📋 Key Information Summary
- Dizziness is a common presenting complaint in Australian general practice and emergency departments, accounting for approximately 3–5% of ED presentations and 1–2% of GP consultations annually.
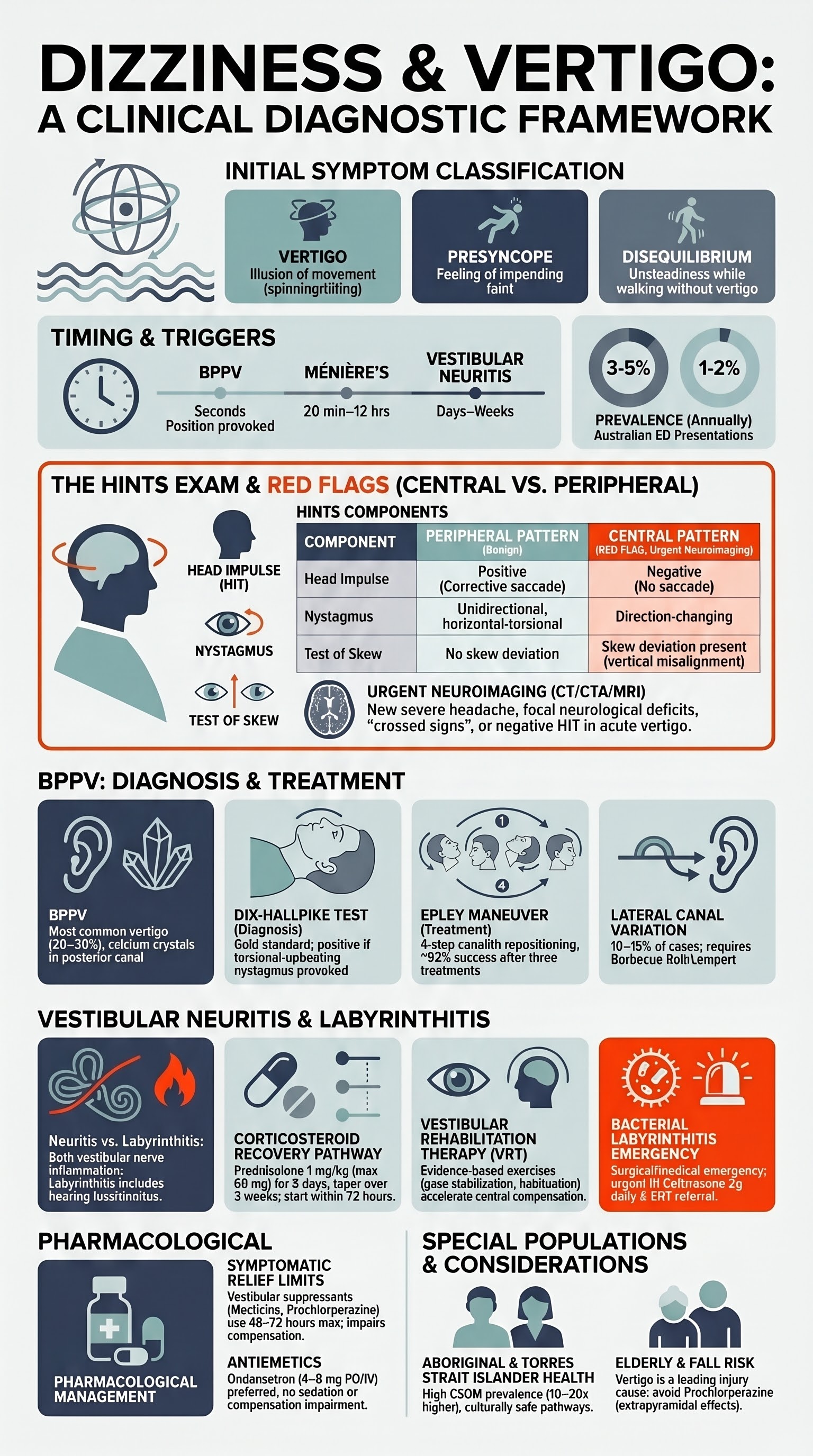
- Always distinguish true vertigo (illusion of movement) from presyncope, disequilibrium, and non-specific dizziness — each has a distinct differential diagnosis and management pathway.
- The HINTS exam (Head Impulse, Nystagmus, Test of Skew) is a bedside examination that can differentiate central from peripheral causes with high sensitivity and specificity when performed acutely by a trained clinician.
- Red flags for central pathology include new-onset severe headache, focal neurological deficits, dysarthria, diplopia, ataxia, crossed signs, cardiovascular risk factors, and anticoagulant use — these mandate urgent neuroimaging (CT/CTA ± MRI).
- Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo (20–30% of cases), diagnosed with the Dix–Hallpike test, and treated with the Epley maneuver — an effective, low-cost, office-based treatment.
- Posterior canal BPPV accounts for ~85% of cases and produces torsional-upbeating nystagmus on Dix–Hallpike; lateral canal BPPV produces direction-changing horizontal nystagmus and is managed with the barbecue roll or Lempert maneuver.
- Vestibular neuritis presents with acute-onset, prolonged (days to weeks) spontaneous vertigo, unilateral vestibular hypofunction, and a positive head-impulse test — there is no cochlear involvement.
- Labyrinthitis is vestibular neuritis with concurrent hearing loss or tinnitus, suggesting cochlear involvement; it may be viral or bacterial (the latter requires urgent ENT referral).
- Early corticosteroids (methylprednisolone 100 mg IV then oral taper, or prednisolone 1 mg/kg PO daily tapered over 3 weeks) may improve vestibular recovery in vestibular neuritis, though evidence is mixed.
- Vestibular rehabilitation therapy (VRT) accelerates central compensation and recovery and should be offered to all patients with vestibular neuritis and labyrinthitis.
- Meclizine and other vestibular suppressants provide symptomatic relief but should be used short-term only (48–72 hours) as they impair central compensation.
- Aboriginal and Torres Strait Islander peoples in remote communities may have limited access to specialist vestibular assessment and imaging; culturally safe education, community-based rehabilitation, and telehealth pathways are essential.
Initial Assessment — Timing, Triggers, HINTS Exam, and Red Flags
History: Characterising the Dizziness
A structured history is the single most important diagnostic step. Ask the patient to describe their symptoms in their own words and then clarify using the following framework.
| Dizziness Type | Description | Typical Causes |
|---|---|---|
| Vertigo | Illusion of rotational or linear movement of self or environment | BPPV, vestibular neuritis, labyrinthitis, Ménière disease, vestibular migraine, posterior fossa stroke |
| Presyncope | Feeling of impending faint or blackout | Orthostatic hypotension, cardiac arrhythmia, vasovagal syncope, PE |
| Disequilibrium | Unsteadiness or imbalance without true vertigo, worse with walking | Peripheral neuropathy, cerebellar disease, vestibulopathy, medication effects |
| Non-specific dizziness | Lightheadedness, floating, vague sense of disorientation | Anxiety, hyperventilation, medication side effects, metabolic causes |
Key History Features — Timing and Triggers
- Onset: Sudden (seconds — BPPV, TIA/stroke) vs acute (minutes to hours — Ménière, vestibular migraine) vs gradual/subacute over hours to days (vestibular neuritis, labyrinthitis).
- Duration of individual episodes: Seconds (BPPV), 20 min to 12 h (Ménière), hours to days (vestibular neuritis, stroke).
- Positional provocation: Turning in bed, looking up, bending forward → suggests BPPV or positional central vertigo.
- Associated symptoms: Hearing loss or tinnitus (labyrinthitis, Ménière, AICA stroke), nausea/vomiting (all vestibular causes), headache (vestibular migraine, SAH), diplopia or dysarthria (central pathology).
- Precipitants: Recent upper respiratory tract infection (vestibular neuritis), head trauma (BPPV, perilymph fistula), Valsalva (superior canal dehiscence).
- Cardiovascular risk factors: Hypertension, diabetes, atrial fibrillation, smoking, hyperlipidaemia — increases suspicion for vertebrobasilar ischaemia.
- Medications: Aminoglycosides, loop diuretics, anticonvulsants, antihypertensives, SSRIs — can cause vestibulotoxicity or orthostatic symptoms.
- New severe headache, particularly "thunderclap" onset → consider SAH
- Focal neurological deficit (hemiparesis, ataxia, dysarthria, dysphagia)
- Diplopia, bilateral visual changes, or loss of vision
- Crossed signs (ipsilateral facial and contralateral body symptoms)
- Hearing loss with acute vertigo in presence of cardiovascular risk factors (AICA territory infarct)
- HINTS exam with normal head-impulse test + direction-changing nystagmus or skew deviation → central until proven otherwise
- Anticoagulant or antiplatelet use with new vertigo and neurological signs
- Progressive unilateral hearing loss with vertigo → acoustic neuroma exclusion
HINTS Examination — Head Impulse, Nystagmus, Test of Skew
The HINTS exam should be performed at the bedside in any patient presenting with acute continuous vertigo and nystagmus. It can be more accurate than early diffusion-weighted MRI (< 48 hours) for identifying posterior fossa stroke. It requires training and should be performed by experienced clinicians (emergency physicians, neurologists, or vestibular physiotherapists).
| Component | Technique | Peripheral Pattern | Central Pattern (Red Flag) |
|---|---|---|---|
| H — Head Impulse Test | Patient fixates on examiner's nose; examiner turns head 10–20° rapidly to one side; observe for corrective saccade | Positive — corrective saccade present (vestibular hypofunction) | Negative — no corrective saccade (normal or bilateral); a negative HIT in acute vertigo is concerning for stroke |
| I — Nystagmus Direction | Observe nystagmus in primary gaze, rightward gaze, and leftward gaze | Unidirectional, horizontal-torsional, beating away from lesion side, suppressed with fixation | Direction-changing (beats one way on right gaze, opposite on left gaze) or purely vertical/torsional nystagmus in primary gaze |
| N — Test of Skew | Cover–uncover test alternating eyes; look for vertical corrective refixation | No skew deviation | Skew deviation present — vertical misalignment of the visual axes, indicates brainstem/cerebellar pathology |
Additional Bedside Tests
- Dix–Hallpike test: Provokes posterior canal BPPV — see BPPV section below.
- Romberg and tandem gait: Impaired tandem gait with eyes open may indicate central pathology; bilateral vestibular loss causes unsteadiness with eyes closed (positive Romberg).
- Fukuda stepping test: Patient marches on the spot with eyes closed; > 30° rotation suggests unilateral vestibular hypofunction.
- Auditory assessment: Whispered voice test or finger rub — hearing loss with vertigo suggests labyrinthitis, Ménière, or AICA stroke.
Benign Paroxysmal Positional Vertigo (BPPV)
BPPV is the most common vestibular disorder, accounting for 20–30% of all vertigo presentations in Australian emergency departments and general practice. It is caused by displaced otoconia (calcium carbonate crystals) from the utricle that migrate into the semicircular canals, most commonly the posterior canal (~85% of cases).
Aetiology and Risk Factors
- Most cases are idiopathic; age > 50 years is the strongest risk factor.
- Head trauma (even minor) — post-traumatic BPPV accounts for ~20% in younger populations.
- Associated with vestibular neuritis, Ménière disease, prolonged bed rest, and inner ear surgery.
- Vitamin D deficiency is emerging as a risk factor; studies show lower serum 25-OH vitamin D in recurrent BPPV patients.
Dix–Hallpike Test — Diagnostic Technique
The Dix–Hallpike test is the gold standard for diagnosing posterior canal BPPV. It should be performed in all patients with positional vertigo.
Epley Maneuver — Canalith Repositioning
The Epley maneuver is the first-line treatment for posterior canal BPPV. It has a single-treatment success rate of approximately 80% and a cumulative success rate of ~92% after three treatments. It can be performed in general practice, emergency departments, or by vestibular physiotherapists.
Pharmacotherapy — Symptomatic Relief
Patient Education — Self-Treatment and Recurrence
- Teach patients the home Epley maneuver for self-treatment of recurrences. The Brandt–Daroff exercises can also be prescribed as an alternative home exercise program.
- Recurrence rates are approximately 30–50% within 5 years — counsel patients that recurrence is common and manageable.
- Avoid head-hanging positions for 48 hours after treatment (e.g., hairdresser basins, gardening, bending).
- Sleep with 2–3 pillows for 48 hours post-maneuver; avoid sleeping on the affected side for one week.
- Consider checking serum vitamin D levels and supplementing if deficient (especially in recurrent cases).
- Referral to a vestibular physiotherapist is recommended if two or more Epley treatments are unsuccessful, if the canal involved is lateral (requires different maneuver), or if the patient cannot tolerate the procedure.
Vestibular Neuritis & Labyrinthitis
Definitions and Pathophysiology
Inflammation of the vestibular nerve (superior branch most commonly affected), likely viral in aetiology (HSV-1 reactivation from the vestibular ganglion is the leading hypothesis). Presents with acute vertigo, nausea/vomiting, and unilateral vestibular hypofunction. No hearing loss.
Inflammation involving both the vestibular nerve and cochlea (labyrinth). Viral labyrinthitis is the most common form. Concurrent sensorineural hearing loss or tinnitus differentiates it from vestibular neuritis. Bacterial labyrinthitis (secondary to otitis media or meningitis) is a medical emergency requiring urgent antibiotics.
Clinical Presentation
- Onset: Acute, often upon waking, or developing over hours. Severe rotational vertigo with nausea and vomiting.
- Duration: Spontaneous vertigo lasts days to 2 weeks, gradually improving. Residual imbalance may persist for weeks to months.
- Examination findings:
- Spontaneous horizontal-torsional nystagmus beating away from the affected side (unidirectional).
- Positive head-impulse test toward the affected side (corrective saccade).
- No skew deviation; unidirectional nystagmus → peripheral pattern on HINTS.
- Falls toward the affected side on Romberg and tandem gait.
- Labyrinthitis additionally: Ipsilateral sensorineural hearing loss and/or tinnitus. If hearing loss is profound and sudden → consider bacterial labyrinthitis or inner ear ischaemia (AICA territory stroke).
Exclusion of Stroke
- If any red flags are present → proceed to urgent CT with CTA (or MRI with DWI if available and not delayed).
- If HINTS exam shows central pattern (normal HIT, direction-changing nystagmus, or skew deviation) → urgent neuroimaging and neurology/stroke unit referral.
- If HINTS cannot be performed (clinician inexperience, patient unable to cooperate) → neuroimaging.
- If stroke is confirmed → manage per Australian Clinical Guidelines for Stroke Management (Stroke Foundation, 2023).
Investigations
Pharmacological Management
Symptomatic Treatment (Vestibular Suppression — Short-Term)
Corticosteroid Therapy — Vestibular Recovery
Evidence from randomised controlled trials (Strupp et al., 2004; Fishman et al., 2011) suggests that early corticosteroid administration may improve vestibular recovery in vestibular neuritis, although the evidence is not definitive and practice varies. Current recommendations from international vestibular guidelines are to consider corticosteroids within the first 72 hours of symptom onset.
Vestibular Rehabilitation Therapy (VRT)
Vestibular rehabilitation therapy is an evidence-based exercise program designed to promote central vestibular compensation. It should be offered to all patients with vestibular neuritis and labyrinthitis, ideally starting within the first 1–2 weeks once nausea is controlled.
- Components of VRT:
- Gaze stabilisation exercises: VOR x1 (fixate on target while moving head) and VOR x2 (moving target and head simultaneously).
- Habituation exercises: Repeated exposure to provocative movements to reduce motion sensitivity.
- Balance and gait training: Static and dynamic balance tasks with progressively reduced base of support and visual input.
- Access in Australia: Vestibular physiotherapists are available in most metropolitan areas and some regional centres. Referral can be made directly from GP. The Australian Physiotherapy Association maintains a directory of vestibular-trained physiotherapists.
- MBS Items for physiotherapy: Medicare-subsidised physiotherapy may be available through a GP Management Plan (GPMP) and Team Care Arrangement (TCA) — MBS Item 10960 (up to 5 allied health sessions per calendar year). Enhanced Primary Care (EPC) referrals are commonly used.
- Duration: Typically 6–12 weeks of supervised sessions with a home exercise program. Most patients with vestibular neuritis recover substantially within 3–6 months, though residual dizziness may persist.
Monitoring and Follow-Up
- Review at 1–2 weeks to assess symptom trajectory, check for BPPV development (secondary BPPV occurs in ~15% of vestibular neuritis cases), and reinforce vestibular rehabilitation exercises.
- Audiometry at 2–4 weeks if labyrinthitis (to document hearing recovery or identify permanent sensorineural loss).
- If symptoms are not improving by 4–6 weeks → consider MRI brain, specialist referral, or re-evaluation of diagnosis.
- Driving safety: Advise patients not to drive until vertigo has resolved and they can perform a rapid head turn without triggering symptoms. Austroads guidelines for medical fitness to drive should be followed.
Bacterial Labyrinthitis — An Urgent Distinction
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of ear disease and its complications, which directly impacts vestibular health. Otitis media with effusion (OME) and chronic suppurative otitis media (CSOM) are highly prevalent in remote Aboriginal and Torres Strait Islander communities, particularly in children, and can lead to conductive hearing loss, labyrinthine complications, and vestibular dysfunction. These conditions are driven by socioeconomic disadvantage, overcrowded housing, limited access to primary healthcare, and environmental factors.
Barriers to Care and Considerations
Quick Reference — Vestibular Syndrome to Treatment
📚 References
- 1. Strupp M, Zingler VC, Arbusow V, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. 2004;351(4):354-361.
- 2. Fishman JM, Burgess C, Waddell A. Corticosteroids for the treatment of idiopathic acute vestibular dysfunction (vestibular neuritis). Cochrane Database Syst Rev. 2011;(5):CD008607.
- 3. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009;40(11):3504-3510.
- 4. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngol Head Neck Surg. 2017;156(3_suppl):S1-S47.
- 5. Stroke Foundation. Clinical Guidelines for Stroke Management 2023. Melbourne: Stroke Foundation; 2023. Available at: https://informme.org.au.
- 6. Curthoys IS, MacDougall HG, Vidal PP, de Waele C. Sustained and transient vestibular systems: a physiological basis for interpreting vestibular function. Front Neurol. 2017;8:114.
- 7. Australian Institute of Health and Welfare (AIHW). Ear health in Aboriginal and Torres Strait Islander children. Cat. no. IHW 244. Canberra: AIHW; 2022.
- 8. Newman-Toker DE, Hsieh YH, Camargo CA Jr, Pelliccia A, Edlow JA. Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample. Mayo Clin Proc. 2008;83(7):765-775.
- 9. McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. 2015;(1):CD005397.
- 10. Austroads. Assessing Fitness to Drive for Commercial and Private Vehicle Drivers. Sydney: Austroads; 2022. Available at: https://austroads.com.au.
- 11. Maslovara S, Soldo SB, Puksec M, Gruber H. Recurrent benign paroxysmal positional vertigo and vitamin D deficiency. Med Glas (Zenica). 2018;15(1):22-27.
- 12. National Aboriginal Community Controlled Health Organisation (NACCHO). National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People. 3rd ed. Melbourne: RACGP/NACCHO; 2018.
- 13. Hain TC, Uddin M. Pharmacological treatment of vertigo. CNS Drugs. 2003;17(2):85-100.
- 14. Aw ST, Todd MJ, Aw GE, Magnussen JS, Curthoys IS, Halmagyi GM. Head impulse test in vestibular neuritis: vestibulo-ocular reflex and cerebellar control. Prog Brain Res. 2008;171:277-283.