraine remains second among the world's causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21(1):137.
- 3. Australian Institute of Health and Welfare (AIHW). Headache and migraine in Australia. Cat. no. PHE 321. Canberra: AIHW; 2023.
- 4. American Headache Society. Consensus statement: The use of triptans, gepants, and ditans in acute migraine treatment. Headache. 2021;61(6):891–895.
- 5. Diener HC, Holle D, Solbach K, Gaul C. Medication-overuse headache: risk factors, pathophysiology and management. Nat Rev Neurol. 2016;12(10):575–583.
- 6. Ailani J, Burch RC, Robbins MS. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache. 2021;61(7):1021–1039.
- 7. Buse DC, Reed ML, Fanning KM, et al. Comorbid and co-occurring conditions in migraine and associated risk of increasing headache days and medication overuse. Headache. 2020;60(1):128–144.
- 8. Australian Government Department of Health and Aged Care. Pharmaceutical Benefits Scheme (PBS) — Online PBS Medicine Listings. Canberra: Commonwealth of Australia; 2025. Available at: pbs.gov.au.
- 9. Dodick DW, Turkel CC, DeGryse RE, et al. OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the double-blind, randomised, placebo-controlled phases of the PREEMPT clinical programme. Headache. 2010;50(6):921–936.
- 10. Diener HC, Charles A, Goadsby PJ, Holle D. New therapeutic approaches for the prevention and treatment of migraine. Lancet Neurol. 2015;14(10):1010–1022.
- 11. Ashina M, Sazer D, Ashina S, et al. Migraine: epidemiology and systems of care. Lancet. 2021;397(10283):1485–1495.
- 12. Derry CJ, Derry S, Moore RA. Sumatriptan (all routes of administration) for acute migraine attacks in adults — overview of Cochrane reviews. Cochrane Database Syst Rev. 2014;(5):CD009108.
- 13. Lipton RB, Croop R, Stock EG, et al. Rimegepant, an oral calcitonin gene-related peptide receptor antagonist, for migraine. N Engl J Med. 2019;381(2):142–149.
- 14. Kuca B, Silberstein SD, Wietecha L, et al. Lasmiditan is an effective acute treatment for migraine: a phase 3 randomized study. Neurology. 2018;91(24):e2222–e2232.
- 15. Australian Government Department of Health and Aged Care. Closing the Gap PBS Co-Payment Program. Canberra: Commonwealth of Australia; 2024.
- 16. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 9th ed. Melbourne: RACGP; 2018.