📋 Key Information Summary
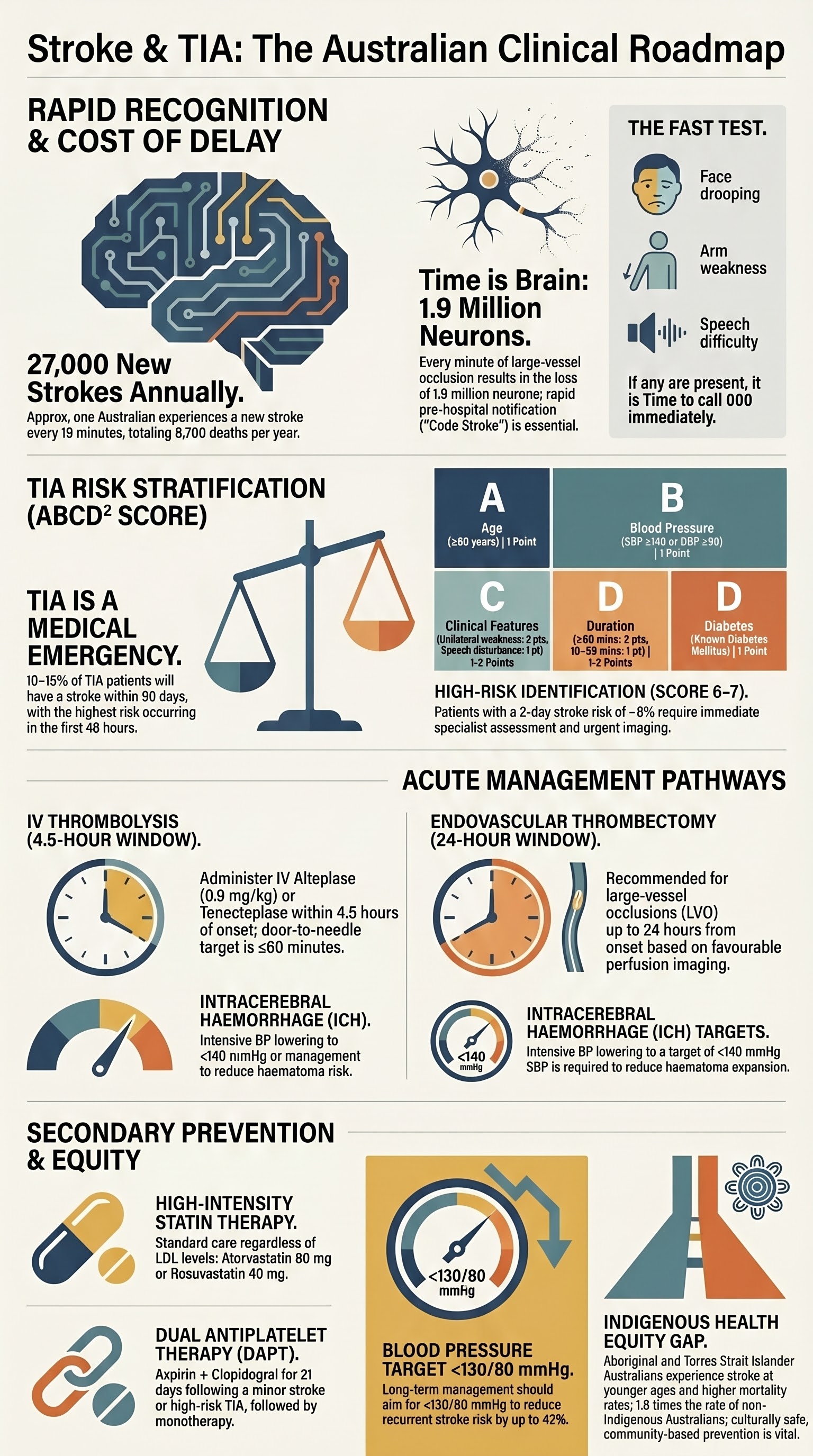
- Stroke is the third leading cause of death in Australia and the leading cause of adult disability; approximately 27,000 Australians experience a new stroke each year (AIHW 2023).
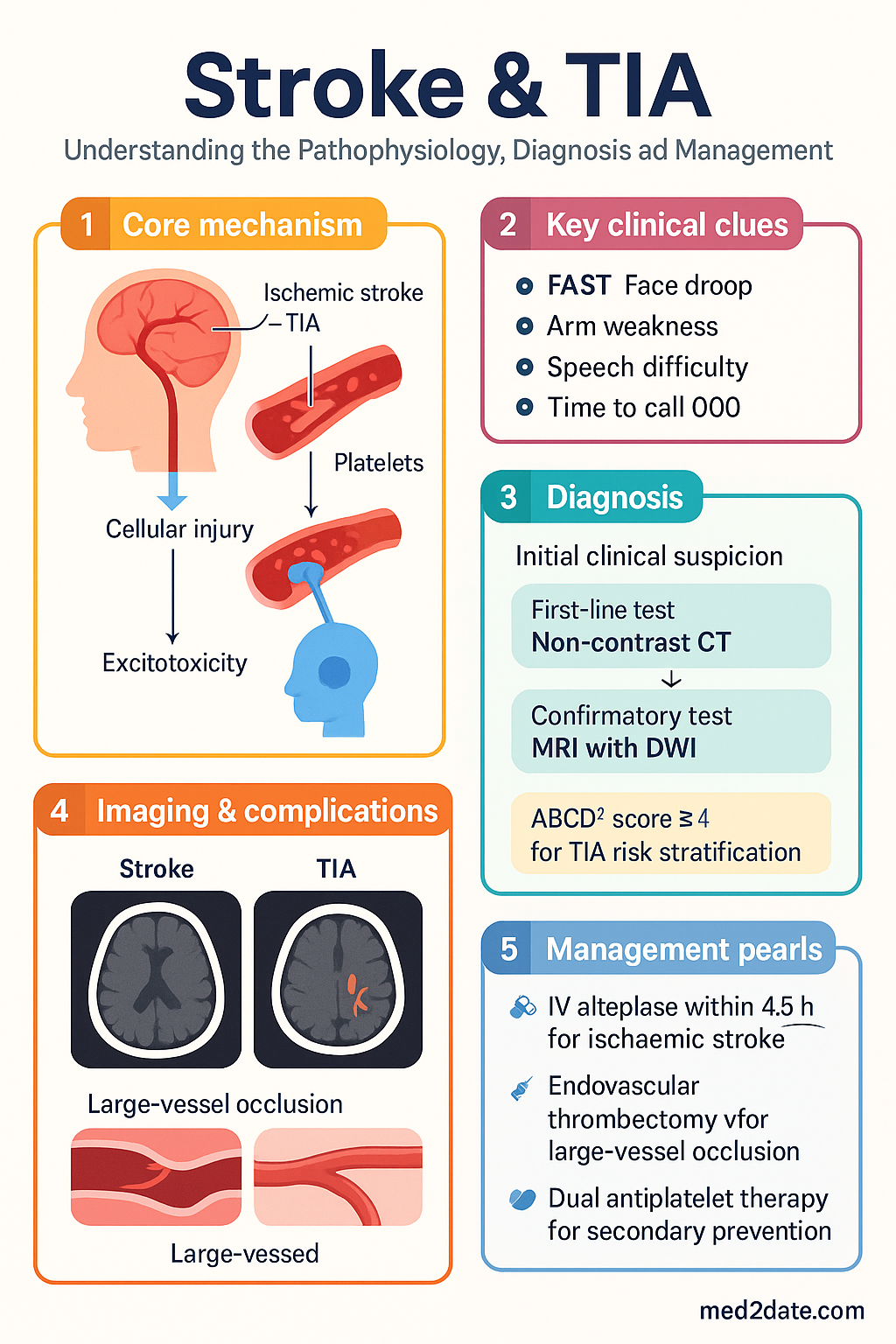
- Transient ischaemic attack (TIA) carries a 10–15% risk of stroke within 90 days, with the highest risk in the first 48 hours — urgent evaluation is mandatory.
- Use the ABCD² score for TIA risk stratification: score ≥4 warrants same-day specialist assessment and brain imaging (CT or MRI with DWI).
- Acute ischaemic stroke recognition uses FAST (Face, Arms, Speech, Time); call 000 immediately — "Time is brain."
- IV alteplase (tenecteplase) is indicated within 4.5 hours of ischaemic stroke onset in eligible patients; door-to-needle target ≤60 minutes.
- Endovascular thrombectomy is recommended for large-vessel occlusion (LVO) within 24 hours with favourable perfusion imaging; transfer to a comprehensive stroke centre without delay.
- Acute blood pressure targets: ischaemic stroke (post-thrombolysis <180/105 mmHg; non-thrombolysed permissive hypertension to 220/120 mmHg); ICH target <140 mmHg systolic (INTERACT2).
- Secondary prevention includes dual antiplatelet therapy (aspirin + clopidogrel) for 21 days after minor stroke/high-risk TIA, then single antiplatelet; anticoagulation for atrial fibrillation-related stroke.
- High-intensity statin therapy (atorvastatin 80 mg or rosuvastatin 40 mg) is standard for secondary stroke prevention regardless of baseline LDL.
- Intracerebral haemorrhage requires immediate reversal of anticoagulation (vitamin K + 4-factor PCC for warfarin; andexanet alfa for DOACs where available) and urgent neurosurgical referral if posterior fossa haemorrhage or hydrocephalus.
- Aboriginal and Torres Strait Islander Australians experience stroke 1.6 times more frequently than non-Indigenous Australians, with younger age of onset and higher mortality — culturally safe, community-based prevention is essential.
- All stroke patients should be assessed for rehabilitation needs, and managed in a dedicated stroke unit where available (evidence for reduced mortality and disability at 12 months).
Introduction & Australian Epidemiology
Stroke encompasses a spectrum of acute cerebrovascular events including ischaemic stroke (~85%), intracerebral haemorrhage (ICH, ~13%), and subarachnoid haemorrhage (~2%). Transient ischaemic attack (TIA) is defined as a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischaemia without acute infarction on imaging. The distinction between TIA and minor ischaemic stroke is increasingly made on MRI diffusion-weighted imaging (DWI) rather than symptom duration alone.
In Australia, stroke remains a leading cause of death and disability. According to the Australian Institute of Health and Welfare (AIHW, 2023):
- Approximately 27,000 new strokes occur each year (one every 19 minutes).
- Over 475,000 Australians are living with the effects of stroke.
- Stroke is the third leading cause of death (~8,700 deaths per year).
- The median age at first stroke is 73 years for men and 78 years for women, though approximately 25% of strokes occur in people under 65.
- Stroke costs the Australian health system an estimated $6.2 billion annually in direct and indirect costs.
- Aboriginal and Torres Strait Islander Australians experience stroke at 1.6 times the rate of non-Indigenous Australians and at a significantly younger age.
The National Stroke Foundation (now Stroke Foundation) has established the Australian Stroke Clinical Registry (AuSCR), and the National Safety and Quality Health Service (NSQHS) Stroke Clinical Care Standard (ACSQHC, 2019) sets benchmarks including time-critical targets for thrombolysis and access to stroke unit care.
TIA Evaluation
TIA is a medical emergency. Although neurological symptoms resolve completely, TIA signals a high short-term risk of completed stroke — up to 10–15% within 90 days, with half of these events occurring within 48 hours. Same-day or next-day TIA evaluation reduces subsequent stroke risk by up to 80% (EXPRESS study, Rothwell et al. 2007).
ABCD² Score for Risk Stratification
The ABCD² score is used in emergency departments and rapid-access TIA clinics to identify patients at highest risk of subsequent stroke.
| Feature | Criteria | Points |
|---|---|---|
| A — Age ≥60 years | Age 60 or older | 1 |
| B — Blood pressure | SBP ≥140 mmHg or DBP ≥90 mmHg at presentation | 1 |
| C — Clinical features | Unilateral weakness | 2 |
| Speech disturbance without weakness | 1 | |
| D — Duration | ≥60 minutes | 2 |
| 10–59 minutes | 1 | |
| D — Diabetes | Known diabetes mellitus | 1 |
| Total | 0–7 | |
Urgent Imaging
Carotid Workup
For anterior circulation TIA (hemiparesis, dysphasia, monocular visual loss), urgent carotid imaging is essential to identify candidates for carotid endarterectomy (CEA) or carotid artery stenting (CAS):
- Symptomatic carotid stenosis ≥70%: CEA recommended within 2 weeks of symptom onset (benefit greatest within 48 hours). NNT ≈ 5 over 5 years to prevent ipsilateral stroke (NASCET/ECST).
- Symptomatic carotid stenosis 50–69%: Moderate benefit from CEA; individualise decision. Consider CEA particularly in men, recent symptoms, and non-disabling stroke.
- Symptomatic carotid stenosis <50%: Best medical therapy alone; surgery not indicated.
- If ≥50% stenosis, CEA should be performed by a vascular surgeon with a perioperative complication rate <6% (Australian standard per RACS). CAS may be considered as an alternative in selected cases.
Cardiac Workup
- 12-lead ECG: Essential for all TIA/stroke patients to detect atrial fibrillation (AF) or other arrhythmias.
- Continuous cardiac monitoring: Inpatient telemetry for ≥24 hours for ischaemic stroke/TIA without known AF (detects paroxysmal AF in ~5–10%).
- Echocardiography (transthoracic ± transoesophageal): Indicated for patients with suspected cardiac source of embolism (e.g., valvular disease, intracardiac thrombus, PFO). MBS item 55122.
- Extended cardiac monitoring (Holter monitor 7–14 days or implantable loop recorder): Consider for cryptogenic TIA/stroke to detect paroxysmal AF. MBS item 11005.
Antiplatelet Initiation
Dual antiplatelet therapy (DAPT) for minor stroke/high-risk TIA: Based on the CHANCE and POINT trials, aspirin 300 mg loading + clopidogrel 300 mg loading, then aspirin 100 mg + clopidogrel 75 mg daily for 21 days is recommended for patients with minor ischaemic stroke (NIHSS ≤3) or high-risk TIA (ABCD² ≥4) presenting within 24 hours of symptom onset. After 21 days, transition to a single antiplatelet agent.
Acute Ischaemic Stroke Pathway
Recognition — FAST and Beyond
The FAST mnemonic is the primary public and prehospital stroke recognition tool endorsed by the Stroke Foundation Australia:
Thrombolysis — IV Alteplase/Tenecteplase
Intravenous thrombolysis is the cornerstone of acute ischaemic stroke treatment within the therapeutic window. Australian hospitals with stroke capabilities should target a door-to-needle time ≤60 minutes (NSQHS Stroke Clinical Care Standard).
| Parameter | Detail |
|---|---|
| Drug | Alteplase (Actilyse®) 0.9 mg/kg IV (max 90 mg); 10% as bolus over 1 min, remainder infused over 60 min. Tenecteplase (0.25 mg/kg IV, max 25 mg, single bolus) is increasingly used as an alternative, especially when thrombectomy is anticipated (AcT trial, NOR-TEST 2A). |
| Time window | Within 4.5 hours of symptom onset (or last known well time) |
| Inclusion criteria | Clinical diagnosis of ischaemic stroke causing measurable neurological deficit; CT brain showing no haemorrhage; age ≥18 years |
| Key exclusions | Intracranial haemorrhage on CT; BP persistently >185/110 mmHg despite treatment; platelet count <100 × 10⁹/L; INR >1.7 or PT >15 sec; current use of DOAC with last dose <48 hours (if renal function normal); recent major surgery/trauma (<14 days); known intracranial neoplasm, AVM, or aneurysm |
| Relative exclusions (3–4.5 h window) | Age >80 years, NIHSS >25, history of both diabetes and prior stroke — these are no longer absolute exclusions based on IST-3 and updated guidelines, but warrant careful specialist discussion |
| BP target post-thrombolysis | <180/105 mmHg for 24 hours post-alteplase |
Endovascular Thrombectomy (Mechanical Thrombectomy)
Endovascular thrombectomy (EVT) is the standard of care for acute ischaemic stroke caused by large-vessel occlusion (LVO) of the anterior circulation. Five landmark trials (MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME, REVASCAT) and subsequent meta-analyses demonstrated robust benefit, with NNT of 2.6 for reduced disability at 90 days.
| Eligibility Criterion | Detail |
|---|---|
| Imaging | CTA or MRA confirming large-vessel occlusion (ICA, M1, or M2 segment of MCA, basilar artery) |
| Time window — early (0–6 h) | Thrombectomy within 6 hours of symptom onset for anterior circulation LVO (no additional perfusion imaging required) |
| Time window — extended (6–24 h) | Based on DAWN/DEFUSE 3 criteria: favourable perfusion imaging (CTP or MRI perfusion) showing salvageable tissue (ischaemic core <70 mL, mismatch ratio ≥1.8) |
| ASPECTS score | ≥6 on non-contrast CT (higher is better; <6 suggests extensive established infarct with limited benefit) |
| Basilar artery occlusion | Thrombectomy indicated for basilar artery occlusion based on ATTENTION and BAOCHE trials (best evidence for NIHSS ≥10, within 12–24 hours with favourable imaging) |
| Comprehensive stroke centres in Australia | Available at Royal Melbourne, Royal Prince Alfred, Royal Adelaide, Sir Charles Gairdner, Princess Alexandra, Royal Brisbane and Women's Hospital, and others — Stroke Foundation maintains an updated list |
Blood Pressure Targets in Acute Ischaemic Stroke
| Scenario | BP Target | Preferred Agents |
|---|---|---|
| Pre-thrombolysis | <185/110 mmHg before alteplase administration | IV labetalol 10–20 mg over 1–2 min (may repeat); or IV GTN infusion 1–2 mg/hr; or IV nicardipine 5 mg/hr (if available) |
| Post-thrombolysis (first 24 h) | <180/105 mmHg | IV labetalol or GTN infusion; monitor BP every 15 min for 2 h, then every 30 min for 6 h, then hourly |
| Non-thrombolysed ischaemic stroke | Permissive hypertension up to 220/120 mmHg; treat only if BP >220/120 mmHg or end-organ damage | IV labetalol, GTN, or oral agents; avoid precipitous drops |
| After 72 hours | Commence/restart long-term antihypertensives; target <130/80 mmHg for secondary prevention | ACE inhibitor ± thiazide ± calcium channel blocker (per SPS3/PATS trials) |
Acute Stroke Unit Care
All acute stroke patients should be managed in a dedicated stroke unit where available. Stroke unit care (multidisciplinary team, protocol-driven management, early mobilisation, monitoring for complications) reduces mortality, institutionalisation, and dependency at 12 months (Cochrane review, 2013). The NSQHS Stroke Clinical Care Standard recommends that ≥80% of acute stroke patients receive stroke unit care.
- Monitoring: Neurological observations (GCS, NIHSS) every 1–4 hours for 72 hours; continuous cardiac telemetry for ≥24 hours; blood glucose monitoring (avoid hypo- and hyperglycaemia); oxygen saturation (maintain SpO₂ ≥94%; supplemental O₂ only if <94%)
- Swallowing assessment: Must be performed by a trained speech pathologist before any oral intake (nil by mouth until assessed). Aspiration pneumonia is a leading cause of post-stroke morbidity.
- DVT prophylaxis: Intermittent pneumatic compression devices; consider LMWH (enoxaparin 40 mg SC daily) after 24–48 hours if haemorrhagic transformation excluded.
- Glycaemic control: Target 5–15 mmol/L; treat glucose >10 mmol/L with insulin; avoid hypoglycaemia (<4 mmol/L).
- Temperature: Treat fever (>38°C) aggressively with paracetamol and source investigation; avoid therapeutic hypothermia (not recommended routinely).
Secondary Prevention
Secondary prevention should commence as soon as the acute phase is complete, ideally before discharge from hospital. Comprehensive risk factor modification reduces the risk of recurrent stroke by 70–80%. All patients require a structured plan addressing antiplatelet/anticoagulation, statins, blood pressure, diabetes, and lifestyle.
Antiplatelet vs Anticoagulation
The choice between antiplatelet and anticoagulant therapy depends on the underlying aetiology:
- First-line options (monotherapy): Aspirin 100–300 mg daily OR Clopidogrel 75 mg daily OR Aspirin 25 mg + dipyridamole 200 mg BD (Aggrenox®)
- Clopidogrel is marginally superior to aspirin alone (CAPRIE trial) and is preferred if aspirin-intolerant.
- Aspirin-dipyridamole combination is equivalent to clopidogrel (PRoFESS trial) but often poorly tolerated (headache).
- DAPT (21 days): For minor stroke/high-risk TIA (see TIA section above).
- Long-term DAPT (>21 days) is NOT recommended for secondary stroke prevention (increased bleeding, no benefit).
- Indicated for stroke associated with atrial fibrillation (valvular or non-valvular), mechanical heart valves, or intracardiac thrombus.
- Non-valvular AF: DOAC preferred over warfarin — apixaban (Eliquis®) 5 mg BD, rivaroxaban (Xarelto®) 20 mg daily, or dabigatran (Pradaxa®) 150 mg BD.
- Timing after ischaemic stroke: Mild stroke (NIHSS <8): restart/introduce DOAC at day 3. Moderate stroke (NIHSS 8–15): day 6–7. Severe stroke (NIHSS >15): day 12–14 (with repeat imaging to exclude haemorrhagic transformation).
- Mechanical heart valves: Warfarin only (INR 2.5–3.5); DOACs are contraindicated.
- DOAC dose reductions: Apixaban 2.5 mg BD if ≥2 of: age ≥80, weight ≤60 kg, Cr ≥133 µmol/L. Rivaroxaban 15 mg daily if eGFR 15–49.
Statins for Secondary Prevention
High-intensity statin therapy is recommended for ALL patients with ischaemic stroke or TIA of atherosclerotic origin, regardless of baseline LDL cholesterol (SPARCL trial: 16% relative risk reduction in recurrent stroke). Initiate within 48 hours of the event if possible. Statins are generally not indicated for primary ICH without coexisting atherosclerotic vascular disease.
Blood Pressure Management
Hypertension is the single most important modifiable risk factor for recurrent stroke. Treatment should commence or be optimised during the index admission.
- Target: <130/80 mmHg for most stroke/TIA patients (ACC/AHA 2017, ESH 2023). Some patients, especially the elderly, may tolerate a target of <140/90 mmHg initially.
- First-line agents: ACE inhibitor (perindopril 4–8 mg daily) ± indapamide 1.5 mg SR daily (PROGRESS trial: combination reduced recurrent stroke by 43%); OR ARB (telmisartan, candesartan); OR calcium channel blocker (amlodipine 5–10 mg daily).
- Timing: Restart pre-existing antihypertensives once clinically stable (usually 24–48 hours post-ischaemic stroke; 7 days post-ICH). New agents can be introduced before discharge.
- Renal artery stenosis: Consider in young patients or those with resistant hypertension; Australian availability of duplex US, CTA, or MRA.
Diabetes Management
- Diabetes increases stroke risk 2–4 fold and worsens post-stroke outcomes.
- HbA1c target: ≤53 mmol/mol (7.0%) for most patients; individualise for frail/elderly patients.
- SGLT2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 receptor agonists (semaglutide, liraglutide) have demonstrated cardiovascular benefit and are preferred in patients with established atherosclerotic cardiovascular disease including stroke.
- Screen for post-stroke glucose intolerance (HbA1c and fasting glucose) in all non-diabetic patients.
Lifestyle Modifications
- Smoking cessation: Single most effective lifestyle intervention. Offer NRT, varenicline (Champix® — PBS Authority Required), or buphenix. Refer to Quitline (13 7848). PBS status: varenicline Authority Required.
- Alcohol: Limit to ≤10 standard drinks per week (NHMRC guidelines 2020). Binge drinking is an independent stroke risk factor.
- Physical activity: ≥150 min/week moderate-intensity aerobic exercise; commence after medical clearance; supervised programs preferred.
- Diet: Mediterranean or DASH-style diet; reduce sodium to <2,000 mg/day; increase fruit, vegetables, whole grains, and oily fish.
- Weight management: Target BMI 18.5–25 kg/m²; waist circumference <94 cm (men) or <80 cm (women).
- Obstructive sleep apnoea: Prevalent in stroke patients (50–70%); screen with STOP-BANG questionnaire; refer for polysomnography and CPAP if indicated.
Patent Foramen Ovale (PFO) Closure
PFO closure should be considered in patients aged <60 years with cryptogenic ischaemic stroke and a high-risk PFO (large shunt, atrial septal aneurysm) after thorough investigation to exclude other aetiologies. The CLOSE, RESPECT, and DEFENSE-PFO trials demonstrated benefit in this subgroup. Refer to a cardiologist with structural heart intervention expertise.
Intracerebral Haemorrhage Basics
Spontaneous intracerebral haemorrhage (ICH) accounts for approximately 13% of all strokes in Australia and carries the highest mortality rate of any stroke subtype (30–50% at 30 days). Management focuses on haemostasis, blood pressure reduction, reversal of anticoagulation, and identification of surgical candidates.
Initial Assessment
- Airway: GCS ≤8 typically requires intubation and mechanical ventilation; involve ICU/anaesthetics early.
- Urgent non-contrast CT brain: Confirms haemorrhage, assesses volume (ABC/2 method), location (deep/infratentorial/lobar), intraventricular extension, and hydrocephalus.
- CT angiography: Consider in patients <70 years, lobar haemorrhage, or no history of hypertension — to identify underlying vascular malformation, aneurysm, or the "spot sign" (active contrast extravasation, indicating haematoma expansion risk).
- Bloods: FBC, coagulation (INR, APTT, fibrinogen), UEC, LFTs, BSL, group and hold, troponin.
- ICH Score: Glasgow Coma Scale, age, ICH volume, intraventricular haemorrhage, infratentorial origin — for prognostication (range 0–6; score ≥5 associated with 30-day mortality >95%).
Blood Pressure Control in ICH
| Scenario | BP Target | Agents |
|---|---|---|
| SBP 150–220 mmHg (no contraindication) | Target SBP <140 mmHg within 1 hour (INTERACT2/ATACH-2) | IV labetalol 10–20 mg bolus (repeat q10–20 min, max 300 mg); or IV nicardipine 5 mg/hr (titrate by 2.5 mg/hr q5–15 min, max 15 mg/hr); or IV GTN infusion 1–2 mg/hr. Transition to oral agents once stable. |
| SBP >220 mmHg | Aggressive reduction with IV infusion; close monitoring in ICU | IV nicardipine or labetalol infusion; continuous arterial BP monitoring preferred |
| On anticoagulants — avoid rapid excessive drops | SBP <140 mmHg; ensure concurrent coagulation reversal | As above, with coagulation reversal (see below) |
Reversal of Anticoagulation
Anticoagulation-associated ICH is a medical emergency. The risk of haematoma expansion is highest in the first few hours, and reversal should not be delayed for any reason.
Tranexamic Acid in ICH
The TICH-2 trial showed that tranexamic acid (1 g IV over 10 min, then 1 g over 8 hours) reduced haematoma expansion but did not improve functional outcomes or mortality at 90 days. It is not routinely recommended for ICH management in Australian guidelines but may be considered on a case-by-case basis, especially if presentation is very early (<3 hours).
Neurosurgical Referral Triggers
Most ICH is managed medically. Neurosurgical intervention is indicated in selected cases. Urgent neurosurgical consultation should be sought for:
- Posterior fossa (cerebellar) haemorrhage with brainstem compression, hydrocephalus, or haematoma diameter ≥3 cm — surgical evacuation is often life-saving (STICH I/II data support).
- Hydrocephalus from intraventricular haemorrhage — consider external ventricular drain (EVD) insertion.
- Lobar haemorrhage with progressive neurological deterioration and haematoma within 1 cm of the cortical surface — may benefit from surgical evacuation.
- Suspected underlying structural lesion (AVM, cavernoma, tumour) — angiography and neurosurgical assessment.
- Young patients with deep ICH and rapid deterioration — consider haematoma evacuation if clinical trajectory warrants.
Ongoing ICH Management
- Seizure management: Prophylactic antiepileptic drugs are not routinely recommended. Treat clinical seizures with levetiracetam (Keppra®) 500–1000 mg IV/PO BD or phenytoin 15–20 mg/kg loading. Continuous EEG monitoring if reduced consciousness out of proportion to imaging.
- Reversal of therapeutic anticoagulation effects: Hold warfarin for 10–14 days; hold DOACs for 4 weeks. Reintroduction of anticoagulation in patients with AF after ICH is a complex decision — consider LAA occlusion as an alternative. Discuss with stroke physician and haematologist.
- Haematoma expansion: Repeat CT at 24 hours or with any clinical deterioration. Growth of haematoma by >33% or >6 mL predicts poor outcome.
- VTE prophylaxis: Intermittent pneumatic compression from admission. Pharmacological prophylaxis (enoxaparin 40 mg SC daily) may be commenced after 48 hours if haemorrhage is stable on repeat imaging.
Special Populations
Pregnancy
- Stroke risk is elevated 2–3 times during pregnancy and the puerperium, particularly in the third trimester and first 6 weeks postpartum.
- Thrombolysis: Alteplase is pregnancy category B3 (TGA). It does not cross the placenta but carries a risk of maternal haemorrhage. Use only if ischaemic stroke is life-threatening and benefit clearly outweighs risk; discuss with obstetric medicine.
- Anticoagulation: Warfarin is teratogenic (Category D) in the first trimester. Use LMWH (enoxaparin weight-adjusted) for anticoagulation in pregnancy. DOACs are contraindicated.
- Antiplatelet: Low-dose aspirin (100–150 mg daily) is considered safe in pregnancy and is used for pre-eclampsia prevention. Clopidogrel has limited safety data — avoid if possible.
- Posterior reversible encephalopathy syndrome (PRES) and cerebral venous sinus thrombosis (CVST) must be considered in the differential diagnosis of pregnancy-related neurological presentations.
- Statins: Contraindicated in pregnancy (teratogenic). Discontinue before conception or immediately upon recognition of pregnancy.
Paediatrics
- Childhood stroke incidence is approximately 2–3 per 100,000 children per year in Australia. Aetiology differs substantially from adults: cardiac disease, moyamoya, arteriopathy, sickle cell disease, and prothrombotic states.
- Recognition: Use the FAST mnemonic adapted for children; also consider sudden onset seizures, severe headache, and altered consciousness.
- Thrombolysis: Not routinely recommended under 18 years due to limited evidence. Case-by-case decision at a comprehensive paediatric stroke centre. Alteplase dose: 0.9 mg/kg (max 90 mg) if used. Tenecteplase: limited paediatric data.
- Thrombectomy: Increasingly performed in older children with LVO at experienced centres; case-by-case basis.
- Anticoagulation/antiplatelet: Per Australian Paediatric Stroke Clinical Guidelines: anticoagulate (LMWH or unfractionated heparin) for arterial dissection, cardioembolism, or CVST. Aspirin 1–5 mg/kg/day for arterial ischaemic stroke without dissection.
- Sickle cell disease: Chronic transfusion programme for secondary prevention; transcranial Doppler screening for primary prevention (available at major paediatric centres).
Elderly (≥80 years)
- Patients ≥80 years account for ~33% of all strokes in Australia and have higher mortality and poorer functional outcomes.
- Thrombolysis: Age ≥80 is no longer an absolute exclusion for IV alteplase within 4.5 hours (IST-3 supported benefit). Tenecteplase may be preferred in this age group due to single bolus administration.
- Thrombectomy: Benefit extends to patients ≥80 years with LVO (HERMES collaboration). Functional outcomes are generally poorer; shared decision-making with family is essential.
- DOAC dose adjustment: Apixaban 2.5 mg BD if age ≥80 plus weight ≤60 kg or Cr ≥133 µmol/L. Rivaroxaban 15 mg daily if eGFR 15–49.
- Falls risk: Address polypharmacy; balance anticoagulation benefit against falls-related bleeding risk (falls alone rarely justify withholding anticoagulation — modelling shows net benefit of anticoagulation even in frequent fallers).
- Rehabilitation: Early mobilisation with physiotherapy, OT, and SALT; aim for inpatient rehabilitation where feasible. Assess for palliative care needs if severe stroke with poor prognosis.
Renal Impairment
- CKD (eGFR <60) is an independent risk factor for stroke and ICH. Dose adjustments are required for several stroke-related medications.
- DOACs: Dabigatran is predominantly renally cleared — avoid if eGFR <30 mL/min. Apixaban 2.5 mg BD if Cr ≥133 µmol/L with age ≥80 or weight ≤60 kg. Rivaroxaban 15 mg daily if eGFR 15–49.
- Contrast imaging: Use non-contrast CT as first-line; CTA requires careful risk-benefit assessment in severe CKD. Ensure adequate hydration; avoid metformin for 48 hours post-contrast if eGFR <30.
- LMWH: Reduce enoxaparin dose to 20 mg SC daily if eGFR <30 mL/min; monitor anti-Xa levels.
- Rosuvastatin: Start at 5 mg if eGFR <30; max 10 mg.
Hepatic Impairment
- Liver disease increases both thrombotic and bleeding risk (rebalanced haemostasis). ICH risk is elevated with coagulopathy and thrombocytopenia.
- DOACs: Contraindicated in Child-Pugh C (severe hepatic impairment); use with caution in Child-Pugh B. Rivaroxaban is contraindicated in Child-Pugh B/C (hepatotoxicity risk).
- Stains: Contraindicated in active liver disease. Atorvastatin and rosuvastatin can be used cautiously in Child-Pugh A–B with LFT monitoring.
- Warfarin: Unpredictable INR response; requires close monitoring if used. Prefer LMWH in severe liver disease with monitoring.
- Coagulopathy management: Correct INR >1.5 with PCC and vitamin K; correct platelets to >100 × 10⁹/L for any invasive procedure.
Immunocompromised
- HIV infection, transplant recipients, and patients on immunosuppressive therapy have increased stroke risk through accelerated atherosclerosis, vasculitis, opportunistic infections, and prothrombotic states.
- HIV: Screen for traditional vascular risk factors; consider vasculitis, CMV vasculopathy, and cryptococcal meningitis in the differential. CD4 count and viral load influence infection-related stroke risk.
- Drug interactions: DOACs interact with protease inhibitors (HIV) and calcineurin inhibitors (transplant) via CYP3A4/P-gp. Warfarin interacts with azoles, rifampicin, and antiretrovirals. Seek specialist pharmacy advice.
- Autoimmune vasculitis: Consider ANCA-associated vasculitis, SLE, and Behçet's disease in young patients with stroke. Refer to rheumatology for immunosuppressive management.
- Cerebral toxoplasmosis, PML, and CNS lymphoma may mimic stroke in severely immunosuppressed patients — MRI with contrast is essential.
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience significantly higher rates of stroke than non-Indigenous Australians. According to the AIHW (2023) and Stroke Foundation data:
- First Nations Australians experience stroke at 1.6 times the rate of non-Indigenous Australians.
- Stroke occurs at a younger age (median age ~56 years vs ~73 years in non-Indigenous Australians).
- 30-day stroke mortality is significantly higher for Indigenous Australians, particularly in remote areas.
- The burden of stroke in ATSI communities is driven by higher prevalence of modifiable risk factors: hypertension, diabetes (3–4 times more prevalent), smoking, obesity, rheumatic heart disease, and chronic kidney disease.
📚 References
- 1. Stroke Foundation Australia. Clinical Guidelines for Stroke Management 2022. Melbourne: Stroke Foundation; 2022. Available from: strokefoundation.org.au.
- 2. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards — Stroke Clinical Care Standard. Sydney: ACSQHC; 2019.
- 3. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines. Stroke. 2019;50(12):e344–e418.
- 4. Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study). Lancet. 2007;370(9596):1432–1442.
- 5. Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack (CHANCE). N Engl J Med. 2013;369(1):11–19.
- 6. Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA (POINT). N Engl J Med. 2018;379(3):215–225.
- 7. Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke (ESCAPE). N Engl J Med. 2015;372(11):1019–1030.
- 8. Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct (DAWN). N Engl J Med. 2018;378(1):11–21.
- 9. Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage (INTERACT2). N Engl J Med. 2013;368(25):2355–2365.
- 10. Amarenco P, Bogousslavsky J, Callahan A 3rd, et al. High-dose atorvastatin after stroke or transient ischemic attack (SPARCL). N Engl J Med. 2006;355(6):549–559.
- 11. PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358(9287):1033–1041.
- 12. Australian Institute of Health and Welfare (AIHW). Stroke and its management in Australia: an update. Cat. no. CVD 86. Canberra: AIHW; 2023.
- 13. National Heart Foundation of Australia / Cardiac Society of Australia and New Zealand. Guidelines for the management of atrial fibrillation 2018. Heart Lung Circ. 2018;27(10):1209–1266.
- 14. Stroke Foundation. Facts and Figures about Stroke in Australia. Melbourne: Stroke Foundation; 2023. Available from: strokefoundation.org.au.
- 15. Qureshi AI, Palesch YY, Barsan WG, et al. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage (ATACH-2). N Engl J Med. 2016;375(11):1033–1043.
- 16. RHDAustralia (Rheumatic Heart Disease Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.