📋 Key Information Summary
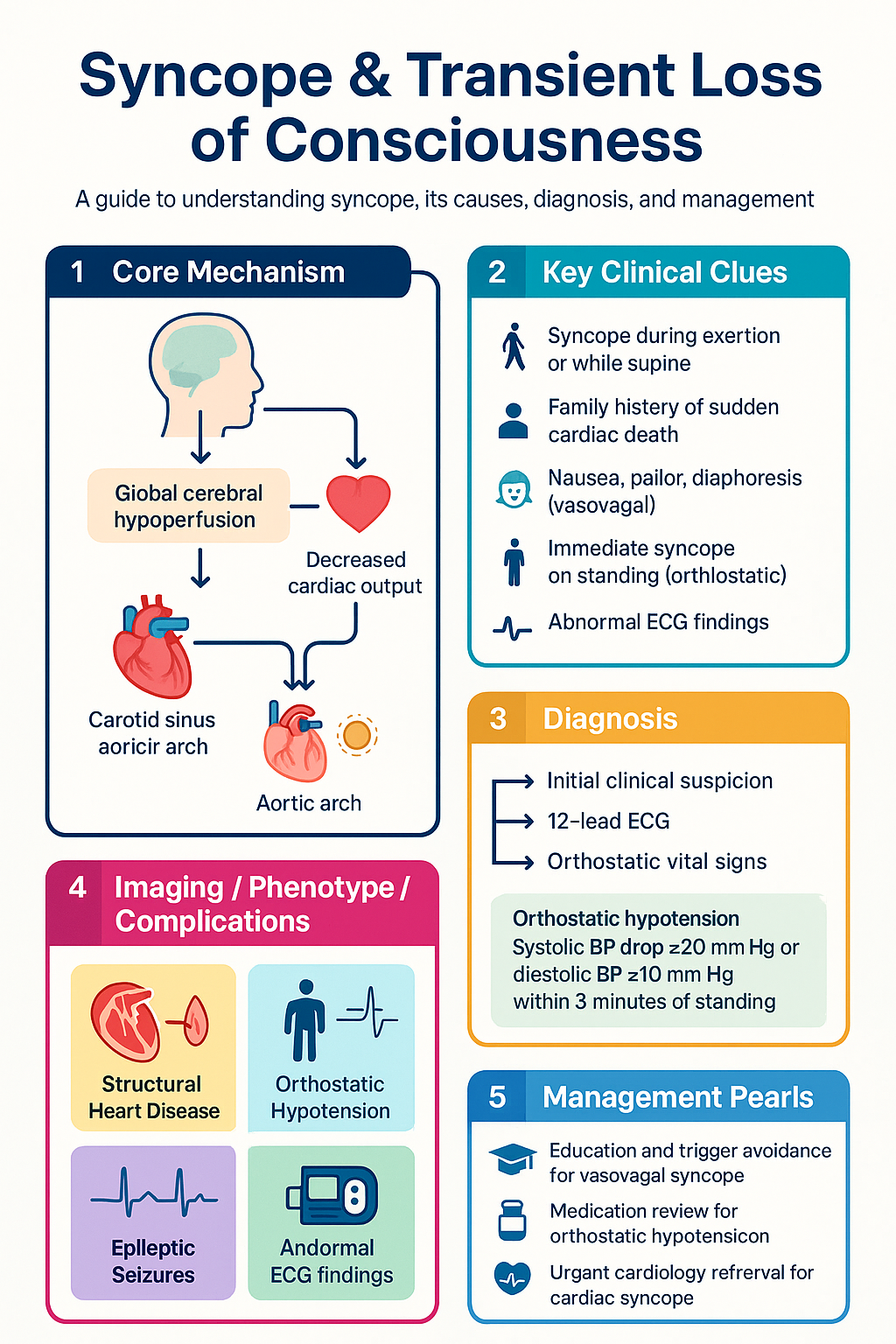
- Syncope is a transient loss of consciousness (TLOC) due to global cerebral hypoperfusion, with rapid onset, short duration, and spontaneous complete recovery.
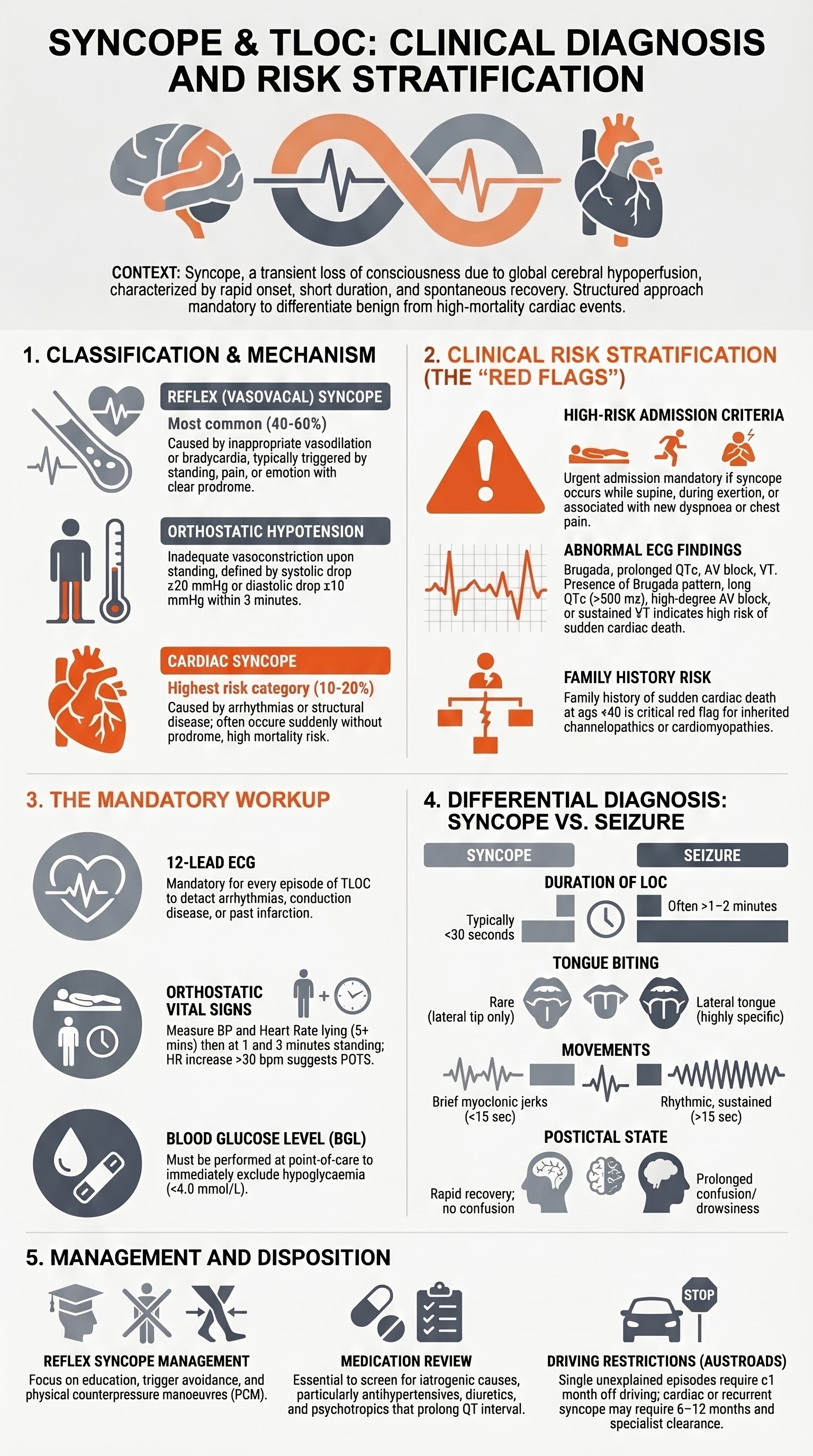
- Cardiac syncope carries the highest mortality risk (up to 30% 1-year mortality in structural heart disease) and always warrants urgent investigation and often admission.
- Reflex (vasovagal) syncope is the most common cause overall, typically benign, and managed with education, trigger avoidance, and physical counterpressure manoeuvres.
- Orthostatic hypotension is diagnosed with a sustained drop in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing, or systolic BP <90 mmHg.
- A 12-lead ECG is mandatory for every episode of TLOC; abnormal ECG findings (prolonged QT, Brugada pattern, AV block, ventricular pre-excitation) mandate urgent cardiology referral.
- High-risk features requiring admission include syncope during exertion or while supine, family history of sudden cardiac death <40 years, new or unexplained dyspnoea, severe structural/coronary heart disease, and haemodynamic instability.
- Neuroimaging and EEG are NOT routine for syncope; order only when there are focal neurological signs, prolonged confusion, or features suggestive of seizure or stroke.
- Medication review is essential — antihypertensives, diuretics, antidepressants, and antipsychotics are common iatrogenic contributors to orthostatic and reflex syncope.
- Driving restrictions apply: Austroads guidelines recommend ≥1 month off driving for a single unexplained syncope episode, and ≥6–12 months for recurrent or cardiac syncope.
- In Aboriginal and Torres Strait Islander populations, delayed presentation, higher burden of cardiovascular disease, and remote access barriers increase syncope-related morbidity and mortality.
- Orthostatic vital signs (lying and standing BP/HR at 1 and 3 minutes) should be performed in every patient presenting with syncope unless the cause is clearly vasovagal.
Introduction & Australian Epidemiology
Transient loss of consciousness (TLOC) is defined as a spontaneous, temporary loss of consciousness with complete recovery. Syncope — TLOC due to global cerebral hypoperfusion — accounts for approximately 1–3% of all emergency department (ED) presentations in Australia and up to 6% of acute medical admissions. It is a leading cause of hospital referral from primary care and carries significant diagnostic and prognostic complexity.
In Australia, syncope-related ED presentations total over 100,000 annually, with a peak incidence in older adults (>65 years). The direct healthcare cost is substantial: approximately $2.4 billion per year including ambulance transport, ED attendance, inpatient investigation, and specialist follow-up. Up to 40% of patients remain undiagnosed after initial ED evaluation.
The differential diagnosis is broad and includes true syncope (cardiac, reflex, orthostatic), epileptic seizures, psychogenic pseudosyncope, and rare causes such as subarachnoid haemorrhage or vertebrobasilar ischaemia. Accurate classification is critical because prognosis and management differ dramatically.
Classification of TLOC
| Type | Mechanism | Proportion | Mortality Risk |
|---|---|---|---|
| Reflex (vasovagal) | Inappropriate vasodilation ± bradycardia | ~40–60% | Very low |
| Orthostatic hypotension | Inadequate compensatory vasoconstriction on standing | ~10–30% | Low–moderate |
| Cardiac syncope | Arrhythmia, structural disease, or acute cardiac event | ~10–20% | High (up to 30% at 1 year) |
| Unknown / unexplained | Uncertain despite evaluation | ~15–30% | Variable |
Pathophysiology
Cerebral autoregulation normally maintains constant cerebral blood flow (CBF) across a mean arterial pressure (MAP) range of approximately 60–150 mmHg. Syncope occurs when MAP falls below the lower autoregulatory threshold, typically at a systolic BP of ~50–60 mmHg, causing global cerebral hypoperfusion lasting >6–8 seconds.
Reflex (Vasovagal) Syncope
Triggered by prolonged standing, emotional distress, pain, or venepuncture. The Bezold–Jarisch reflex mediates a paradoxical bradycardia and vasodilation via vagal afferents. Prodromal symptoms (nausea, pallor, diaphoresis, visual dimming) are typical and reflect the gradual haemodynamic decline. Tilt-table testing can provoke this response in susceptible individuals.
Orthostatic Hypotension
Gravity-dependent pooling of 500–1000 mL of blood in the lower limbs on standing reduces venous return. Normally, baroreceptors in the carotid sinus and aortic arch trigger sympathetic activation to maintain BP. Failure of this reflex — due to autonomic neuropathy (diabetes, Parkinson disease), volume depletion, or vasodilatory medications — results in sustained hypotension.
Cardiac Syncope
Arrhythmic syncope (bradyarrhythmias, supraventricular tachycardia, ventricular tachycardia) reduces cardiac output abruptly. Structural causes (aortic stenosis, hypertrophic cardiomyopathy, cardiac tamponade, pulmonary embolism) limit the heart's ability to increase output in response to demand. Both mechanisms produce sudden-onset LOC often without prodrome.
History & Risk Stratification
A thorough history is the single most important diagnostic tool in syncope. Witnesses should be contacted where possible. The history should aim to classify syncope as reflex, orthostatic, or cardiac, and identify high-risk features that mandate admission and urgent investigation.
Essential Historical Features
| Domain | Suggests Reflex Syncope | Suggests Cardiac Syncope | Suggests Orthostatic |
|---|---|---|---|
| Position | Prolonged standing, sitting upright | Supine or during exertion | Immediately on standing |
| Prodrome | Nausea, warmth, pallor, diaphoresis (>30 sec) | None or brief palpitations | Gradual lightheadedness, visual greying |
| Onset | Gradual | Sudden | Seconds after postural change |
| Recovery | Rapid, no confusion | May be prolonged if low cardiac output | Rapid once supine |
| Triggers | Pain, emotion, warm environment, venepuncture | Exertion, chest pain preceding | Dehydration, medications, morning |
| Injury | Infrequent (often collapsed onto something) | Common (sudden LOC, lacerations) | Occasional |
High-Risk Clinical Features
- Syncope during exertion or while supine
- Family history of sudden cardiac death at <40 years of age
- New or unexplained dyspnoea
- Severe structural heart disease or known reduced ejection fraction
- ECG abnormalities: sustained ventricular tachycardia, high-degree AV block, Brugada pattern, long QTc (>500 ms), ventricular pre-excitation, Q waves suggesting infarction
- Persistent hypotension (systolic <90 mmHg)
- Syncope associated with chest pain or palpitations
- Severe aortic stenosis or hypertrophic cardiomyopathy
Risk Stratification Tools
The San Francisco Syncope Rule and the Canadian Syncope Risk Score (CSRS) assist in identifying patients safe for discharge. The CSRS stratifies patients into low (≤−1), medium (0–3), and high (≥4) risk categories at 30 days for serious adverse events. In Australian EDs, clinical gestalt combined with ECG findings remains the predominant approach, supplemented by these validated scores.
History Red Flags — Seizure vs Syncope Differentiation
| Feature | Syncope | Seizure |
|---|---|---|
| Tongue biting | Lateral tip (if at all) | Lateral tongue (highly specific) |
| Duration of LOC | <30 seconds typically | >1–2 minutes |
| Tonic-clonic movements | Brief myoclonic jerks (<15 sec) may occur | Sustained >15 seconds, rhythmic |
| Postictal confusion | Rapid recovery, no confusion | Prolonged (>5 min) confusion/drowsiness |
| Cyanosis | Pallor | Cyanosis during event |
| Incontinence | Rare (urinary only) | Urinary ± faecal, more common |
Basic Workup
The workup should be targeted and guided by the clinical history and risk stratification. Routine extensive investigation of every syncopal episode is low-yield and not cost-effective. Australian emergency and primary care guidelines recommend a stepwise approach.
Core Investigations
Neuroimaging and EEG — When to Order
| Investigation | Indication | When NOT to Order |
|---|---|---|
| CT Brain (non-contrast) | Head injury from syncope, focal neuro signs, suspected SAH, anticoagulated patient with trauma | Routine syncope workup without red flags |
| MRI Brain | Focal neuro deficit, suspected posterior fossa lesion, recurrent unexplained TLOC with seizure features | Classic vasovagal syncope, orthostatic hypotension |
| CT Angiography (head/neck) | Suspected vertebrobasilar ischaemia, posterior circulation TIA features | Typical syncope without vertebrobasilar symptoms |
| EEG | Prolonged post-event confusion (>5 min), witnessed tonic-clonic activity >15 sec, recurrent unexplained LOC with seizure features, tongue biting (lateral) | Brief myoclonic jerks during syncope, classic vasovagal, orthostatic syncope |
Recommended Initial Workup Pathway
Clinical Presentation & Diagnostic Criteria
Reflex (Vasovagal) Syncope
Classic presentation: young adult in a warm, crowded environment, or in the setting of pain, emotion, or venepuncture. Prodrome of nausea, pallor, lightheadedness, and visual dimming for 30 seconds to a few minutes, followed by LOC lasting <30 seconds. Rapid recovery with no postictal features. Three subtypes: vasodepressor (predominant hypotension), cardioinhibitory (predominant bradycardia/asystole), and mixed.
Situational Syncope
A subtype of reflex syncope triggered by specific situations: micturition syncope (nocturnal, male), defaecation syncope, cough syncope (COPD, smokers), swallowing syncope, post-exercise syncope. Each has a distinct vagal trigger mechanism.
Carotid Sinus Syncope
Predominantly in men >50 years. Reproducible syncope or presyncope with carotid sinus massage — defined as asystole >3 seconds and/or systolic BP drop >50 mmHg. Diagnosed by carotid sinus massage under continuous monitoring. Must exclude significant carotid stenosis prior to testing.
Orthostatic Hypotension
Diagnosed when systolic BP falls ≥20 mmHg or diastolic BP falls ≥10 mmHg within 3 minutes of standing, or any systolic BP <90 mmHg on standing. Initial orthostatic hypotension occurs within 15 seconds of standing (common in young men), while classical orthostatic hypotension occurs at 1–3 minutes. Delayed orthostatic hypotension (>3 minutes) may indicate progressive autonomic failure.
Cardiac Arrhythmic Syncope
Bradyarrhythmic syncope (sinus node dysfunction, high-degree AV block, pacemaker malfunction) or tachyarrhythmic syncope (VT, SVT with rapid ventricular response, torsades de pointes). Typically sudden onset, may occur supine, minimal or no prodrome. Recovery may be rapid but associated with injury. The ECG or cardiac monitor is often diagnostic.
Structural Cardiac Causes
Aortic stenosis (exertional syncope + systolic murmur), hypertrophic cardiomyopathy (young athlete, family history SCD), cardiac tamponade (raised JVP, pulsus paradoxus), acute pulmonary embolism (pleuritic chest pain, tachycardia, hypoxia), aortic dissection (tearing chest pain, BP differential).
Management Strategies
Acute Management of Syncope in the ED
Management by Syncope Type
Reflex (Vasovagal) Syncope
Management is primarily non-pharmacological and patient education is the cornerstone. Most patients require no medication.
- Education: Reassurance, explanation of benign nature, recognition of prodromal symptoms
- Trigger avoidance: Prolonged standing, dehydration, warm/crowded environments, excessive alcohol
- Increase fluid intake: 2–3 L water/day (1.5 L bolus over 15 min before prolonged standing on waking)
- Increase dietary salt: 6–10 g NaCl/day (unless contraindicated by hypertension, heart failure, renal disease)
- Physical counterpressure manoeuvres (PCM): Leg crossing with muscle tensing, squatting, handgrip exercises — effective in prodromal phase
- Tilt training: Standing against a wall for 15–30 min daily — limited evidence but low risk
- Midodrine: 5–10 mg PO TDS (avoid late evening dose). α₁-agonist. PBS Authority Required (Section 100). Evidence: moderate, reduces syncope burden in recurrent vasovagal syncope.
- Fludrocortisone: 0.1–0.2 mg PO daily. Mineralocorticoid. Volume expansion. PBS General Benefit. Limited evidence in vasovagal syncope; more useful in orthostatic hypotension.
- SSRIs (sertraline, paroxetine): Small studies suggest benefit. Not first-line. May modulate central serotonergic pathways involved in autonomic control.
Orthostatic Hypotension
- Treat underlying cause: Volume repletion (IV normal saline if dehydrated), correct anaemia, review and withdraw offending medications.
- Non-pharmacological: Rise slowly, avoid prolonged recumbency, elastic compression stockings (waist-high), sleep with head of bed elevated 10–20°, increase fluid (2–3 L/day) and salt intake (8–10 g/day), squat to stand manoeuvres.
- Pharmacological: Midodrine 5–10 mg PO TDS (first-line), fludrocortisone 0.1–0.2 mg PO mane (second-line, monitor for hypertension and hypokalaemia), droxidopa 100–600 mg PO TDS (specialist use, limited PBS access).
Cardiac Syncope — Definitive Treatment
| Cause | Treatment |
|---|---|
| Sick sinus syndrome | Permanent pacemaker (dual-chamber preferred) |
| High-degree AV block (Mobitz II, complete) | Permanent pacemaker |
| Supraventricular tachycardia | Catheter ablation (first-line for AVNRT/AVRT) or rate/rhythm control |
| Ventricular tachycardia (sustained) | ICD implantation (if EF ≤35%), catheter ablation, antiarrhythmic drugs (amiodarone, sotalol) |
| Severe aortic stenosis | Aortic valve replacement (surgical or TAVI) |
| Hypertrophic cardiomyopathy + high risk | ICD implantation (risk stratify with HCM Risk-SCD calculator) |
| Acute pulmonary embolism | Anticoagulation (heparin → DOAC), thrombolysis if massive with haemodynamic compromise |
Medication Review
A thorough medication review is a critical component of syncope management, particularly in older adults and patients with orthostatic hypotension. The following medication classes are commonly implicated:
| Drug Class | Mechanism of Syncope | Action |
|---|---|---|
| Antihypertensives (diuretics, ACEi, ARBs, CCBs, α-blockers) | Volume depletion, excessive vasodilation | Dose reduction or cessation; switch to shorter-acting agent |
| Psychotropics (TCAs, SSRIs, antipsychotics, benzodiazepines) | Orthostatic hypotension, QT prolongation | Review indication, consider alternatives, monitor QTc |
| Anti-anginals (nitrates, β-blockers) | Vasodilation, bradycardia | Dose adjustment; avoid abrupt β-blocker cessation |
| Opioids | Vasodilation, orthostatic hypotension | Reduce dose, consider non-opioid analgesia |
| Phosphodiesterase-5 inhibitors (sildenafil, tadalafil) | Vasodilation, especially with nitrates | Absolute contraindication with nitrates; counselling |
| Diabetes medications (insulin, sulfonylureas) | Hypoglycaemia | Review targets, adjust doses, educate on recognition |
Driving & Occupational Advice
- Single vasovagal syncope: No driving restriction (private vehicle). Commercial licence: 1 month off driving.
- Recurrent vasovagal syncope: Private licence: cease driving until controlled (minimum 1 month). Commercial licence: minimum 3 months off, until 12 months recurrence-free.
- Unexplained syncope: Private licence: minimum 1 month off driving. Commercial licence: minimum 6 months off, requires specialist assessment.
- Cardiac syncope (arrhythmic/structural): Private licence: minimum 1 month (or as per specific cardiac condition). Commercial licence: minimum 6–12 months; specialist review required.
- Orthostatic syncope: Cease driving until cause identified and treated. Private licence: minimum 1 month.
Occupational hazards: Patients in safety-critical roles (pilots, heavy machinery operators, commercial drivers, crane operators) require formal occupational health and specialist assessment before return to work. Notify the relevant authority if required by state legislation.
Follow-Up and Disposition
- Low-risk (discharged from ED): GP follow-up within 1–2 weeks. Review ECG and bloods. Reinforce lifestyle measures. Return precautions.
- Moderate-risk (observed): Outpatient cardiology or syncope clinic referral within 2–4 weeks. Arrange Holter/loop recorder if indicated.
- High-risk (admitted): Cardiology consultation during admission. Discharge with clear follow-up plan, specialist appointment within 1–2 weeks. ICD/pacemaker assessment if indicated.
- Recurrent unexplained syncope: Consider syncope unit referral (available in some tertiary centres: Royal Melbourne, Westmead, Royal Adelaide). Implantable loop recorder if ≥2 unexplained episodes.
Special Populations
Pregnancy
Paediatrics
Elderly (>65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a significantly higher burden of cardiovascular disease, rheumatic heart disease, diabetes-related autonomic neuropathy, and chronic kidney disease — all of which contribute to increased syncope risk. Delayed presentation, cultural and linguistic barriers, and limited access to specialist services in remote and very remote areas compound the challenge of syncope evaluation and management.
- Rheumatic heart disease (RHD): ATSI Australians have among the highest rates of RHD globally. Valvular disease (particularly mitral stenosis) and associated arrhythmias are important cardiac causes of syncope in this population. Auscultation and echocardiography should be considered early.
- Diabetes-related autonomic neuropathy: Type 2 diabetes prevalence is 3–4 times higher in ATSI populations. Autonomic neuropathy causing orthostatic hypotension is underrecognised.
- Acute rheumatic fever (ARF): Recurrent ARF can cause progressive valvular disease. Syncope in a young ATSI person warrants cardiac evaluation to exclude RHD complications.
- Chronic kidney disease: ATSI Australians are 4 times more likely to have CKD. Electrolyte disturbance and volume-related syncope are common.
📚 References
- 1. Shen W-K, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017;136(5):e60–e122. doi:10.1161/CIR.0000000000000499
- 2. Brignole M, Moya A, de Lange FJ, et al. 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883–1948. doi:10.1093/eurheartj/ehy037
- 3. Sheldon RS, Amuah JE, Connolly SJ, et al. Design and use of a quantitative score for the evaluation of syncope in the emergency department. CMAJ. 2021;193(45):E1733–E1741. doi:10.1503/cmaj.210464
- 4. Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. CMAJ. 2016;188(12):E289–E298. doi:10.1503/cmaj.151469
- 5. Austroads. Assessing Fitness to Drive. Sydney: Austroads; 2022. Available at: austroads.com.au
- 6. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Canberra: AIHW; 2023.
- 7. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 8. Anderson NE, Kerr BJ, Sethi R, et al. Syncope presentations to Australian emergency departments: epidemiology and outcomes. Emerg Med Australas. 2022;34(5):714–721.
- 9. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection and management of heart failure in Australia. 2018 (updated 2024).
- 10. Sutton R, de Jong JSY, Stewart JM, et al. Persistent problem of syncope-related morbidity and mortality: the fainting fallacy. Europace. 2023;25(4):1365–1372. doi:10.1093/europace/euad048
- 11. Clinical Excellence Commission (NSW). Recognition and Management of Deteriorating Patients (Between the Flags). Sydney: CEC; 2022.
- 12. Roy Morgan Research. Syncope and falls in the elderly: Australian burden of disease analysis. Melbourne: AIHW Injury Research Series; 2021.