📋 Key Information Summary
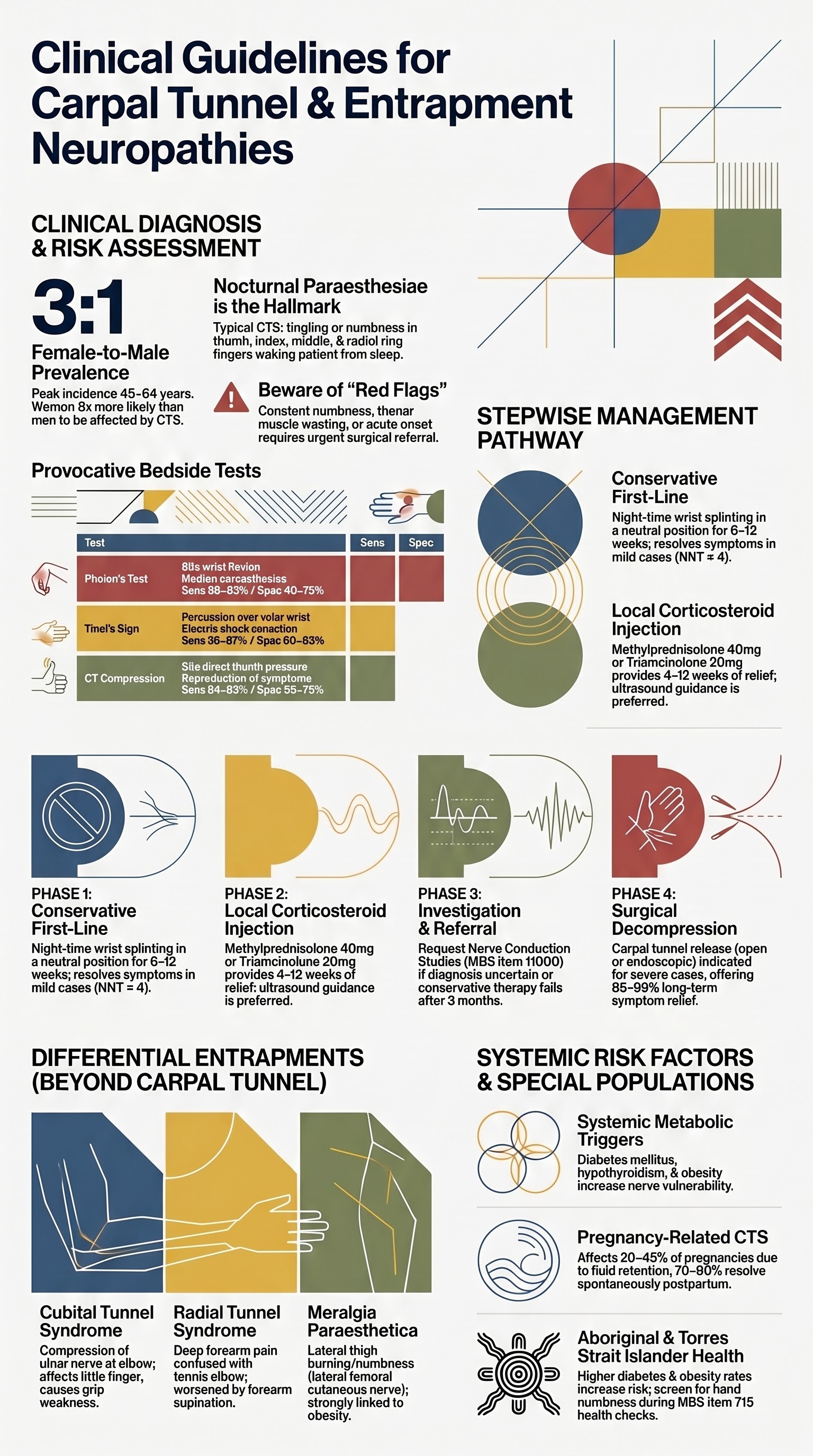
- Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy in Australia, affecting 3–6% of the adult population with higher prevalence in women and certain occupational groups.
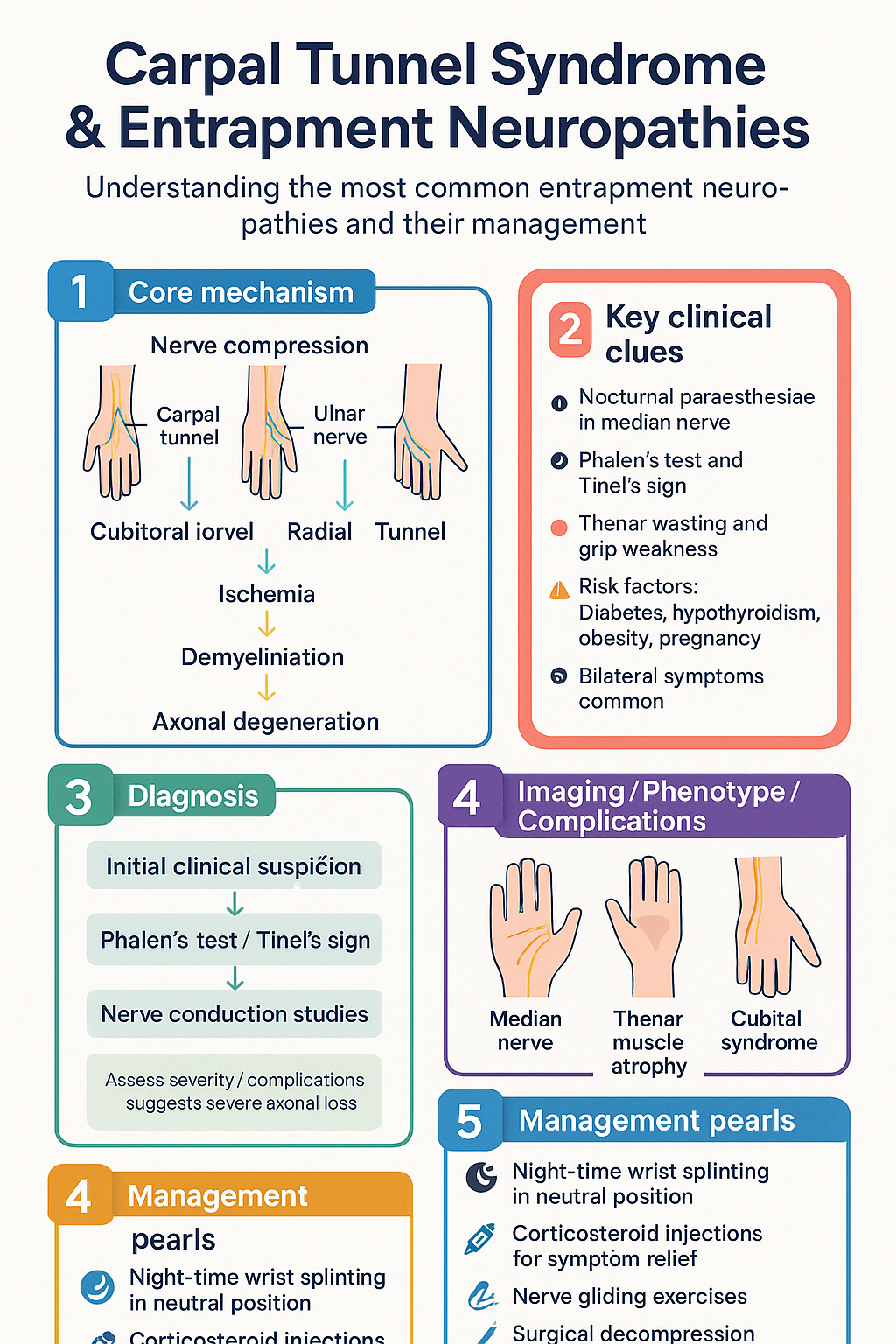
- Typical CTS presents with nocturnal paraesthesiae in the median nerve distribution (thumb, index, middle, lateral ring finger), often waking the patient from sleep.
- Phalen's test (wrist flexion 60 s) and Tinel's sign (percussion over carpal tunnel) are useful bedside provocative tests but have moderate sensitivity and specificity — clinical diagnosis remains paramount.
- First-line management is night-time wrist splinting in neutral position for ≥6 weeks; this alone resolves symptoms in many mild-to-moderate cases.
- Corticosteroid injection (methylprednisolone 40 mg or triamcinolone 20 mg locally) provides short-to-medium-term relief and is PBS-listed; can be repeated once if initial response is good but relapses.
- Nerve conduction studies (NCS) are indicated when the diagnosis is uncertain, symptoms are severe or persistent despite conservative therapy, or surgical decompression is being considered (Medicare rebate Item 11000 series).
- Carpal tunnel release (open or endoscopic) is indicated for severe or refractory CTS with thenar wasting, constant numbness, or failed ≥3 months of conservative management.
- Cubital tunnel syndrome (ulnar nerve at elbow) presents with medial forearm/hand numbness and grip weakness; conservative measures include avoiding elbow flexion and padding; surgery indicated for motor deficit or refractory cases.
- Meralgia paraesthetica (lateral femoral cutaneous nerve) causes lateral thigh burning/numbness; usually managed conservatively with weight reduction, looser clothing, and gabapentinoids; surgery rarely required.
- Radial tunnel syndrome causes deep proximal forearm pain worsened by forearm supination against resistance; distinguish from lateral epicondylitis; usually responds to physiotherapy and activity modification.
- Diabetes mellitus, hypothyroidism, obesity, pregnancy, and rheumatoid arthritis are important systemic risk factors for entrapment neuropathies — screen accordingly.
- Aboriginal and Torres Strait Islander peoples may have higher rates of undiagnosed diabetes and obesity, increasing entrapment neuropathy risk; culturally appropriate screening and access to specialist services in remote areas remain critical gaps.
Introduction & Australian Epidemiology
Entrapment neuropathies result from focal compression or tension on a peripheral nerve at an anatomical bottleneck, leading to ischaemia, demyelination, and — if prolonged — axonal degeneration. Carpal tunnel syndrome (CTS) is by far the most common, but cubital tunnel syndrome, radial tunnel syndrome, and meralgia paraesthetica are also frequently encountered in Australian primary care and specialist practice.
In Australia, CTS has an estimated prevalence of 3–6% in the general adult population and accounts for the majority of upper-limb nerve conduction studies performed. The Australian Institute of Health and Welfare (AIHW) data indicate that carpal tunnel release is among the most commonly performed hand and wrist procedures in both public and private hospitals, with over 20,000 procedures nationally per year. Women are affected approximately three times more often than men, and peak incidence occurs between ages 45 and 64.
Occupational factors remain debated in the Australian literature. While repetitive manual work, vibration exposure, and sustained wrist flexion/extension are associated with CTS in Workers' Compensation claims (Safe Work Australia), population-based studies suggest that the attributable occupational risk is smaller than previously believed, with systemic metabolic factors (diabetes, obesity, thyroid disease, pregnancy) playing an equally important role.
Carpal Tunnel Syndrome
Typical Symptoms
CTS classically presents with intermittent or constant paraesthesiae (tingling, burning, numbness) in the distribution of the median nerve distal to the carpal tunnel — affecting the thumb, index finger, middle finger, and the radial half of the ring finger. The little finger is characteristically spared.
- Nocturnal symptoms are the hallmark — patients report waking with a "dead" or tingling hand, often relieved by shaking or hanging the hand over the side of the bed.
- Activity-related symptoms — gripping, driving, holding a phone, or repetitive wrist flexion may provoke paraesthesiae.
- Weakness and clumsiness — dropping objects, difficulty with jars and buttons suggests thenar muscle involvement (abductor pollicis brevis) and indicates more advanced disease.
- Pain may radiate proximally into the forearm, wrist, or even the shoulder, but isolated proximal arm pain without digital paraesthesiae is atypical for CTS.
- Constant numbness in the median nerve territory with two-point discrimination >6 mm at the index finger pulp suggests severe axonal loss and warrants urgent surgical consideration.
Provocative Clinical Tests
| Test | Technique | Positive Result | Sensitivity / Specificity |
|---|---|---|---|
| Phalen's test | Patient holds wrists in full flexion (palms together) for 60 seconds | Reproduction of median nerve paraesthesiae within 60 s | Sens 68–83% / Spec 40–73% |
| Reverse Phalen (prayer sign) | Wrist extension (dorsiflexed prayer position) for 60 s | Paraesthesiae in median distribution | Sens 48–67% / Spec 56–75% |
| Tinel's sign | Percussion over the carpal tunnel (volar wrist crease) | Electric shock or tingling into median nerve fingers | Sens 38–67% / Spec 60–83% |
| Carpal tunnel compression test | Direct sustained pressure over carpal tunnel with thumbs for 30 s | Reproduction of symptoms | Sens 64–87% / Spec 50–73% |
| Thenar wasting | Visual inspection and palpation of the thenar eminence | Visible or palpable atrophy of abductor pollicis brevis | Low sensitivity but highly specific for severe CTS |
Initial Conservative Management — Wrist Splinting
Night-time wrist splinting in neutral position (0° extension) is the recommended first-line therapy for mild-to-moderate CTS. A rigid or semi-rigid splint that maintains the wrist in neutral prevents flexion during sleep, reducing intraneural pressure.
- Duration: Minimum 6 weeks; often 8–12 weeks to assess full benefit.
- Wear schedule: Nightly; some patients benefit from daytime wear during aggravating activities.
- Availability: Prefabricated wrist splints (e.g., Futuro®, Mueller®) are available over the counter at pharmacies for approximately $20–40; custom thermoplastic splints from a hand therapist (Item 10950 MBS) may be preferred for complex cases.
- Evidence: A Cochrane review (2012) and subsequent RCTs show that splinting significantly improves symptoms at 6 weeks compared to no treatment, with NNT ≈ 4.
- Adjuncts: Nerve gliding exercises (median nerve neurodynamic mobilisation) may provide additional benefit when supervised by a physiotherapist or hand therapist.
Corticosteroid Injection
Local corticosteroid injection into the carpal tunnel is recommended when splinting alone provides insufficient relief after 4–6 weeks, or when rapid symptom control is needed while awaiting specialist review or surgery.
When to Request Nerve Conduction Studies
Nerve conduction studies (NCS) and electromyography (EMG) are not required to diagnose classic CTS with a clear clinical history. However, NCS/EMG are indicated in the following circumstances:
- Diagnostic uncertainty — atypical symptoms, symptoms in non-median distribution, or suspected alternative diagnoses (cervical radiculopathy, polyneuropathy, brachial plexopathy).
- Severe or progressive symptoms — constant numbness, thenar wasting, or weakness to help grade severity and guide urgency of surgical referral.
- Failed conservative management — prior to surgical decompression to confirm the diagnosis and exclude co-existing proximal pathology.
- Medicolegal or Workers' Compensation cases where objective documentation is required.
- Recurrent symptoms after surgery — to assess for incomplete release, fibrosis, or misdiagnosis.
Australian access and MBS: NCS/EMG is available in most metropolitan centres and many regional hospitals. The MBS Item 11000 series provides a Medicare rebate for nerve conduction studies when requested by a specialist (neurologist, rehabilitation physician, or surgeon). Some GPs can access NCS through community neurophysiology services, though specialist interpretation is recommended. Wait times in the public system can be 4–12 weeks; private access is typically within 1–2 weeks.
Other Entrapment Neuropathies
Cubital Tunnel Syndrome (Ulnar Nerve at the Elbow)
Cubital tunnel syndrome is the second most common upper-limb entrapment neuropathy. The ulnar nerve is compressed at the elbow, most commonly at the cubital tunnel (behind the medial epicondyle) or the Osborne's ligament (arcuate ligament).
Symptoms and Signs
- Paraesthesiae and numbness in the ulnar 1½ fingers (ring and little finger) and ulnar border of the hand.
- Medial elbow pain, often worse with sustained elbow flexion (e.g., holding a phone, sleeping with arms bent).
- Grip weakness and clumsiness — difficulty opening jars, turning keys.
- Severe/signs of denervation: Intrinsic hand muscle wasting (first dorsal interosseous, hypothenar muscles), clawing of ring and little fingers (ulnar claw hand), Wartenberg's sign (abducted little finger), Froment's sign (IP flexion of thumb on pinch grip).
Bedside Tests
- Tinel's at the elbow — percussion over the ulnar nerve in the cubital tunnel.
- Elbow flexion test — full elbow flexion with wrist extension for 60 s; reproduction of ulnar symptoms.
- Froment's sign — compensatory thumb IP flexion when pinching paper, indicating adductor pollicis weakness.
Conservative vs Surgical Management
Radial Tunnel Syndrome
Radial tunnel syndrome involves compression of the posterior interosseous nerve (deep branch of the radial nerve) as it passes through the radial tunnel — from the radiocapitellar joint through the supinator muscle (Arcade of Frohse). It is often misdiagnosed as lateral epicondylitis.
Key Distinguishing Features from Lateral Epicondylitis
| Feature | Radial Tunnel Syndrome | Lateral Epicondylitis |
|---|---|---|
| Pain location | Deep, aching pain 3–5 cm distal to lateral epicondyle (over the radial tunnel) | Lateral epicondyle itself |
| Aggravating factor | Forearm supination against resistance; resisted middle finger extension | Wrist extension against resistance |
| Tenderness | Tenderness over the radial tunnel (distal to epicondyle) | Tenderness at the lateral epicondyle |
| Paraesthesiae | Usually absent (pure motor/sensory deep branch) | Absent |
| Weakness | Late — finger drop if posterior interosseous nerve palsy develops | Weakness secondary to pain |
Management
- Conservative (first-line): Activity modification (avoid repetitive supination/pronation), physiotherapy focusing on forearm extensor stretching and strengthening, counterforce bracing, NSAIDs for 2–4 weeks.
- Corticosteroid injection: May be trialled at the radial tunnel (deep to the extensor carpi radialis brevis); evidence is limited and effect size is small.
- Referral for surgery: Indicated for refractory cases failing 3–6 months of conservative therapy, or if posterior interosseous nerve palsy develops (finger/wrist drop). Surgical decompression of the radial tunnel has variable outcomes (60–80% improvement).
Meralgia Paraesthetica (Lateral Femoral Cutaneous Nerve)
Meralgia paraesthetica results from compression of the lateral femoral cutaneous nerve (LFCN) as it passes beneath or through the inguinal ligament, typically near the anterior superior iliac spine (ASIS). It is a purely sensory nerve; motor involvement does not occur.
Symptoms
- Burning, tingling, or numbness over the anterolateral thigh — from the ASIS to the mid-thigh.
- Symptoms are worsened by standing, walking, or hip extension and relieved by sitting or hip flexion.
- Allodynia (pain from light touch to the affected area) may be present in chronic cases.
Risk Factors
- Obesity (BMI >30) — the single strongest modifiable risk factor.
- Tight clothing — belts, corsets, tight waistbands, tool belts.
- Pregnancy — increased abdominal girth and intra-abdominal pressure.
- Diabetes mellitus — predisposes to nerve vulnerability.
- Post-surgical — iliac bone graft harvest, hip replacement (direct nerve injury).
Conservative vs Referral
Pathophysiology
Entrapment neuropathies share a common pathophysiological mechanism: focal nerve compression at an anatomical site where the nerve passes through a rigid or semi-rigid tunnel or beneath a fibrous band.
- Mechanical compression reduces intraneural blood flow, causing endoneurial oedema and ischaemia. Venous congestion occurs first, followed by arterial insufficiency if compression persists.
- Demyelination at the compression site produces conduction block and/or slowing, detectable on NCS as prolongation of distal motor latency or reduction in sensory nerve action potential amplitude.
- In chronic compression, segmental demyelination progresses to secondary axonal degeneration, which is associated with muscle denervation (visible on EMG as fibrillation potentials and positive sharp waves) and poorer prognosis for full recovery after decompression.
- In CTS specifically: The carpal tunnel is an osseofibrous space bounded by the carpal bones dorsally and the flexor retinaculum (transverse carpal ligament) volarly. Increased pressure within the tunnel (from synovial hypertrophy, oedema, space-occupying lesions, or anatomical variation) compresses the median nerve. Normal carpal tunnel pressure is 2–10 mmHg; in CTS, it may exceed 30 mmHg at rest and rise further with wrist flexion.
- Systemic predisposing conditions: Diabetes mellitus causes endoneurial microangiopathy making nerves more vulnerable to compression. Hypothyroidism causes mucopolysaccharide deposition in the flexor tenosynovium. Rheumatoid arthritis causes synovial hypertrophy. Obesity increases carpal tunnel pressure.
Investigations
Nerve Conduction Studies and Electromyography (NCS/EMG)
Laboratory Investigations (Screening for Systemic Causes)
Imaging
Risk Stratification & Severity Scoring
For carpal tunnel syndrome, clinical severity can be graded to guide management urgency and predict response to conservative versus surgical treatment. The Bland classification (modified) is widely used in Australian practice:
Empirical Therapy
Stepwise Approach to Carpal Tunnel Syndrome
Pharmacological Options for Neuropathic Pain Component
While entrapment neuropathies are primarily mechanical problems, neuropathic pain agents may provide symptomatic relief while definitive treatment is arranged:
Directed / Definitive Therapy
Carpal Tunnel Release Surgery
Surgical decompression (carpal tunnel release) is indicated for:
- Severe CTS with constant numbness or thenar wasting.
- Moderate CTS failing ≥3 months of conservative management (splinting + at least one corticosteroid injection).
- Electrodiagnostically confirmed CTS with significant conduction impairment.
- CTS caused by a space-occupying lesion (ganglion cyst, lipoma, tenosynovitis) amenable to excision.
| Technique | Open Release | Endoscopic Release |
|---|---|---|
| Incision | 3–4 cm palmar incision | 1–2 small portal incisions |
| Average return to work | 3–4 weeks | 1–2 weeks |
| Long-term outcomes | Excellent (85–95% symptom relief) | Comparable |
| Risks | Palmar scar tenderness, pillar pain, nerve injury (rare) | Incomplete release, nerve/vessel injury (slightly higher risk with inexperienced operator) |
| Anaesthesia | Local ± sedation (day procedure) | Local ± sedation (day procedure) |
| Cost (private) | ~$1,500–3,000 (surgeon + anaesthetic) | Similar or slightly higher |
Post-Operative Rehabilitation
- Hand elevation and gentle finger movements from day 1.
- Wound care — keep dry for 5–7 days; sutures removed at 10–14 days.
- Light desk work: 1–2 weeks (endoscopic) or 2–3 weeks (open).
- Heavy manual work: 4–6 weeks (open) or 3–4 weeks (endoscopic).
- Hand therapy referral if stiffness, weakness, or complex regional pain syndrome (CRPS) develops.
Cubital Tunnel — Surgical Options
For cubital tunnel syndrome requiring surgery:
- In situ decompression — release of the cubital tunnel retinaculum (Osborne's ligament). Simplest technique; suitable for mild-to-moderate cases without nerve subluxation.
- Anterior transposition — the ulnar nerve is moved anterior to the medial epicondyle (subcutaneous, intramuscular, or submuscular). Indicated when nerve subluxates or in revision surgery.
- Medial epicondylectomy — removes the bony prominence compressing the nerve. Less commonly performed in modern practice.
Monitoring
Conservative Management Monitoring
Post-Surgical Monitoring
- 2 weeks: Wound check, suture removal, assess for early complications (infection, haematoma, nerve injury).
- 6 weeks: Assess symptom resolution, grip strength, wound healing. Most patients report significant improvement by this stage.
- 3 months: Formal review — assess for residual symptoms, pillar pain, scar tenderness. If no improvement, consider NCS and evaluate for incomplete release, incorrect diagnosis, or superimposed neuropathy.
- Long-term: Recurrence rate after carpal tunnel release is 3–10%. Patients should be counselled that symptoms may recur, particularly if systemic risk factors are not addressed.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of conditions that predispose to entrapment neuropathies, yet face significant barriers to timely diagnosis and treatment. Culturally safe, person-centred care is essential.
📚 References
- 1. Padua L, Coraci D, Erra C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(12):1273–1284.
- 2. Bland JD. Carpal tunnel syndrome. BMJ. 2007;335(7615):343–346.
- 3. Huisstede BM, Hoogvliet P, Randsdorp MS, et al. Carpal tunnel syndrome. Part I: effectiveness of nonsurgical treatments — a systematic review. Arch Phys Med Rehabil. 2010;91(7):981–1004.
- 4. Shi Q, MacDermid JC. Is surgical intervention more effective than non-surgical treatment for carpal tunnel syndrome? A systematic review. J Orthop Surg Res. 2011;6:17.
- 5. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 6. Royal Australian College of General Practitioners (RACGP). Management of type 2 diabetes: A handbook for general practice. Melbourne: RACGP; 2020.
- 7. Descatha A, Leclerc A, Chastang JF, Roquelaure Y; Study Group on Repetitive Work. Incidence of ulnar nerve entrapment at the elbow in repetitive work. Scand J Work Environ Health. 2004;30(3):234–240.
- 8. Safe Work Australia. Work-related musculoskeletal disorders in Australia. Canberra: Safe Work Australia; 2019.
- 9. Elnady B, Ekber M, Getha K, et al. Ultrasound for diagnosis of carpal tunnel syndrome: a systematic review and meta-analysis. J Ultrasound Med. 2023;42(5):1021–1034.
- 10. Necking LE, Dahlin LB, Fridén J. Clinical assessment of nerve compression: provocative tests and their diagnostic value. J Hand Surg Eur. 2020;45(8):803–810.
- 11. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. Canberra: NHMRC; 2018 (updated 2023).
- 12. Burke FD, Wilgis EFS, Dubin NH, et al. Relationship between the duration and type of symptoms and severity of carpal tunnel syndrome. J Hand Surg Eur. 2009;34(5):637–640.
- 13. Cheung C, Podemos S, Shah M. Meralgia paraesthetica: an update on diagnosis and management. Aust J Gen Pract. 2021;50(10):718–723.
- 14. RHDAustralia (Remote Health Division, NT Department of Health). Minimising the risk of rheumatic heart disease in Aboriginal and Torres Strait Islander peoples. Darwin: RHDAustralia; 2022.
- 15. Fajardo M, Kim SH, Szabo RM. Incidence of carpal tunnel release: trends and implications within the United States ambulatory care setting. J Hand Surg Am. 2012;37(8):1599–1605.