📋 Key Information Summary
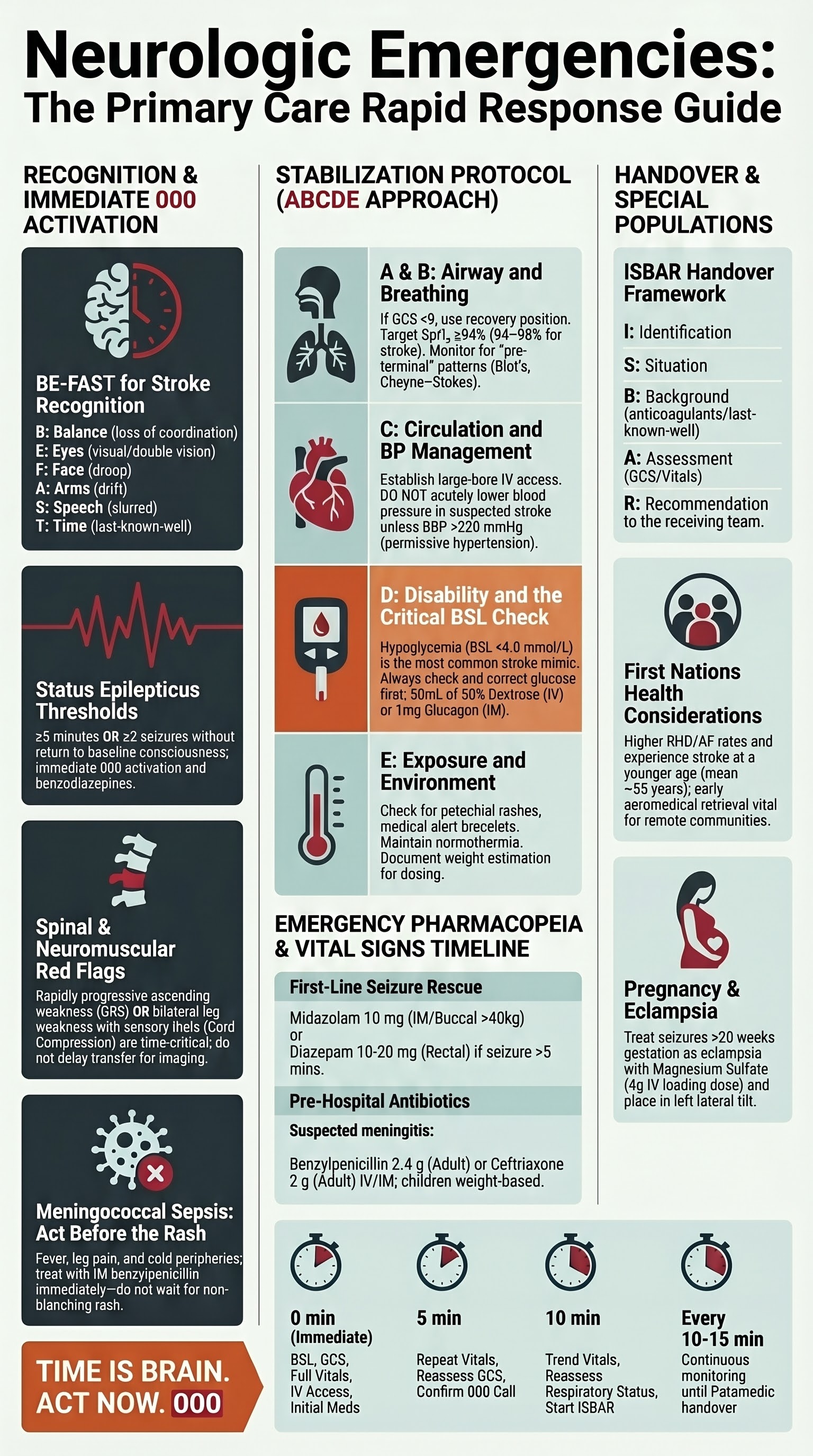
- Suspected acute stroke with symptom onset within 4.5 hours requires an immediate Triple Zero (000) call — do NOT drive the patient yourself; paramedics can pre-notify the stroke team and initiate pre-hospital thrombolysis pathways.
- Use the FAST screen (Face, Arms, Speech, Time) and note exact last-known-well time; this determines eligibility for IV alteplase (tenecteplase increasingly used in some Australian centres) and endovascular thrombectomy up to 24 hours in select cases.
- Status epilepticus is defined as seizure lasting ≥5 minutes or ≥2 seizures without return to baseline — administer IM midazolam 10 mg (>40 kg) or rectal/buccal diazepam as first-line benzodiazepine before ambulance arrival.
- Acute paraplegia or rapidly progressive ascending weakness (suspected Guillain–Barré syndrome or spinal cord compression) is a time-critical emergency requiring same-day hospital assessment and transfer.
- Suspected bacterial meningitis or meningococcal sepsis: administer IM benzylpenicillin 2.4 g (adults) or ceftriaxone 2 g IV/IM immediately if available, then call 000 — do not delay transfer for lumbar puncture in primary care.
- In the pre-transfer stabilization period, use the ABCDE approach: secure airway (recovery position if GCS <9), high-flow oxygen if SpO₂ <94%, IV access with 0.9% NaCl, BSL check, and continuous vital-sign monitoring.
- Document all findings, medications given, and exact times on the Australian Ambulance clinical handover form or ISBAR framework to ensure seamless transition of care.
- Hypoglycaemia (BSL <4.0 mmol/L) is the most common stroke mimic — always check and correct glucose before assuming a neurologic emergency is present.
- Blood pressure management in suspected stroke: do NOT lower BP acutely in primary care unless hypertensive emergency (systolic >220 mmHg) — permissive hypertension maintains cerebral perfusion.
- Aboriginal and Torres Strait Islander peoples experience stroke incidence 1.5–3 times higher than non-Indigenous Australians, with younger age of onset and higher mortality — culturally safe communication and community-based awareness programs are essential.
- Patients on anticoagulants (warfarin, DOACs) with suspected stroke require specific documentation of INR, last dose, and agent name — this directly influences thrombolysis eligibility.
- For recurrent seizure activity after benzodiazepine administration, position patient in recovery position, protect from injury, time the seizure, and communicate duration to paramedics — do NOT insert objects into the mouth.
Introduction & Australian Epidemiology
Neurologic emergencies represent some of the most time-critical presentations encountered in Australian primary care. General practitioners and practice nurses are frequently the first clinicians to assess patients with acute neurologic deterioration, and the actions taken in the first 10–30 minutes can profoundly influence long-term outcomes including mortality, functional independence, and quality of life.
This guideline provides a practical framework for Australian primary care clinicians to: (1) recognise neurologic emergencies that mandate immediate ambulance transfer, (2) initiate evidence-based stabilisation measures, and (3) communicate effectively with receiving emergency departments and specialist teams.
Australian Epidemiology
- Stroke: Approximately 38,000 Australians experience a new or recurrent stroke annually (Stroke Foundation, 2023). Stroke is the third leading cause of death and the leading cause of acquired disability. The Australian Stroke Clinical Registry (AuSCR) reports that only ~40% of ischaemic stroke patients arrive at hospital within the 4.5-hour window for IV thrombolysis, highlighting the critical role of primary care recognition and rapid transfer.
- Epilepsy and seizures: Approximately 250,000 Australians live with epilepsy (Epilepsy Action Australia). Status epilepticus has an in-hospital mortality of 15–20% and community-onset cases often present first to primary care.
- Meningitis: Bacterial meningitis incidence in Australia is approximately 2–3 per 100,000 per year. Meningococcal disease notifications averaged 700–900 per year pre-COVID; serogroup B and W are now predominant (National Notifiable Diseases Surveillance System).
- Guillain–Barré syndrome (GBS): Incidence 1–2 per 100,000 per year, with significant morbidity requiring ICU admission in up to 30% of cases. Early recognition in primary care is essential as respiratory failure can develop within hours.
- Spinal cord emergencies: Traumatic spinal cord injury affects ~2,000 Australians annually (AIHW). Non-traumatic cord compression from metastatic disease or epidural abscess is an increasingly common presentation in primary care, particularly in patients with known malignancy.
- Aboriginal and Torres Strait Islander populations: First Nations Australians experience stroke at 1.5–3 times the rate of non-Indigenous Australians, at a significantly younger age, and with higher case-fatality rates (AIHW, 2022). Access to stroke units and thrombolysis-capable hospitals remains limited in rural and remote communities.

When to Call an Ambulance
The following clinical scenarios represent neurologic emergencies requiring immediate activation of Triple Zero (000) ambulance services. In each case, the primary care clinician should call 000 personally rather than instructing a patient or carer to do so, to ensure accurate clinical handover to the dispatch centre and responding paramedics.
1. Suspected Acute Stroke
Stroke is the prototypical "time-critical" neurologic emergency. Both ischaemic stroke (eligible for IV thrombolysis within 4.5 hours and endovascular thrombectomy within 24 hours in select cases) and haemorrhagic stroke (requiring urgent neurosurgical assessment) demand rapid hospital transfer.
Recognition — FAST and BE-FAST
The FAST mnemonic remains the standard community screening tool endorsed by the Australian Stroke Foundation. The expanded BE-FAST adds Balance and Eyes to improve sensitivity for posterior circulation strokes, which account for approximately 20% of presentations:
| Letter | Feature | Assessment |
|---|---|---|
| B | Balance | Sudden loss of balance or coordination, ataxia, vertigo |
| E | Eyes | Sudden visual loss, double vision, visual field defect |
| F | Face | Facial droop — ask patient to smile or show teeth |
| A | Arms | Arm drift — ask patient to hold both arms out for 10 seconds |
| S | Speech | Slurred speech or inability to repeat a simple sentence |
| T | Time | Note exact last-known-well time — ask patient, family, bystanders |
Additional Stroke Red Flags Requiring 000 Call
- Sudden severe headache ("thunderclap headache") with focal deficits — consider subarachnoid haemorrhage
- Sudden isolated vertigo with nystagmus and ataxia — posterior circulation stroke
- Sudden confusion, agitation, or reduced consciousness in a patient with new neurologic signs
- Known atrial fibrillation or mechanical heart valve with new neurologic deficit
- Patient on anticoagulants with suspected stroke (document agent, last dose, INR if available)
2. Status Epilepticus
Status epilepticus is defined by the International League Against Epilepsy (ILAE) as a seizure lasting ≥5 minutes OR two or more seizures without recovery of consciousness between them. It is a medical emergency with significant morbidity and mortality if not treated promptly.
Classification
| Type | Definition | Clinical Features | Urgency |
|---|---|---|---|
| Generalised convulsive status epilepticus (GCSE) | Generalised tonic-clonic seizure ≥5 min | Rhythmic limb jerking, cyanosis, incontinence, tongue biting | Immediate 000 |
| Focal status epilepticus | Continuous focal seizure ≥5 min | Rhythmic jerking of one limb or facial muscles, preserved consciousness initially | Immediate 000 |
| Non-convulsive status epilepticus (NCSE) | Prolonged altered consciousness without overt motor activity | Confusion, staring, subtle eye blinking — often misdiagnosed | Urgent 000 if persistent |
When to Call 000
- Any seizure lasting ≥5 minutes in a known epilepsy patient
- First-ever seizure — always requires emergency assessment (exclude structural cause, meningitis, metabolic derangement)
- Seizure in a patient who has not responded to their usual rescue medication (e.g., buccal midazolam)
- Recurrent seizures without return to consciousness between episodes
- Seizure in a pregnant patient (exclude eclampsia — administer IV magnesium sulfate 4 g over 15–20 min if available)
- Seizure associated with head trauma, fever, signs of meningitis, or known immunocompromise
- Post-ictal period lasting >30 minutes without neurological recovery
3. Acute Paraplegia / Spinal Cord Emergency
Acute onset of bilateral lower limb weakness, sensory level, or sphincter dysfunction constitutes a spinal cord emergency. The most common causes encountered in primary care include:
- Spinal cord compression — from metastatic disease (breast, lung, prostate, kidney, thyroid), epidural abscess, or severe disc herniation
- Spinal cord infarction — anterior spinal artery syndrome with acute paraplegia, loss of pain/temperature sensation below the level, and preserved posterior column function
- Transverse myelitis — bilateral motor and sensory deficits with a sensory level, often post-infectious or associated with multiple sclerosis, NMOSD, or MOG-antibody disease
- Cauda equina syndrome — saddle anaesthesia, bilateral sciatica, urinary retention, reduced anal tone
Red Flags in Acute Paraplegia
- Known malignancy with new back pain and bilateral leg weakness
- Sensory level (use pin-prick testing to identify dermatomal level)
- New urinary retention or incontinence with lower limb weakness
- Bilateral positive Babinski sign (upgoing plantars)
- Fever with back pain and progressive weakness (suspect epidural abscess)
- Anticoagulant use with sudden onset back pain and paraplegia (suspect spinal epidural haematoma)
4. Suspected Meningitis / Meningococcal Sepsis
Bacterial meningitis and meningococcal sepsis are rapidly progressive, life-threatening infections. Primary care clinicians may encounter patients in the early stages where the classic triad of fever, neck stiffness, and altered mental status is not yet fully developed.
Clinical Features — High-Suspicion Presentation
- Classic triad (present in ~45% of bacterial meningitis cases): Fever + neck stiffness + altered consciousness
- Early/meningococcal features: Fever with petechial or purpuric rash (non-blanching), leg pain, cold hands and feet, rapid deterioration
- Neonates and infants: Fever, irritability, poor feeding, bulging fontanelle, high-pitched cry, lethargy
- Immunocompromised patients: May present atypically without fever or meningism — maintain high index of suspicion
- Photophobia, severe headache, nausea/vomiting, Kernig's sign, Brudzinski's sign
Pre-Hospital Antibiotic Administration
If bacterial meningitis or meningococcal sepsis is suspected and hospital transfer will take >30 minutes, administer pre-hospital antibiotics in primary care. Do not delay transfer for antibiotic administration if the ambulance is imminently arriving.
5. Rapidly Progressive Weakness — Guillain–Barré Syndrome and Acute Neuromuscular Emergencies
Rapidly progressive weakness — ascending, descending, or generalised — may indicate Guillain–Barré syndrome (GBS), myasthenic crisis, or acute inflammatory myopathy. These conditions can progress to respiratory failure within hours to days.
Guillain–Barré Syndrome (GBS)
- Typically presents 1–4 weeks after a preceding infection (most commonly Campylobacter jejuni gastroenteritis, respiratory tract infection, or Zika virus)
- Symmetrical ascending weakness starting in the legs, with areflexia
- May have paraesthesia, back pain, and autonomic dysfunction (tachycardia, hypertension, urinary retention)
- Respiratory involvement: monitor vital capacity — bedside forced vital capacity (FVC) <20 mL/kg or rapid decline is an indication for ICU transfer
- Facial weakness (bilateral), bulbar weakness (dysphagia, dysarthria), and ophthalmoplegia may occur
Myasthenic Crisis
- Exacerbation of myasthenia gravis with respiratory failure or need for intubation
- Often precipitated by infection, medication changes (aminoglycosides, beta-blockers, magnesium), surgery, or non-adherence
- Progressive bulbar weakness (difficulty swallowing, choking), ptosis, diplopia, and proximal limb weakness
- Any myasthenia patient with new dyspnoea, difficulty managing secretions, or inability to swallow medications warrants 000 transfer
When to Call 000 for Progressive Weakness
- Bilateral leg weakness developing over hours to days, especially with areflexia
- Difficulty breathing, unable to speak in full sentences, shallow breathing, or using accessory muscles
- Inability to swallow, choking on saliva or fluids
- Rapidly worsening weakness in a patient with known myasthenia gravis
- New bilateral weakness with bladder or bowel dysfunction
- Suspected botulism (descending paralysis, bulbar palsy, blurred vision after ingestion of home-canned food)
Stabilisation Prior to Transfer
Once a neurologic emergency has been recognised and 000 activated, the primary care clinician must initiate stabilisation measures using the structured ABCDE approach. The goal is to prevent secondary brain or spinal cord injury and maintain organ perfusion until paramedics arrive and during transfer.
A — Airway
- Assess: Is the patient speaking? Are there gurgling sounds, snoring, or stridor? Is there pooling of secretions?
- GCS <9: The patient cannot protect their own airway — place in the recovery position (lateral decubitus), head tilted slightly down to allow secretions to drain
- Seizure patients: Maintain airway by jaw thrust; place in recovery position once convulsions cease; do NOT insert any object into the mouth
- Bulbar weakness (GBS, myasthenic crisis): Sit upright if able; if unable to manage secretions, position to prevent aspiration; suction if available
- Cervical spine precautions: If trauma suspected (particularly in seizures with fall, or acute paraplegia with trauma), maintain manual in-line stabilisation until paramedics apply a collar
B — Breathing
- Assess respiratory rate, depth, pattern, and SpO₂: Target SpO₂ ≥94% (or ≥88–92% in known COPD with chronic hypercapnia)
- Supplemental oxygen: Apply high-flow oxygen (15 L/min via non-rebreather mask) if SpO₂ <94% or signs of respiratory distress. In suspected stroke, avoid hyperoxia — titrate to SpO₂ 94–98% once established
- Respiratory pattern assessment:
| Pattern | Significance | Action |
|---|---|---|
| Cheyne–Stokes (crescendo–decrescendo with apnoeic pauses) | Bilateral cerebral hemispheric or diencephalic dysfunction; heart failure | Elevate head of bed 30°; document and communicate |
| Central neurogenic hyperventilation | Brainstem lesion | Urgent — anticipate intubation |
| Ataxic / Biot's breathing (irregular with prolonged pauses) | Medullary compression — pre-terminal sign | Immediate 000 if not already en route; prepare for bag-valve-mask |
| Paradoxical breathing (abdomen moves in on inspiration) | Diaphragmatic weakness — GBS, high cervical cord lesion, myasthenic crisis | ICU-level transfer required |
C — Circulation
- Establish IV access: Insert a large-bore (18G or 16G) peripheral IV cannula. Obtain bloods simultaneously (FBC, UEC, LFTs, coagulation, BSL, VBG or ABG, lactate, troponin if cardiac cause considered)
- IV fluid: Commence 0.9% sodium chloride at a keep-vein-open rate (e.g., 80–100 mL/hr) unless signs of fluid overload. Avoid hypotonic solutions (risk of cerebral oedema)
- Blood pressure management — disease-specific:
| Scenario | BP Target | Notes |
|---|---|---|
| Ischaemic stroke (pre-thrombolysis) | <185/110 mmHg for alteplase eligibility | Managed by receiving stroke team — do NOT lower in GP |
| Ischaemic stroke (no thrombolysis planned) | Permissive hypertension; treat if >220/120 mmHg | Permissive hypertension maintains penumbral perfusion |
| Intracerebral haemorrhage | <140 mmHg systolic (INTERACT2/ATACH-2 targets) | Managed at hospital — but avoid excessive BP in primary care |
| Subarachnoid haemorrhage | <160 mmHg systolic | Urgent neurosurgical transfer |
| Spinal cord compression | MAP ≥85 mmHg | Maintain perfusion to the injured cord; IV fluids ± vasopressors at hospital |
| Meningococcal sepsis | Support with IV fluids; fluid bolus 20 mL/kg NS for children | Vasopressors initiated by paramedics / ED |
D — Disability (Neurologic Assessment)
Perform a focused neurologic assessment and document findings for handover. This assessment serves as the baseline against which deterioration or improvement is measured.
Glasgow Coma Scale (GCS)
| Component | Response | Score |
|---|---|---|
| Eye opening (E) | Spontaneous | 4 |
| To voice | 3 | |
| To pain | 2 | |
| None | 1 | |
| Verbal (V) | Oriented | 5 |
| Confused | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 | |
| Motor (M) | Obeys commands | 6 |
| Localises pain | 5 | |
| Withdrawal (flexion) | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Extension (decerebrate) | 2 | |
| None | 1 |
Focused Neurologic Examination Prior to Transfer
- Pupils: Size, symmetry, reactivity to light — unequal or fixed pupils suggest herniation
- Limb strength: Medical Research Council (MRC) grading 0–5 in all four limbs; document any asymmetry
- Reflexes: Present, absent, or exaggerated; Babinski sign (upgoing plantars = upper motor neuron)
- Sensation: Light touch, pin-prick — identify any sensory level in suspected cord pathology
- Cerebellar signs: Finger–nose test, heel–shin test, rapid alternating movements
- Cranial nerves: Brief assessment of II–XII (visual fields, eye movements, facial symmetry, tongue protrusion, palatal movement, shoulder shrug)
Blood Glucose Level (BSL) — Critical Step
E — Exposure and Environment
- Fully expose the patient (within privacy and dignity) to identify rash (petechiae in meningococcal sepsis), injuries from falls during seizures, or skin changes
- Maintain normothermia — use blankets to prevent hypothermia; hyperthermia >38.5°C in status epilepticus may indicate superimposed infection and should prompt consideration of meningitis
- Check for medical alert bracelet, identification necklace, or phone ICE (In Case of Emergency) contacts
- Document weight estimation (for drug dosing) if possible
Seizure-Specific Stabilisation — Benzodiazepine Administration
If a patient is actively seizing in the primary care setting, first-line benzodiazepines should be administered before ambulance arrival. The route depends on availability and clinical setting:
Communication with the Receiving Team
Effective communication between primary care and the receiving emergency department or specialist team is critical for timely and appropriate management. Use the ISBAR framework (endorsed by the Australian Commission on Safety and Quality in Health Care):
Essential Information to Document and Communicate
- Exact last-known-well time (stroke) or seizure onset time
- All vital signs with times (HR, BP, RR, SpO₂, temperature, GCS, BSL)
- Medications given (drug, dose, route, time)
- Current medications — especially anticoagulants (agent, dose, last dose taken, INR if known), anticonvulsants, antihypertensives, and insulin
- Allergies
- Relevant medical history (AF, prosthetic heart valve, malignancy, epilepsy, myasthenia gravis, recent surgery)
- Trend of neurologic observations (improving, stable, or deteriorating)
- Contact details for next of kin or substitute decision-maker
Specific Stabilisation Measures by Emergency Type
| Emergency | Specific GP Measures | Do NOT Do |
|---|---|---|
| Ischaemic stroke | NBM (nil by mouth); position head at 30°; record last-known-well time; note anticoagulant use | Do NOT give aspirin pre-hospital; do NOT lower BP acutely; do NOT give IV fluids rapidly (risk of cerebral oedema) |
| Intracerebral haemorrhage | Elevate head 30°; NBM; correct coagulopathy information for receiving team | Do NOT administer antiplatelet agents or anticoagulants; do NOT lower BP aggressively in GP |
| Status epilepticus | Buccal midazolam or IM midazolam; recovery position; BSL; oxygen if SpO₂ <94% | Do NOT insert objects in mouth; do NOT restrain forcefully; do NOT give oral medications during seizure |
| Meningitis | IM benzylpenicillin 2.4 g (adult) or ceftriaxone 2 g; IV access; fluid resuscitation | Do NOT delay transfer for LP; do NOT use corticosteroids in primary care |
| Spinal cord compression | IV access; maintain MAP ≥85 mmHg with fluids; document sensory level and motor grade | Do NOT allow patient to mobilise; do NOT delay for MRI in GP |
| GBS / Myasthenic crisis | Sit upright; bedside FVC if possible; NBM if bulbar weakness; IV access | Do NOT administer aminoglycosides or magnesium if myasthenia suspected; do NOT leave patient unattended if respiratory compromise |
Investigations in Primary Care (Pre-Transfer)
Investigations in the primary care setting should be limited to those that are immediately available and will directly influence pre-hospital management or ambulance destination. Do NOT delay transfer for investigations that can be performed at the receiving hospital. The primary role of primary care is recognition, stabilisation, and initiation of time-critical treatments.
Risk Stratification & Transport Destination
In metropolitan areas, paramedics will generally transport to the nearest stroke-capable or major tertiary hospital. However, in regional and rural Australia, the primary care clinician may need to advise on transport destination. The following stratification guides decision-making:
Monitoring During Pre-Transfer Period
Continuous monitoring from the time of recognition until handover to paramedics is essential. Document all observations with times to enable trending and informed decision-making by the receiving team.
Key Monitoring Parameters
| Parameter | Frequency | Deterioration Triggers |
|---|---|---|
| GCS | Every 5–15 min | Drop of ≥2 points; new unilateral pupil dilation |
| Respiratory rate and SpO₂ | Continuous / every 5 min | RR <10 or >30; SpO₂ <92%; paradoxical breathing |
| Blood pressure | Every 5–10 min | Systolic <90 mmHg (hypoperfusion); SBP >220 (hypertensive emergency) |
| Heart rate | Continuous (ECG if available) | New AF; HR <50 or >150; new arrhythmia |
| BSL | At presentation; repeat if GCS drops | BSL <4.0 or >15 mmol/L |
| Temperature | At presentation; repeat every 15 min | Temperature >38.5°C (consider meningitis); hyperthermia in status epilepticus |
| Pupils | Every 10 min | New anisocoria; fixed dilated pupil (herniation) |
| Motor response | Every 10 min | New weakness; posturing (decorticate/decerebrate) |
| Seizure duration | Continuous timing | Seizure >5 min (→ give benzodiazepine); continuous after 2nd dose (→ 000 priority escalation) |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Stroke Foundation. Clinical Guidelines for Stroke Management 2022. Melbourne: Stroke Foundation; 2022. Available from: informme.org.au
- 2. Australian Institute of Health and Welfare (AIHW). Stroke and its management in Australia: an update. AIHW Cat. No. CVD 87. Canberra: AIHW; 2023.
- 3. Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3–23.
- 4. Royal Australian College of General Practitioners (RACGP). Emergency medicine and the general practitioner. RACGP Position Statement. Melbourne: RACGP; 2020.
- 5. Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke (INTERACT2). N Engl J Med. 2013;368(10):893–903.
- 6. van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 2016;22(Suppl 3):S37–S62.
- 7. Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat Rev Neurol. 2019;15(11):671–683.
- 8. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021. Standard 6: Communicating for Safety.
- 9. National Health and Medical Research Council (NHMRC). Australian Clinical Guidelines for Acute Stroke Management. Canberra: NHMRC; 2019.
- 10. Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int J Stroke. 2022;17(1):18–29.
- 11. Epilepsy Action Australia. National Epilepsy Management Guidelines. Sydney: Epilepsy Action Australia; 2023. Available from: epilepsy.org.au
- 12. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Detailed Analyses. Canberra: AIHW; 2022.
- 13. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines. Stroke. 2019;50(12):e344–e418.
- 14. National Notifiable Diseases Surveillance System (NNDSS). Communicable Diseases Intelligence: Meningococcal Disease Surveillance Reports. Canberra: Department of Health and Aged Care; 2023.