📋 Key Information Summary
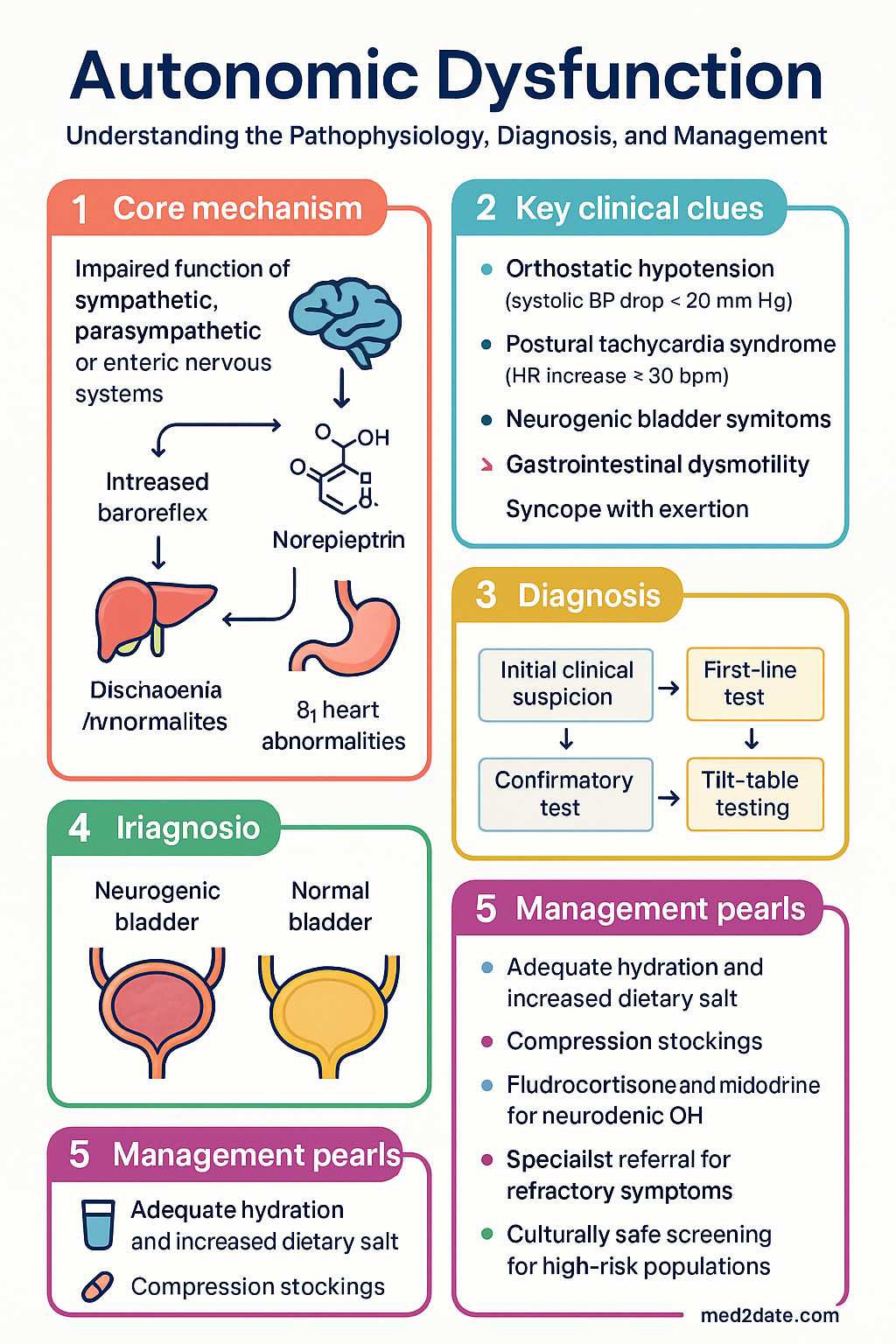
- Autonomic dysfunction encompasses orthostatic hypotension (OH), postural tachycardia syndrome (POTS), neurogenic bladder, and gastrointestinal dysmotility — all reflecting impaired involuntary nervous system regulation.
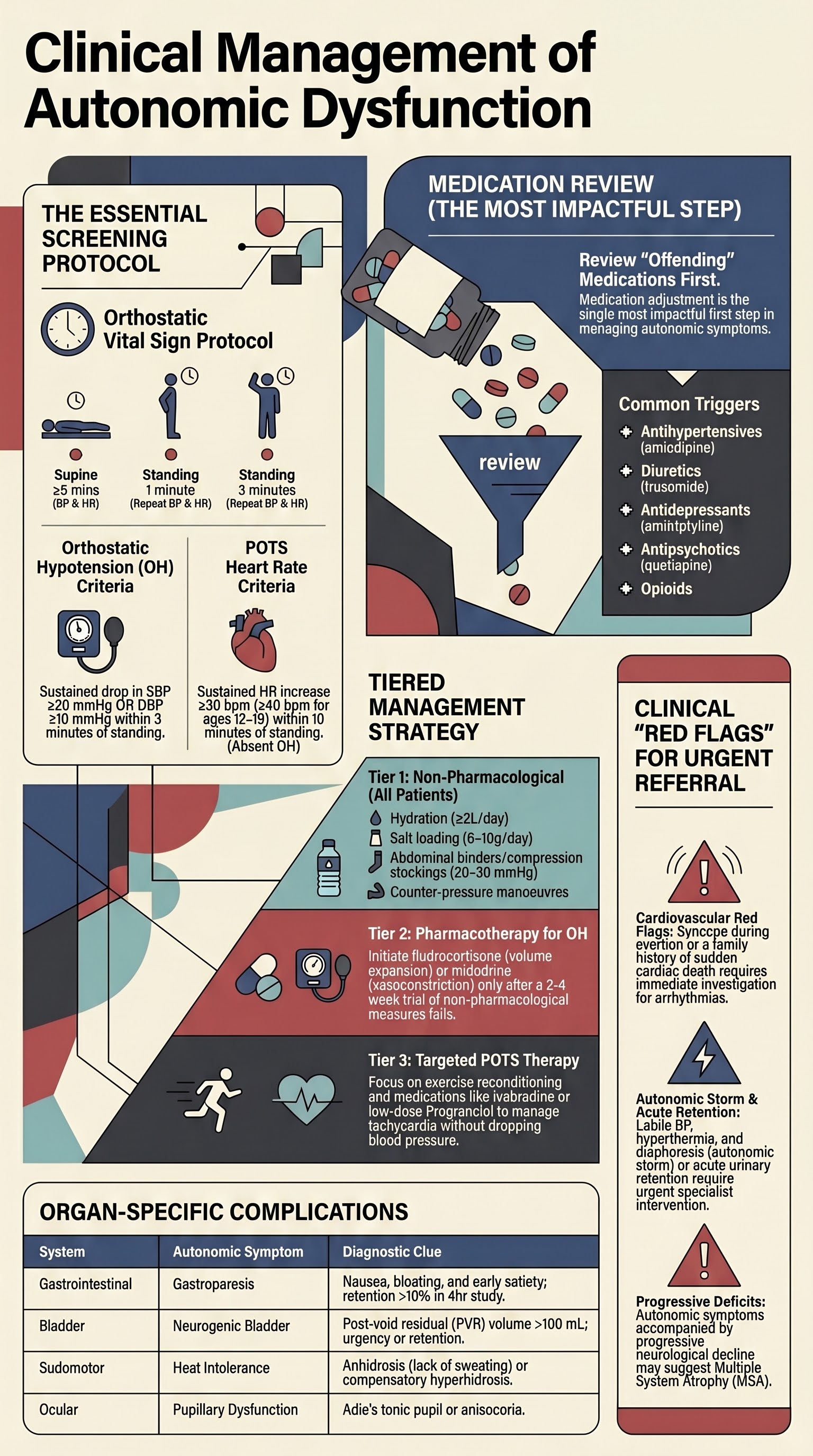
- Orthostatic hypotension is defined as a sustained drop in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing; always measure lying and standing BP as a minimum screening step.
- Medication review is the single most impactful first step — antihypertensives, diuretics, α-blockers, antidepressants, antipsychotics, and opioids are common offenders.
- Diabetes mellitus is the most common systemic cause of autonomic neuropathy in Australia; screen with HbA1c and consider cardiac autonomic reflex testing if symptomatic.
- Initial management of orthostatic symptoms includes adequate hydration (≥2 L/day), increased dietary salt (6–10 g/day if not contraindicated), compression stockings (knee-high 20–30 mmHg), and slow positional changes.
- Postural tachycardia syndrome (POTS) requires a heart rate increase ≥30 bpm (≥40 bpm in adolescents) within 10 minutes of standing without orthostatic hypotension — formal tilt-table testing confirms diagnosis.
- Fludrocortisone and midodrine are first-line pharmacological agents for neurogenic orthostatic hypotension; both are available on the PBS in Australia.
- Gastrointestinal autonomic symptoms (gastroparesis, constipation, faecal incontinence) require targeted workup including gastric emptying studies and anorectal physiology testing before specialist referral.
- Neurogenic bladder presents as urinary retention, frequency, urgency, or incontinence — post-void residual volume measurement is the essential bedside test; urodynamic studies guide definitive management.
- Red flags requiring urgent referral include syncope with exertion, recurrent unexplained falls in the elderly, new-onset autonomic storm (labile BP, hyperthermia, diaphoresis), and autonomic symptoms with progressive neurological deficits suggesting multiple system atrophy.
- Aboriginal and Torres Strait Islander Australians have higher rates of diabetes and renal disease, increasing autonomic neuropathy burden; culturally safe screening and remote-access pathways are essential.
- Refer to a neurologist with autonomic expertise or a dedicated autonomic laboratory when initial workup is non-diagnostic, symptoms are refractory, or a neurodegenerative cause (MSA, Parkinson's) is suspected.
Introduction & Australian Epidemiology
Autonomic dysfunction refers to a broad spectrum of disorders arising from impaired function of the sympathetic, parasympathetic, or enteric nervous systems. Symptoms span multiple organ systems — orthostatic intolerance, syncope, gastroparesis, constipation, bladder dysfunction, sudomotor abnormalities, and cardiovascular instability. In primary care, these symptoms are common but frequently under-recognised or attributed to other conditions, leading to delayed diagnosis and impaired quality of life.
In Australia, orthostatic hypotension affects approximately 5–10% of community-dwelling adults over 65 years and up to 30% of aged-care residents. The prevalence is substantially higher among people with diabetes mellitus, Parkinson's disease, and chronic kidney disease — all conditions with significant Australian burden. Diabetes alone affects over 1.3 million Australians (AIHW, 2023), and cardiac autonomic neuropathy is present in up to 73% of individuals with longstanding type 1 diabetes and 54% with type 2 diabetes.
Postural tachycardia syndrome (POTS) predominantly affects young women (female-to-male ratio ~5:1) and has gained increased recognition in Australia post-COVID-19, with emerging data suggesting SARS-CoV-2 as a trigger for autonomic dysregulation. Neurogenic bladder and gastrointestinal dysmotility are frequently encountered comorbidities in neurological conditions including multiple sclerosis, spinal cord injury, and diabetic neuropathy.
Pathophysiology
Normal Autonomic Function
The autonomic nervous system maintains homeostasis through a balance of sympathetic (fight-or-flight) and parasympathetic (rest-and-digest) tone. On standing, baroreceptors in the carotid sinus and aortic arch detect a transient fall in blood pressure, triggering sympathetic vasoconstriction and vagal withdrawal to maintain cerebral perfusion. The enteric nervous system independently coordinates gastrointestinal motility, while parasympathetic pathways via S2–S4 control bladder detrusor function.
Mechanisms of Dysfunction
- Neurogenic (primary autonomic failure): Degeneration of postganglionic sympathetic neurons (pure autonomic failure) or central autonomic pathways (multiple system atrophy, Parkinson's disease). Lewy body deposition disrupts brainstem cardiovascular centres.
- Peripheral autonomic neuropathy: Diabetic autonomic neuropathy (microvascular injury to vasa nervorum), amyloidosis (transthyretin or light-chain deposition), autoimmune (Guillain-Barré, autoimmune autonomic ganglionopathy with ganglionic acetylcholine receptor antibodies).
- Hyperadrenergic states (POTS): May reflect partial dysautonomia with peripheral denervation and compensatory sympathetic activation, hypovolaemia, deconditioning, or autoimmune-mediated mechanisms.
- Medication-induced: Pharmacological blockade of adrenergic, cholinergic, or dopaminergic pathways (e.g., antihypertensives, anticholinergics, dopamine antagonists).
- Secondary causes: Chronic kidney disease (uraemic autonomic neuropathy), autoimmune diseases (SLE, Sjögren's), paraneoplastic syndromes (anti-Hu antibodies), and hereditary conditions (familial dysautonomia, Fabry disease).
Organ-Specific Pathophysiology
| System | Normal Function | Autonomic Dysfunction |
|---|---|---|
| Cardiovascular | Baroreflex-mediated BP and HR stability on standing | Orthostatic hypotension, POTS, supine hypertension, syncope |
| Gastrointestinal | Coordinated peristalsis via enteric nervous system | Gastroparesis, constipation, faecal incontinence, small intestinal bacterial overgrowth |
| Bladder | Parasympathetic detrusor contraction coordinated with sphincter relaxation | Detrusor underactivity (retention), detrusor-sphincter dyssynergia, neurogenic overactivity |
| Sudomotor | Thermoregulatory sweating | Anhidrosis or compensatory hyperhidrosis; heat intolerance |
| Pupillary | Light reflex and accommodation | Adie's tonic pupil, anisocoria |
Screening & Basic Workup
Orthostatic Vital Signs — The Essential First Step
Measurement of lying and standing blood pressure and heart rate is the single most important screening test for autonomic dysfunction and should be performed in every patient presenting with dizziness, syncope, unexplained falls, or fatigue.
- Patient lies supine for ≥5 minutes; measure BP and HR.
- Patient stands (assisted if needed); measure BP and HR at 1 minute and 3 minutes.
- Orthostatic hypotension (OH): Systolic drop ≥20 mmHg or diastolic drop ≥10 mmHg within 3 minutes of standing.
- Heart rate criteria for POTS: Sustained HR increase ≥30 bpm (≥40 bpm if age 12–19) within 10 minutes of standing without OH; symptoms of orthostatic intolerance must be present.
- Record symptoms during standing (lightheadedness, visual dimming, palpitations, nausea).
Medication Review
A thorough medication reconciliation is imperative. The following medication classes are the most frequent contributors to autonomic symptoms in Australian primary care:
| Drug Class | Examples | Autonomic Effect | Action |
|---|---|---|---|
| Antihypertensives | Amlodipine, perindopril, irbesartan, prazosin, doxazosin | Exaggerated BP drop on standing | Dose reduction, timing adjustment (avoid nocturnal dosing if morning OH), consider agents with less orthostatic effect |
| Diuretics | Frusemide, hydrochlorothiazide, indapamide, spironolactone | Volume depletion, electrolyte disturbance | Review indication, reduce dose, ensure adequate oral hydration |
| Antidepressants | Amitriptyline, nortriptyline, sertraline, venlafaxine | Anticholinergic effects (dry mouth, urinary retention, constipation); noradrenergic effects (orthostatic hypotension) | Weigh risk-benefit; consider agents with fewer anticholinergic properties |
| Antipsychotics | Quetiapine, olanzapine, risperidone, clozapine | α-adrenergic blockade → OH; anticholinergic effects → urinary retention, constipation | Psychiatry co-review; dose timing; monitoring |
| Opioids | Oxycodone, morphine, tapentadol, codeine | Constipation (near-universal), nausea, urinary retention | Regular laxatives (macrogol, senna); consider opioid rotation; minimise duration |
| Anticholinergics | Oxybutynin, solifenacin, trospium, hyoscine | Constipation, urinary retention (paradoxically), dry mouth, cognitive effects | Review cumulative anticholinergic burden using Anticholinergic Cognitive Burden Scale |
| Dopamine antagonists | Metoclopramide, prochlorperazine, domperidone | Extrapyramidal effects; orthostatic hypotension | Limit duration; avoid in Parkinson's disease |
Screening for Diabetes and Systemic Causes
- Diabetes mellitus: HbA1c (if not known diabetic), fasting glucose. Diabetic autonomic neuropathy is the most common cause of chronic dysautonomia in Australia. Screen all patients with ≥5 years of diabetes for cardiac autonomic neuropathy using cardiovascular reflex tests.
- Thyroid dysfunction: TSH — both hyper- and hypothyroidism can mimic or exacerbate autonomic symptoms.
- Renal impairment: eGFR, electrolytes — uraemia causes autonomic neuropathy; electrolyte abnormalities (hyponatraemia, hyperkalaemia) contribute to orthostatic symptoms.
- Haematological: FBC — anaemia (iron deficiency, B12/folate deficiency) exacerbates orthostatic intolerance; macrocytosis may suggest B12 deficiency (associated with autonomic neuropathy).
- Autoimmune screen: ANA, anti-SSA/SSB (Sjögren's syndrome is a recognised cause of autonomic neuropathy); consider ganglionic acetylcholine receptor antibodies if autoimmune autonomic ganglionopathy is suspected (referred to specialist laboratory).
- Infectious: HIV serology, hepatitis B/C — if risk factors present; these can cause autonomic neuropathy.
- Paraneoplastic: Anti-Hu (ANNA-1) antibodies if suspected paraneoplastic autonomic neuropathy — refer to neurologist.
- Vitamin deficiency: B12, folate, thiamine — especially in the setting of alcohol use disorder, malnutrition, or post-bariatric surgery.
Focused History and Examination
- Orthostatic symptoms: Timing of dizziness (morning worse → volume depletion; postprandial → postprandial hypotension); relationship to meals, heat, exertion, alcohol.
- Syncope characterisation: Prodrome (presyncope with warmth, nausea, diaphoresis suggests vasovagal; sudden collapse without prodrome raises concern for cardiac syncope); position (standing vs. supine); triggers (micturition, defecation, cough, swallowing).
- Gastrointestinal: Early satiety, nausea, bloating (gastroparesis); constipation (<3 stools/week, straining); diarrhoea (may be overflow or autonomic diarrhoea); faecal incontinence.
- Bladder: Hesitancy, weak stream, incomplete emptying (retention); urgency, frequency, incontinence (overactivity); recurrent UTIs suggest incomplete bladder emptying.
- Sudomotor: Heat intolerance, anhidrosis, compensatory sweating, dry skin.
- Neurological red flags: Parkinsonism (rigidity, tremor, bradykinesia → Parkinson's disease or MSA); cerebellar ataxia (MSA-c); peripheral neuropathy (length-dependent sensory loss).
- Syncope during exertion or with family history of sudden cardiac death (arrhythmia risk).
- Autonomic storm: labile blood pressure, tachycardia, hyperthermia, diaphoresis (consider neuroleptic malignant syndrome, serotonin syndrome, phaeochromocytoma, autonomic dysreflexia in spinal cord injury).
- Acute urinary retention requiring catheterisation — urgent urology or neurology assessment.
- Progressive neurological symptoms with autonomic failure (MSA, paraneoplastic).
Clinical Presentation & Diagnostic Criteria
Orthostatic Hypotension (OH)
Orthostatic hypotension is defined as a sustained reduction in systolic blood pressure ≥20 mmHg or diastolic blood pressure ≥10 mmHg within 3 minutes of standing or head-up tilt at ≥60°. It may be asymptomatic or present with lightheadedness, visual blurring, neck ache ("coat-hanger" pain — trapezius/paraspinal muscle ischaemia), nausea, cognitive slowing, or frank syncope.
- Neurogenic OH: Due to impaired baroreflex-mediated vasoconstriction; associated with low supine noradrenaline levels; seen in Parkinson's disease, MSA, pure autonomic failure, diabetic neuropathy.
- Non-neurogenic OH: Due to volume depletion, medications, cardiac disease (aortic stenosis, heart failure); noradrenaline levels are typically elevated.
- Initial OH: Transient BP drop within 15 seconds of standing with rapid recovery; common in young people and rarely pathological.
Postural Tachycardia Syndrome (POTS)
POTS is characterised by an excessive increase in heart rate on standing without a significant drop in blood pressure, accompanied by chronic (≥6 months) orthostatic symptoms.
- Sustained HR increment ≥30 bpm within 10 min of standing or head-up tilt (≥40 bpm in ages 12–19 years).
- Absence of OH (BP drop does not meet OH criteria).
- Symptoms of orthostatic intolerance for ≥6 months (fatigue, lightheadedness, palpitations, cognitive difficulties, nausea).
- Symptoms worsen with standing and improve with recumbency.
- Absence of other conditions explaining tachycardia (dehydration, medications, anaemia, fever).
POTS subtypes include neuropathic (partial small-fibre denervation), hyperadrenergic (elevated standing noradrenaline ≥600 pg/mL), and hypovolaemic variants — subtype identification guides targeted therapy.
Syncope
Syncope is transient loss of consciousness due to global cerebral hypoperfusion with rapid, spontaneous recovery. Distinguish from non-syncopal causes of loss of consciousness (seizures, vertigo, hypoglycaemia, psychogenic pseudosyncope). Aetiological classification:
- Reflex (vasovagal): Most common; triggered by pain, emotion, prolonged standing, warm environments. Prodrome of nausea, warmth, pallor, diaphoresis.
- Orthostatic: Due to OH or POTS; occurs within minutes of standing.
- Cardiac: Arrhythmic (bradyarrhythmia, tachyarrhythmia, long QT) or structural (aortic stenosis, HOCM, PE); highest mortality risk — requires urgent investigation.
Gastrointestinal Autonomic Dysfunction
- Gastroparesis: Delayed gastric emptying without mechanical obstruction. Presents with nausea, vomiting, early satiety, bloating, upper abdominal pain. Most common cause: diabetes (29% of cases); also post-surgical (fundoplication, bariatric), idiopathic, and medication-related.
- Chronic constipation: Reduced stool frequency, hard stools, straining, incomplete evacuation. Autonomic causes include colonic inertia (reduced colonic motility) and dyssynergic defecation (incoordination of pelvic floor muscles).
- Faecal incontinence: May be due to internal anal sphincter denervation (autonomic) or external sphincter/pudendal nerve dysfunction (somatic); overlap is common.
- Small intestinal bacterial overgrowth (SIBO): Secondary to dysmotility; presents with bloating, diarrhoea, malabsorption, and nutritional deficiency.
Neurogenic Bladder
- Detrusor underactivity (underactive bladder): Impaired detrusor contraction leading to incomplete emptying, hesitancy, weak stream, recurrent UTIs, overflow incontinence. Common in diabetes, Parkinson's disease, MSA, spinal cord injury.
- Detrusor overactivity: Involuntary detrusor contractions causing urgency, frequency, urge incontinence. May coexist with sphincter dysfunction (detrusor-sphincter dyssynergia) in suprasacral spinal cord lesions.
- Autonomic dysreflexia: Life-threatening hypertensive crisis triggered by bladder distension or bowel impaction in patients with spinal cord injury at T6 or above. Requires immediate recognition and treatment.
Investigations
First-Line Investigations (Primary Care)
Gastrointestinal Investigations
Bladder Investigations
Specialist Autonomic Testing
Risk Stratification & Severity Scoring
Orthostatic Hypotension Severity
Syncope Risk Stratification (Canadian Syncope Risk Score)
The Canadian Syncope Risk Score (CSRS) stratifies patients presenting to the ED with syncope into low, medium, and high risk for 30-day serious adverse events. High-risk features include abnormal ECG, elevated troponin, history of heart disease, systolic BP <90 mmHg at triage, and physician diagnosis of vasovagal syncope excluded.
POTS Functional Impairment
Initial Management
Non-Pharmacological Interventions — First-Line for All Patients
Pharmacological Management — Orthostatic Hypotension
Adjunctive Agents for Orthostatic Hypotension
Pharmacological Management — POTS
Gastrointestinal Autonomic Symptom Management
| Symptom | First-Line | Second-Line / Referral |
|---|---|---|
| Gastroparesis | Dietary modification (small, frequent, low-fat, low-fibre meals; liquid nutrition if severe). Metoclopramide 10 mg PO/IM TDS AC (max 5 days in acute setting — risk of tardive dyskinesia with chronic use). Domperidone 10 mg PO TDS AC (preferred in Parkinson's — does not cross BBB; TGA Special Access Scheme if not PBS-listed). | Gastric electrical stimulation (Enterra™ — compassionate use at selected Australian centres). Botulinum toxin injection into pylorus (limited evidence; available endoscopically). Erythromycin 40–200 mg PO TDS AC (prokinetic via motilin receptor; short-term use due to tachyphylaxis). Gastroenterology referral. |
| Constipation | Adequate fluid and fibre (soluble fibre: psyllium husk 1 TDS). Macrogol 3350 (Movicol®) 1–3 sachets/day. Docusate + senna 1–2 tablets nocte. Osmotic laxatives (lactulose 15–30 mL BD). | Prucalopride (Resotran®) 2 mg PO daily (5-HT₄ agonist; stimulates colonic motility; Authority Required for chronic constipation failing other laxatives). Biofeedback therapy for dyssynergic defecation (available at major hospitals). Linaclotide (Constella®) 290 mcg PO daily (guanylate cyclase-C agonist). |
| Faecal incontinence | Pelvic floor physiotherapy (first-line for all). Bulking agents (psyllium). Anti-diarrhoeal (loperamide 2–4 mg PRN, max 16 mg/day). Bowel habit training (scheduled toileting after meals). | Sacral nerve stimulation (InterStim™) — available at major centres (Royal Melbourne, RPAH). Anal sphincter repair if structural defect on endoanal ultrasound. MDT: gastroenterology, colorectal surgery, pelvic floor physiotherapy. |
Bladder Autonomic Symptom Management
| Symptom / Pattern | First-Line | Second-Line / Specialist |
|---|---|---|
| Overactive bladder / urgency | Bladder retraining (scheduled voiding, gradual increase in intervals). Pelvic floor exercises. Solifenacin 5–10 mg PO daily, or mirabegron (Betmiga®) 50 mg PO daily (β₃ agonist — less anticholinergic side effects). Oxybutynin (Kentera® patch 3.9 mg/24h — transdermal avoids first-pass anticholinergic effects). | Botulinum toxin A (Botox® 100 units intravesical injection via cystoscopy — MBS item 36826). Sacral neuromodulation. Urology referral. |
| Urinary retention / underactive bladder | Clean intermittent self-catheterisation (CISC) — first-line for chronic retention; teach technique with continence nurse specialist. Timed voiding / double voiding. Alpha-blocker: tamsulosin 400 mcg PO daily (if bladder outlet obstruction component). | Suprapubic catheter if CISC not feasible. Sacral nerve stimulation. Intradetrusor botulinum toxin for detrusor-sphincter dyssynergia (specialist). Urology referral mandatory for PVR >300 mL or recurrent UTIs. |
- Orthostatic symptoms with normal bedside testing and negative basic workup — requires tilt-table testing and cardiovascular reflex tests.
- Suspected POTS — confirm diagnosis and subtype with tilt-table test + standing catecholamines.
- Suspected neurodegenerative autonomic failure (MSA, Parkinson's) — specialist neurological assessment and autonomic function testing.
- Refractory symptoms despite optimised non-pharmacological and first-line pharmacological management.
- Suspected autoimmune autonomic ganglionopathy — requires antibody testing and immunotherapy initiation.
Autonomic Laboratory Referral Centres in Australia
| State | Centre | Services |
|---|---|---|
| NSW | Royal North Shore Hospital (Sydney Autonomic Laboratory) | HUTT, CARTs, QSART, TST |
| NSW | Royal Prince Alfred Hospital / University of Sydney | HUTT, CARTs, small-fibre assessment |
| VIC | The Alfred Hospital / Monash University | HUTT, CARTs, sweat testing |
| VIC | Royal Melbourne Hospital / Florey Institute | HUTT, CARTs, QSART, skin biopsy |
| SA | Royal Adelaide Hospital | HUTT, CARTs |
| QLD | Royal Brisbane and Women's Hospital | HUTT, CARTs |
| WA | Fiona Stanley Hospital / Sir Charles Gairdner Hospital | HUTT (limited access — via neurology referral) |
Directed / Pathogen-Specific Therapy
Diabetic Autonomic Neuropathy
Glycaemic control is the primary disease-modifying strategy. In type 1 diabetes, intensive glucose control reduces the incidence of autonomic neuropathy by approximately 50% (DCCT/EDIC). In type 2 diabetes, the effect is more modest but sustained multifactorial risk factor management (glycaemia, BP, lipids) is beneficial (Steno-2 trial).
- Cardiac autonomic neuropathy (CAN): Independent predictor of mortality. Screen annually with cardiovascular reflex tests (deep breathing HR variability is most sensitive). Refer to endocrinology/cardiology if confirmed. ACE inhibitors (perindopril) and statins may have neuroprotective effects beyond BP/lipid lowering.
- Gastroparesis: Adjust insulin timing (administer after meals when gastric emptying is unpredictable). Use continuous glucose monitoring (CGM) to detect postprandial hypoglycaemia from delayed nutrient absorption. Co-manage with endocrinologist and gastroenterologist.
Autoimmune Autonomic Ganglionopathy (AAG)
AAG is caused by antibodies against the ganglionic nicotinic acetylcholine receptor (gAChR). It presents with subacute onset of severe pandysautonomia (orthostatic hypotension, anhidrosis, fixed pupils, gastroparesis, urinary retention, sicca symptoms). High antibody titres (>0.20 nmol/L) correlate with severity.
Other immunotherapies used in refractory AAG include plasma exchange (PLEX), corticosteroids, rituximab, and mycophenolate — all under specialist immunology or neurology supervision.
Multiple System Atrophy (MSA)
MSA is a progressive neurodegenerative disease with autonomic failure as a core feature, combined with parkinsonism (MSA-P) or cerebellar ataxia (MSA-C). There is no disease-modifying therapy. Management is symptomatic:
- OH: Fludrocortisone + midodrine + droxidopa as tolerated (see above).
- Supine hypertension: Short-acting antihypertensive at night (losartan 50 mg nocte, captopril 25 mg nocte, or transdermal nitroglycerin patch applied at night and removed in the morning).
- Stridor: Continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP); consider botulinum toxin injection into vocal cord abductors; tracheostomy in advanced cases.
- Bladder dysfunction: CISC preferred; avoid anticholinergics if detrusor underactivity.
- Palliative care: Early integration of palliative care services; advance care planning discussion early in the disease course (median survival 6–10 years from symptom onset).
Parkinson's Disease Autonomic Dysfunction
Autonomic symptoms are near-universal in advanced Parkinson's disease and may precede motor symptoms by years. Management approaches:
- Review PD medications — dopamine agonists and levodopa worsen OH. Avoid sudden dose reductions (risk of akinetic crisis).
- Fludrocortisone and midodrine as above.
- Droxidopa is particularly useful in PD-related neurogenic OH.
- Consider atomoxetine (Strattera®) 18–80 mg PO daily — noradrenaline reuptake inhibitor; emerging evidence for PD-related OH.
- Constipation: Prevalence >60%. Macrogol first-line. Prucalopride if refractory.
- Gastroparesis: Impairs absorption of levodopa — timing of medication and meals becomes critical. Consider liquid levodopa formulations.
- Sialorrhoea: Glycopyrrolate (glycopyrronium) 1 mg PO BD or botulinum toxin injection into salivary glands.
Monitoring
Primary Care Monitoring Framework
Monitoring Specific Agents
| Agent | Monitoring Parameter | Frequency | Stop/Modify If |
|---|---|---|---|
| Fludrocortisone | Serum K⁺, supine BP, weight, ankle oedema | 2 weeks post-initiation; then monthly × 3; then 3-monthly | K⁺ <3.0 mmol/L, supine BP >180/100, heart failure, significant oedema |
| Midodrine | Supine BP (must be measured), standing BP, urinary symptoms | 1 week post-initiation; then monthly × 3 | Supine BP >180/110, urinary retention, severe bradycardia |
| Ivabradine | Resting HR, ECG, visual symptoms | 2 weeks post-initiation; then 3-monthly | Resting HR <50 bpm, visual disturbances persistent, QTc prolongation |
| DDAVP | Serum sodium, daily weight, fluid balance | 3 days, 1 week, then monthly | Na⁺ <130 mmol/L, weight gain >1 kg, headache (hyponatraemia symptom) |
| Propranolol | Resting HR, BP, exercise tolerance, mood | 2 weeks; then 3-monthly | Resting HR <50, worsening fatigue, bronchospasm |
Falls Prevention
Autonomic dysfunction is an independent risk factor for falls, particularly in the elderly. Australian falls prevention guidelines (ACSQHS) recommend:
- Multifactorial falls risk assessment (balance, gait, vision, cognition, medications, home environment).
- Home hazard assessment and modification (Occupational Therapy referral — MBS item 10950 for chronic disease management plans).
- Exercise programme targeting balance and strength (e.g., Otago Exercise Programme, tai chi — available through community health services).
- Hip protectors in high-risk aged-care residents.
- Review and minimise psychoactive medications (sedatives, anticholinergics, opioids).
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a significantly higher burden of autonomic dysfunction due to the disproportionate prevalence of its underlying causes — particularly type 2 diabetes (3.7 times the rate of non-Indigenous Australians), chronic kidney disease, rheumatic heart disease, and cardiovascular disease (AIHW, 2023). Diabetic autonomic neuropathy is a major contributor to the excess cardiovascular mortality seen in Indigenous communities.
- Integrate lying-standing BP measurement into all chronic disease checks for Aboriginal and Torres Strait Islander patients with diabetes, cardiovascular disease, or CKD.
- Use the Closing the Gap PBS co-payment exemption to ensure affordable access to fludrocortisone, midodrine, and other relevant medications.
- Collaborate with ACCHOs and Aboriginal Health Workers to deliver culturally safe autonomic symptom education, falls prevention, and bladder/bowel health programmes.
- Leverage Patient Assisted Travel Schemes (PATS) for regional/remote patients requiring specialist autonomic testing at metropolitan centres.
- Include autonomic symptom screening in Annual Health Checks (MBS item 715) for Aboriginal and Torres Strait Islander peoples.
📚 References
- 1. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69-72.
- 2. Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41-e63.
- 3. Spallone V, Ziegler D, Freeman R, et al. Cardiovascular autonomic neuropathy in diabetes: clinical impact, assessment, diagnosis, and management. Diabetes Metab Res Rev. 2011;27(7):639-653.
- 4. Shibao C, Okamoto LE, Biaggioni I. Pharmacotherapy of autonomic failure. Pharmacol Rev. 2012;64(4):935-956.
- 5. Low PA, Tomalia VA, Park KJ. Autonomic function tests: some clinical applications. J Clin Neurol. 2013;9(1):1-8.
- 6. Vernino S, Low PA, Fealey RD, et al. Autoimmune autonomic ganglionopathy and ganglionic acetylcholine receptor antibodies. N Engl J Med. 2008;358(12):1262-1268.
- 7. Raj SR, Black BK, Biaggioni I, et al. Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome: less is more. Circulation. 2009;120(9):725-734.
- 8. Arnold AC, Ng J, Raj SR. Treatment of postural tachycardia syndrome: a comparison of octreotide and midodrine. Clin Auton Res. 2016;26(6):391-397.
- 9. Fanciulli A, Stankovic I, Krismer F, et al. Multiple system atrophy. Nat Rev Dis Primers. 2019;5(1):85.
- 10. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian facts. Canberra: AIHW; 2023. Cat. no. CVD 85.
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 12. Galbraith S, Cameron H, Begg D. Orthostatic hypotension in the elderly: a practical approach. Aust J Gen Pract. 2020;49(12):822-828.
- 13. Camilleri M, Parkman HP, Shafi MA, et al. Clinical guideline: management of gastroparesis. Am J Gastroenterol. 2013;108(1):18-37.
- 14. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Urology. 2003;61(1):37-49.
- 15. Sheldon RS, Morillo CA, Krahn AD, et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011;27(2):246-253.