📋 Key Information Summary
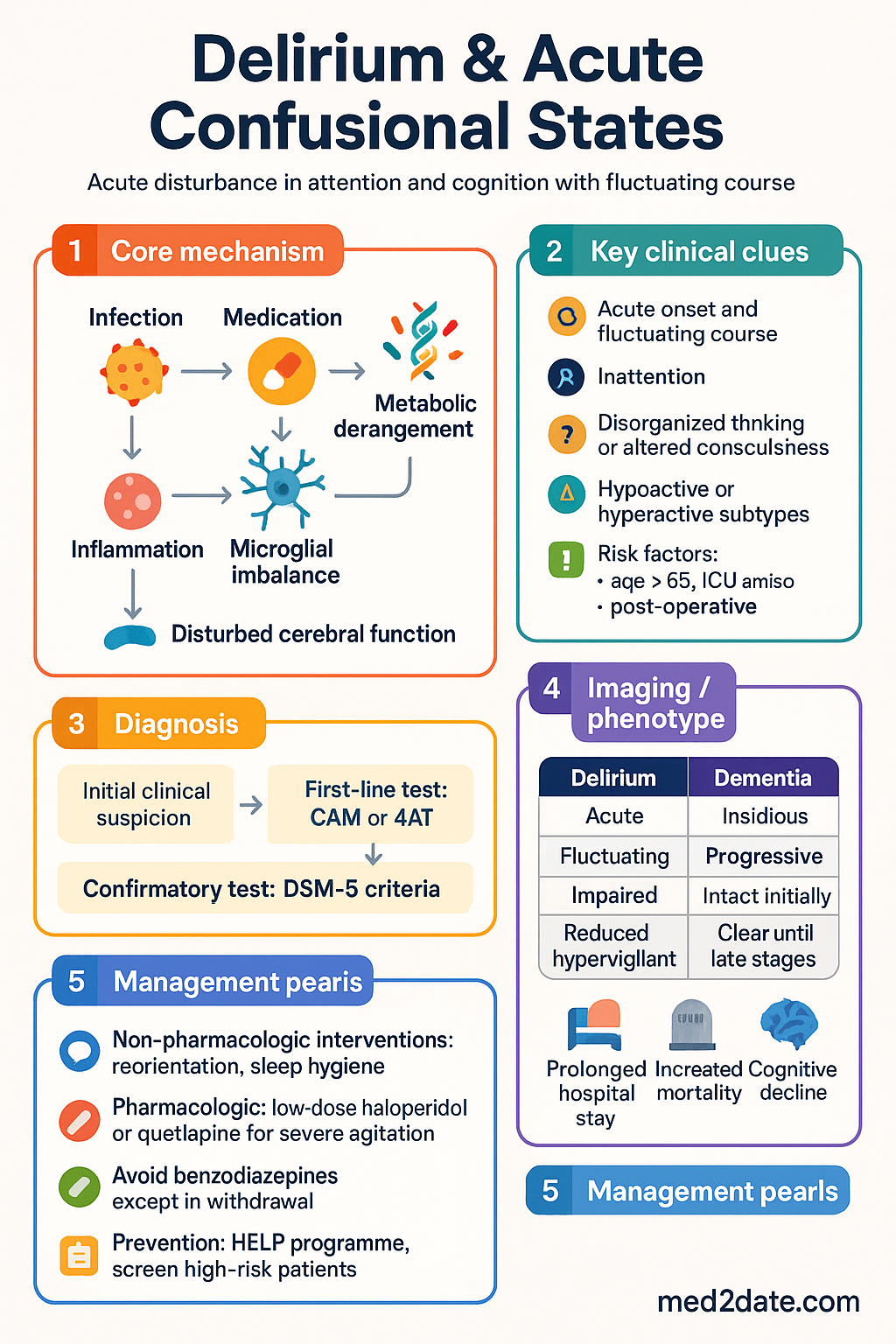
- Delirium is an acute, fluctuating disturbance in attention and awareness affecting 10–30% of Australian hospitalised adults, with rates exceeding 50% in ICU and post-operative orthopaedic populations.
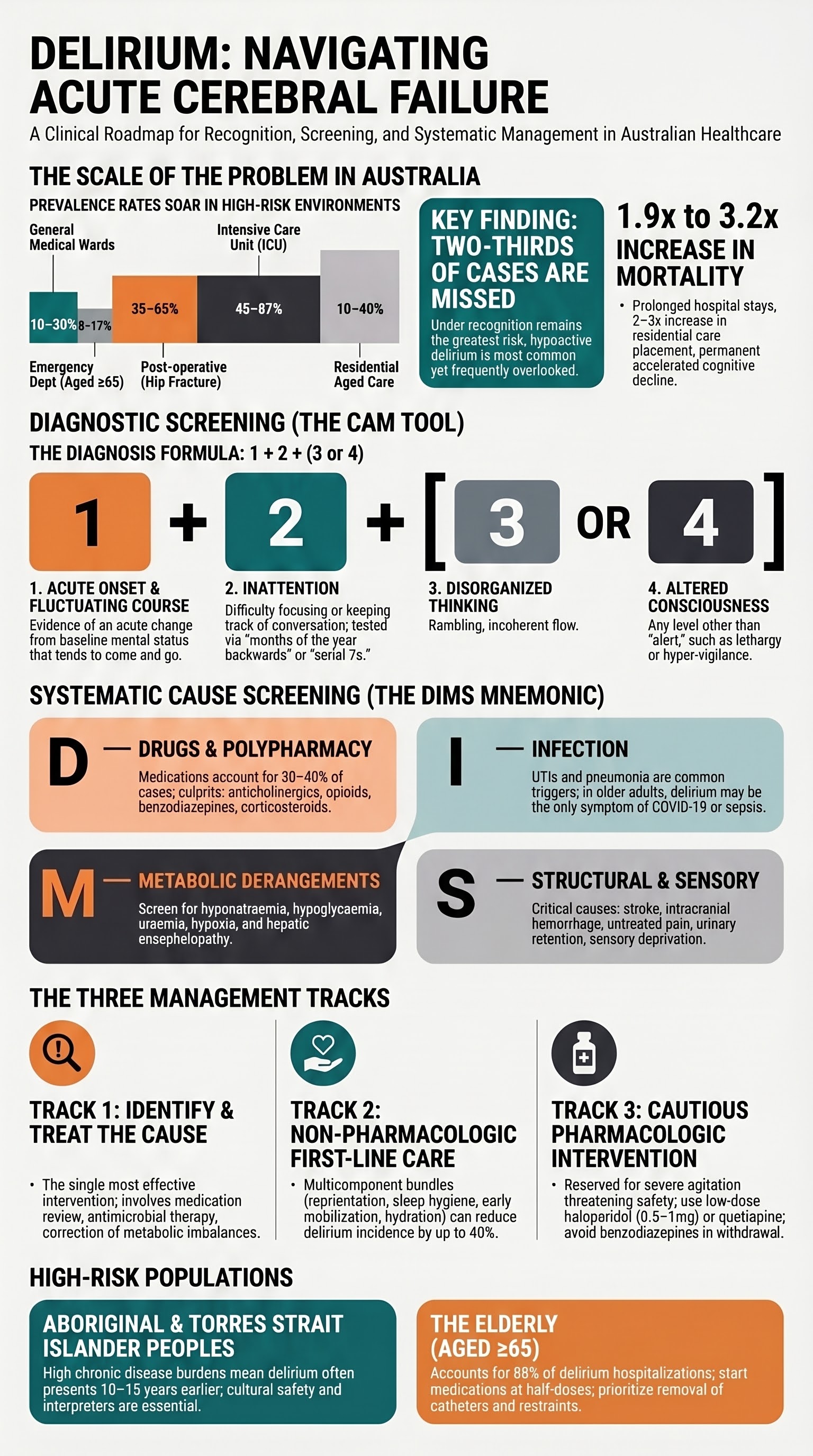
- The Confusion Assessment Method (CAM) is the recommended bedside screening tool in primary care and emergency departments — requires acute onset, fluctuating course, inattention, and disorganised thinking OR altered consciousness. class="guideline-li">Hypoactive delirium is the most common subtype yet the most frequently missed; always screen with CAM in older adults, post-surgical patients, and those with pre-existing cognitive impairment.
- Common precipitants include infection (UTI, pneumonia), anticholinergic and psychoactive medications (opioids, benzodiazepines, antipsychotics), metabolic derangements (hyponatraemia, hypoglycaemia, uraemia), and alcohol or benzodiazepine withdrawal.
- A systematic "delirium screen" should identify and treat reversible causes — use the mnemonic DIMS: Drugs, Infection, Metabolic, Structural/Sensory deprivation.
- Non-pharmacologic multicomponent interventions (reorientation, sleep hygiene, early mobilisation, hydration, hearing/visual aids) are first-line and reduce delirium incidence by 30–40%.
- Pharmacologic management is reserved for severe agitation threatening patient or staff safety — low-dose haloperidol (0.5–1 mg PO/IM) or quetiapine (12.5–25 mg PO) are first-line; avoid benzodiazepines except in alcohol/benzo withdrawal or hepatic encephalopathy.
- All antipsychotics carry a TGA black-box warning for increased mortality in dementia-related psychosis; use the lowest effective dose for the shortest duration and document indication clearly.
- Prevention strategies in high-risk patients (aged ≥65, hip fracture, ICU admission, pre-existing dementia) include the HELP programme components — multicomponent non-pharmacologic bundles reduce new-onset delirium by up to 40%.
- Aboriginal and Torres Strait Islander peoples may present with delirium at younger ages due to higher burden of chronic disease; cultural considerations, interpreter use, and family-centred care are essential.
- Delirium is associated with prolonged hospital stay, increased mortality (OR 1.9–3.2), accelerated cognitive decline, and higher rates of aged-care facility placement — post-discharge follow-up is mandatory.
- Mortality from delirium in older Australians ranges from 22–76% at one year depending on population and setting; early recognition and cause-directed treatment improve outcomes significantly.
Introduction & Australian Epidemiology
Delirium is a neuropsychiatric syndrome characterised by an acute disturbance in attention, awareness, and cognition that develops over hours to days, represents a change from baseline, and tends to fluctuate in severity over the course of the day. It is a medical emergency reflecting underlying physiological derangement rather than a primary psychiatric disorder.
In Australia, delirium remains significantly under-recognised. Prospective studies in Australian hospitals report detection rates of only 30–50% of cases meeting DSM-5 criteria, with hypoactive and mixed subtypes most frequently missed. The condition carries substantial morbidity and healthcare costs, with an estimated annual burden exceeding $2.7 billion to the Australian healthcare system.
Key Australian Data
| Setting | Prevalence / Incidence | Key Notes |
|---|---|---|
| General medical wards | 10–30% prevalence | Higher in patients aged ≥65 yrs |
| Emergency department (aged ≥65) | 8–17% | Often the first point of contact; screening on arrival critical |
| Post-operative (hip fracture) | 35–65% | Highest-risk surgical cohort in Australia |
| Intensive care unit | 45–87% | Use CAM-ICU; associated with prolonged ventilation |
| Residential aged care (new admissions) | 10–40% | Often misdiagnosed as behavioural disturbance of dementia |
| Palliative care | 28–83% in final weeks of life | Terminal delirium requires compassionate, individualised approach |
The Australian Institute of Health and Welfare (AIHW) reports that older Australians (≥65 years) account for approximately 80% of delirium-related hospitalisations. Aboriginal and Torres Strait Islander Australians, who experience a higher burden of chronic disease at younger ages, may develop delirium at ages 10–15 years younger than the non-Indigenous population. Delirium is associated with a 1.9- to 3.2-fold increase in in-hospital mortality, a 2- to 3-fold increase in rates of new residential aged-care placement, and significantly accelerated long-term cognitive decline.
Recognition in Primary Care & Emergency Department
Early recognition is the single most important step in delirium management. The 2023 ACSQHC Delirium Clinical Care Standard recommends that all patients aged ≥65 years and all patients with known cognitive impairment presenting to any Australian healthcare setting should be screened for delirium using a validated tool.
Core Diagnostic Features (DSM-5-TR)
- Criterion A: Disturbance in attention and awareness
- Criterion B: Develops over a short period (hours to days), represents a change from baseline, and tends to fluctuate in severity during the day
- Criterion C: Additional disturbance in cognition (memory deficit, disorientation, language disturbance, visuospatial ability, perception)
- Criterion D: Criteria A and C are not better explained by a pre-existing, established, or evolving neurocognitive disorder
- Criterion E: There is evidence from the history, physical examination, or laboratory findings that the disturbance is a direct physiological consequence of another medical condition, substance intoxication/withdrawal, or multiple aetiologies
Confusion Assessment Method (CAM)
The CAM (Inouye et al., 1990) is the most widely validated and recommended bedside tool for delirium screening in Australian clinical practice. The short CAM can be administered in 5 minutes. The CAM-ICU is validated for mechanically ventilated patients. The 4AT (rapid assessment tool) is an alternative that requires no training and has high sensitivity (90%) in ED settings.
Delirium diagnosis by CAM requires Features 1 + 2 + either 3 or 4:
Delirium Subtypes
Differentiating Delirium from Dementia
| Feature | Delirium | Dementia |
|---|---|---|
| Onset | Acute (hours to days) | Insidious (months to years) |
| Course | Fluctuating, often worse at night (sundowning) | Gradually progressive |
| Attention | Impaired (hallmark feature) | Relatively preserved until late stages |
| Consciousness | Altered (clouded, hyperalert, or lethargic) | Clear until advanced disease |
| Reversibility | Usually reversible when cause treated | Generally irreversible (though treatable causes may coexist) |
| Memory | Impaired for events during delirium (often no recall) | Recent memory impaired early, remote memory impaired late |
| Perception | Visual hallucinations common; illusions | Hallucinations less common until advanced Lewy body dementia |
| Psychomotor | Hyperactive, hypoactive, or mixed | Usually normal early; abulia late |
Practical Screening Protocol for Australian EDs and Wards
- Trigger: All patients aged ≥65 years; all patients with known or suspected cognitive impairment; all post-operative patients (especially hip fracture); all ICU admissions; any acute change in behaviour or consciousness.
- Tool: Short CAM (5 min) or 4AT (2 min, no training required). For ICU: CAM-ICU.
- Frequency: On presentation, then at minimum every shift (q8–12h) for at-risk patients.
- Document: Record CAM result in the medical record and handover to the next clinician.
- If positive: Initiate cause-directed workup immediately (see Investigations and Initial Management).
Common Precipitants
Delirium is a final common pathway for multiple aetiologies. It is rarely unifactorial — most patients have 2–4 contributing precipitants simultaneously. A systematic approach using the DIMS mnemonic ensures no major category is overlooked.
D — Drugs (anticholinergics, opioids, benzodiazepines, corticosteroids, polypharmacy)
I — Infection (UTI, pneumonia, cellulitis, COVID-19, meningitis)
M — Metabolic (electrolytes, glucose, renal, hepatic, thyroid, hypoxia, dehydration)
S — Structural / Sensory (stroke, haemorrhage, seizure, pain, constipation, urinary retention, sensory deprivation)
Drugs — Common Culprits
Medications account for 30–40% of delirium cases in Australian hospitalised patients. Polypharmacy (≥5 medications) is itself an independent risk factor. High-risk drug classes include:
| Drug Class | Examples | Mechanism | Action |
|---|---|---|---|
| Anticholinergics | Promethazine, hyoscine, oxybutynin, amitriptyline, chlorphenamine | Central muscarinic blockade | Cease or substitute with non-anticholinergic alternative |
| Benzodiazepines | Diazepam, midazolam, temazepam, lorazepam | GABA-A potentiation, oversedation, paradoxical agitation | Taper if possible; avoid new prescriptions in elderly |
| Opioids | Morphine, oxycodone, tramadol, fentanyl, codeine | Mu-receptor effects, neuroexcitatory metabolites (M3G, M6G) | Reduce dose, rotate opioid, ensure adequate analgesia (untreated pain also causes delirium) |
| Corticosteroids | Prednisolone ≥40 mg, dexamethasone, methylprednisolone | Steroid psychosis, dose-dependent | Reduce dose if possible; typically occurs within first 5 days |
| Antipsychotics | Haloperidol (paradoxical), risperidone, olanzapine | Anticholinergic burden, EPS, metabolic effects | Review indication; avoid using to "treat" delirium without clear cause-directed action |
| Fluoroquinolones | Ciprofloxacin, moxifloxacin | GABA inhibition, CNS penetration | Consider alternative antibiotic if delirium onset temporally associated |
Infection
- Urinary tract infection: Most commonly attributed infectious cause in elderly Australians — but beware of asymptomatic bacteriuria (do not treat in catheterised or non-symptomatic patients simply because delirium is present).
- Pneumonia: Community-acquired and aspiration pneumonia. Consider in any delirious patient with hypoxia or new cough.
- Cellulitis / skin and soft-tissue infection: Particularly in patients with diabetes or peripheral vascular disease.
- COVID-19 and influenza: Delirium may be the presenting feature in older adults, even without prominent respiratory symptoms.
- Meningitis / encephalitis: Consider in patients with fever, neck stiffness, photophobia, focal neurological signs, or immunosuppression.
- Occult bacteraemia: Always obtain blood cultures in the septic, delirious patient.
Metabolic Derangements
| Derangement | Common Causes | Key Point |
|---|---|---|
| Hyponatraemia (Na <130 mmol/L) | Diuretics, SIADH, dehydration, DDAVP | Correct slowly (<10 mmol/L per 24 h) to avoid osmotic demyelination |
| Hypernatraemia (Na >150 mmol/L) | Dehydration, diabetes insipidus, inadequate water access | Common in elderly in residential care; assess hydration status |
| Hypoglycaemia (<4.0 mmol/L) | Insulin, sulfonylureas, missed meals, sepsis | Treat urgently; glucose <2.8 mmol/L is a medical emergency |
| Uraemia (eGFR <15 mL/min) | Acute kidney injury, chronic kidney disease | Consider dialysis; adjust all renally cleared medications |
| Hepatic encephalopathy | Cirrhosis, portal hypertension, GI bleeding, infection | Lactulose + rifaximin; precipitant-directed treatment |
| Hypoxia / hypercapnia | COPD exacerbation, PE, pneumonia, heart failure | ABG essential if SpO₂ <94% or respiratory distress |
| Thyroid dysfunction | Myxoedema madness (hypothyroid), thyrotoxicosis | TFTs should be part of the delirium workup in older adults |
| Wernicke's encephalopathy | Alcohol dependence, malnutrition, bariatric surgery, hyperemesis | Give IV thiamine 300–500 mg BEFORE glucose in suspected cases |
Substance Use & Withdrawal
- Alcohol withdrawal delirium (delirium tremens): Typically onset 48–96 hours after last drink. Mortality 5–15% if untreated. Use the CIWA-Ar protocol; manage with benzodiazepines (diazepam or lorazepam) in a monitored setting. PBS-listed diazepam 5–20 mg PO/IV with symptom-triggered dosing.
- Benzodiazepine withdrawal: Can occur after only 2–4 weeks of regular use. Gradual taper recommended; abrupt cessation in ICU patients is a common precipitant.
- Opioid withdrawal: Less commonly causes delirium but contributes to agitation and autonomic instability.
- Anticholinergic toxicity: Flushing, dry skin, mydriasis, tachycardia, urinary retention, agitation. Physostigmine 0.5–2 mg IV (specialist use only) for severe cases.
- Cannabis, methamphetamine, synthetic cannabinoids: Increasingly recognised as delirium precipitants in younger Australian adults, particularly in regional and remote areas.
Structural & Sensory Causes
- Stroke / intracranial haemorrhage: Especially right hemisphere, thalamic, or posterior fossa lesions.
- Post-ictal state: Non-convulsive status epilepticus should be considered in unexplained persistent delirium — EEG monitoring required.
- Pain: Under-treated pain is a major and modifiable cause. Use validated pain scales suitable for non-verbal patients (e.g., Abbey Pain Scale in dementia).
- Urinary retention / constipation: Easily identified and treated; bladder scan and abdominal examination should be routine in delirium assessment.
- Sensory deprivation: Absent hearing aids or glasses, dark single rooms, lack of familiar objects — particularly important for patients with pre-existing dementia.
Pathophysiology
Delirium pathophysiology is multifactorial and incompletely understood. Current evidence supports a model of widespread neuroinflammation, neurotransmitter imbalance, and impaired connectivity in brain networks subserving attention and executive function.
Key Neurobiological Mechanisms
- Neuroinflammation: Systemic inflammatory mediators (IL-1β, IL-6, TNF-α) cross a disrupted blood–brain barrier, activate microglia, and cause widespread neuronal dysfunction. This "sickness behaviour" model explains why systemic infection causes cerebral dysfunction.
- Cholinergic deficiency: The most consistent neurotransmitter finding. Acetylcholine is essential for attention, arousal, and memory encoding. Anticholinergic medications and acetylcholinesterase depletion in ageing brains directly impair these functions.
- Dopaminergic excess: Excess dopamine contributes to hyperactive delirium and psychotic features. This underpins the use of dopamine-blocking antipsychotics in symptomatic management.
- GABA/glutamate imbalance: Impaired GABAergic inhibition and excessive glutamatergic excitation (NMDA receptor dysfunction) contribute to neuronal excitotoxicity. Hepatic encephalopathy represents a GABA-ergic excess model.
- Impaired network connectivity: Functional MRI studies demonstrate reduced connectivity between the thalamus, prefrontal cortex, and posterior parietal cortex — regions critical for attention and consciousness.
- Chronic vulnerability (brain reserve): Patients with pre-existing neurodegeneration (Alzheimer's, Lewy body, vascular dementia) have reduced brain reserve and are more susceptible to delirium from any given physiological insult.
Investigations
The delirium workup should be directed by clinical assessment, but a minimum set of baseline investigations is recommended for all patients with new-onset delirium. Additional tests are guided by the DIMS screen and clinical findings.
Essential Investigations
Directed Investigations (Based on Clinical Suspicion)
Risk Stratification & Severity Scoring
Identifying High-Risk Patients
Prevention begins with identifying those at greatest risk. The following factors are independently associated with delirium in Australian hospital cohorts:
| Risk Factor | Odds Ratio | Modifiable? |
|---|---|---|
| Pre-existing dementia / cognitive impairment | 2.5–6.3 | Not directly, but environmental modifications help |
| Age ≥65 years (especially ≥85) | 1.6–3.1 | No |
| Hip fracture / emergency surgery | 3.9–8.7 | Partially — anaesthetic and analgesic choice, early mobilisation |
| Sensory impairment (vision or hearing) | 1.6–2.5 | Yes — ensure glasses and hearing aids are in place |
| Polypharmacy (≥5 medications) | 1.5–2.4 | Yes — medication review, deprescribing |
| Severe illness (APACHE II ≥15) | 2.0–3.5 | Partially — treat underlying illness |
| Dehydration / malnutrition | 1.8–3.0 | Yes — fluid and nutritional support |
| Infection at admission | 1.8–2.7 | Yes — prompt antimicrobial therapy |
| Indwelling catheter | 1.4–2.2 | Yes — avoid unless clearly indicated; remove early |
| Previous episode of delirium | 2.0–5.7 | Not directly, but informs proactive prevention |
Severity Assessment
There is no single validated "severity score" for delirium used universally in Australian practice. However, the following clinical framework guides escalation:
Richmond Agitation–Sedation Scale (RASS)
| Score | Term | Description |
|---|---|---|
| +4 | Combative | Combative, violent, immediate danger to staff |
| +3 | Very agitated | Pulling at tubes/catheters, aggressive behaviour |
| +2 | Agitated | Frequent non-purposeful movement, fights ventilator |
| +1 | Restless | Anxious but movements not aggressive or vigorous |
| 0 | Alert and calm | Spontaneously pays attention to carer |
| −1 | Drowsy | Not fully alert but sustained awakening to voice (eye opening/contact >10 s) |
| −2 | Light sedation | Briefly awakens to voice (eye opening/contact <10 s) |
| −3 | Moderate sedation | Movement or eye opening to voice (no eye contact) |
| −4 | Deep sedation | No response to voice, movement or eye opening to physical stimulation |
| −5 | Unarousable | No response to voice or physical stimulation |
Initial Management
Management of delirium follows three parallel tracks: (1) identify and treat the underlying cause(s), (2) implement non-pharmacologic supportive measures, and (3) consider cautious pharmacologic management for severe distress or safety concerns. Prevention in high-risk patients is the fourth pillar.
Track 1 — Identify and Treat the Cause
The single most effective intervention for delirium is treating the underlying precipitant. Every delirious patient should undergo a systematic cause-directed workup using the DIMS mnemonic (see Common Precipitants section). Key actions include:
- Medication review: Cease or reduce dose of all anticholinergic, sedative, and psychoactive medications where clinically safe. Involve a pharmacist for anticholinergic burden scoring.
- Infection management: Commence empirical antibiotics per local hospital antibiogram if infection suspected. For community presentations, refer to eTG Antibiotic guidelines — amoxicillin + clavulanate for UTI, ceftriaxone + azithromycin for pneumonia (adjust for local resistance patterns and patient allergies).
- Metabolic correction: Replace electrolytes, correct glucose, manage renal/hepatic failure. Administer IV thiamine 300–500 mg before glucose in any malnourished or alcohol-dependent patient.
- Pain management: Treat unrecognised pain with regular simple analgesia (paracetamol 1 g QID PO/IV) and judicious opioid titration. Paradoxically, both untreated pain and excessive opioids can cause delirium — use the lowest effective dose.
- Hydration and nutrition: Assess fluid status; commence IV normal saline if dehydrated. Ensure adequate oral intake with assistance at mealtimes.
- Manage constipation and urinary retention: Bladder scan (retention if >400 mL post-void). Laxatives (macrogol or lactulose) for constipation.
Track 2 — Non-Pharmacologic Multicomponent Interventions
Non-pharmacologic measures are first-line for all patients with delirium and form the cornerstone of prevention for high-risk patients. The Hospital Elder Life Program (HELP) model, adapted for Australian hospitals, has a strong evidence base.
Track 3 — Cautious Antipsychotic Use
Track 4 — Prevention in High-Risk Patients
Prevention is more effective than treatment. Multicomponent non-pharmacologic interventions can reduce new-onset delirium by 30–40% in high-risk populations. The Hospital Elder Life Program (HELP) and equivalent Australian models (e.g., Melbourne Ageing Research Collaboration guidelines) provide the framework.
- Orientation board at bedside (name, date, location, daily schedule)
- Ensure glasses and hearing aids are in use
- Early mobilisation (sit out of bed by post-op day 0–1 for surgical patients)
- Sleep protocol (lights off 21:00–06:00, minimise noise, avoid benzodiazepines)
- Hydration protocol (target ≥1.5 L/day oral intake or IV equivalent)
- Cognitive stimulation (daily therapeutic conversation, reminiscence)
- Medication review (pharmacy-led anticholinergic burden reduction)
- Avoid unnecessary catheters and restraints
- Low-dose haloperidol (0.5 mg PO BD) has been studied for post-operative delirium prevention in hip fracture patients (HOLIDADE trial and others) — results are mixed; NOT routinely recommended for prophylaxis.
- Melatonin (0.5–3 mg nocte) — some evidence for reducing incidence in medical inpatients; not PBS-listed for this indication.
- Dexmedetomidine — reduces ICU delirium incidence versus benzodiazepine sedation; ICU specialist use only.
- Cholinesterase inhibitors (donepezil, rivastigmine) — NO evidence for delirium prevention or treatment; the MODD trial was negative. Do not start for this indication.
Monitoring
In-Hospital Monitoring
Monitoring Antipsychotic Therapy
- ECG: Baseline and at 24–48 hours for haloperidol. Discontinue if QTc >500 ms or increases by >60 ms from baseline.
- Neurological status: Assess for extrapyramidal symptoms (EPS), akathisia, neuroleptic malignant syndrome (NMS) — fever, rigidity, autonomic instability, elevated CK. Stop antipsychotic immediately if NMS suspected.
- Sedation level: RASS target 0 to −1 for patients on antipsychotics. Over-sedation masks delirium and impedes assessment.
- Falls risk: Antipsychotics increase fall risk by 1.5–2× in elderly patients. Implement falls precautions.
- Cessation plan: Taper and cease antipsychotics within 48–72 hours of delirium resolution. If continuing beyond 1 week, formal specialist review is required with documented rationale.
Special Populations
Pregnancy & Postpartum
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Australians experience a significantly higher burden of the conditions that precipitate delirium — including diabetes, chronic kidney disease, rheumatic heart disease, ear disease and hearing loss, and harmful alcohol use — and often at younger ages than the non-Indigenous population. Delirium in Indigenous Australians may therefore occur in patients aged 45–65 years who would not typically be flagged as "high risk" by age-based screening algorithms alone.
📚 References
- 1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Arlington, VA: APA Publishing; 2022. [Delirium diagnostic criteria — Chapter: Neurocognitive Disorders]
- 2. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
- 3. Inouye SK, Bogardus ST, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–676. doi:10.1056/NEJM199903043400901
- 4. Australian Commission on Safety and Quality in Health Care (ACSQHC). Delirium Clinical Care Standard. Sydney: ACSQHC; 2023. Available at: www.safetyandquality.gov.au
- 5. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006;35(4):350–364. doi:10.1093/ageing/afl005
- 6. Witlox J, Eurelings LSM, de Jonghe JFM, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304(4):443–451. doi:10.1001/jama.2010.1013
- 7. Australian Institute of Health and Welfare (AIHW). Older Australians. AIHW; 2023. Available at: www.aihw.gov.au/reports/older-people/older-australians
- 8. Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU study): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2013;1(7):515–523. doi:10.1026/S2213-2600(13)70166-8
- 9. van Eijk MM, Roes KC, Honing ML, et al. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010;376(9755):1829–1837. doi:10.1016/S0140-6736(10)61855-7
- 10. Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2018;6(6):CD005594. doi:10.1002/14651858.CD005594.pub3
- 11. Reston J, Schoelles KM. In-facility delirium prevention programs as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):375–380. doi:10.7326/0003-4819-158-5-201303051-00006
- 12. Royal Australian and New Zealand College of Psychiatrists (RANZCP). Practice Guideline for the Treatment of Delirium. Melbourne: RANZCP; 2021.
- 13. NHMRC Clinical Practice Guidelines and Expert Panels. Australian Clinical Practice Guidelines — Delirium in Older People. Canberra: NHMRC; 2023.
- 14. Traube C, Silver G, Kearney J, et al. Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the PICU*. Crit Care Med. 2014;42(3):656–663. doi:10.1097/CCM.0000000000000044
- 15. RHDAustralia (Remote Health Division, Flinders University). Alcohol Management Plans and Fetal Alcohol Spectrum Disorder Resources. Darwin: RHDAustralia; 2023. Available at: www.rhdaustralia.org.au
- 16. O'Hanlon S, Inouye SK. Delirium: a missing piece of the pandemic puzzle. Age Ageing. 2020;49(4):497–498. doi:10.1093/ageing/afaa091
- 17. Therapeutic Goods Administration (TGA). Antipsychotic Medicines and Increased Risk of Death in Elderly Patients with Dementia — Black Box Warning. Canberra: TGA, Department of Health and Aged Care; 2023.