📋 Key Information Summary
- Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a complex, multi-system neuroimmune condition affecting an estimated 250,000 Australians, with a peak onset between ages 20–45 years.
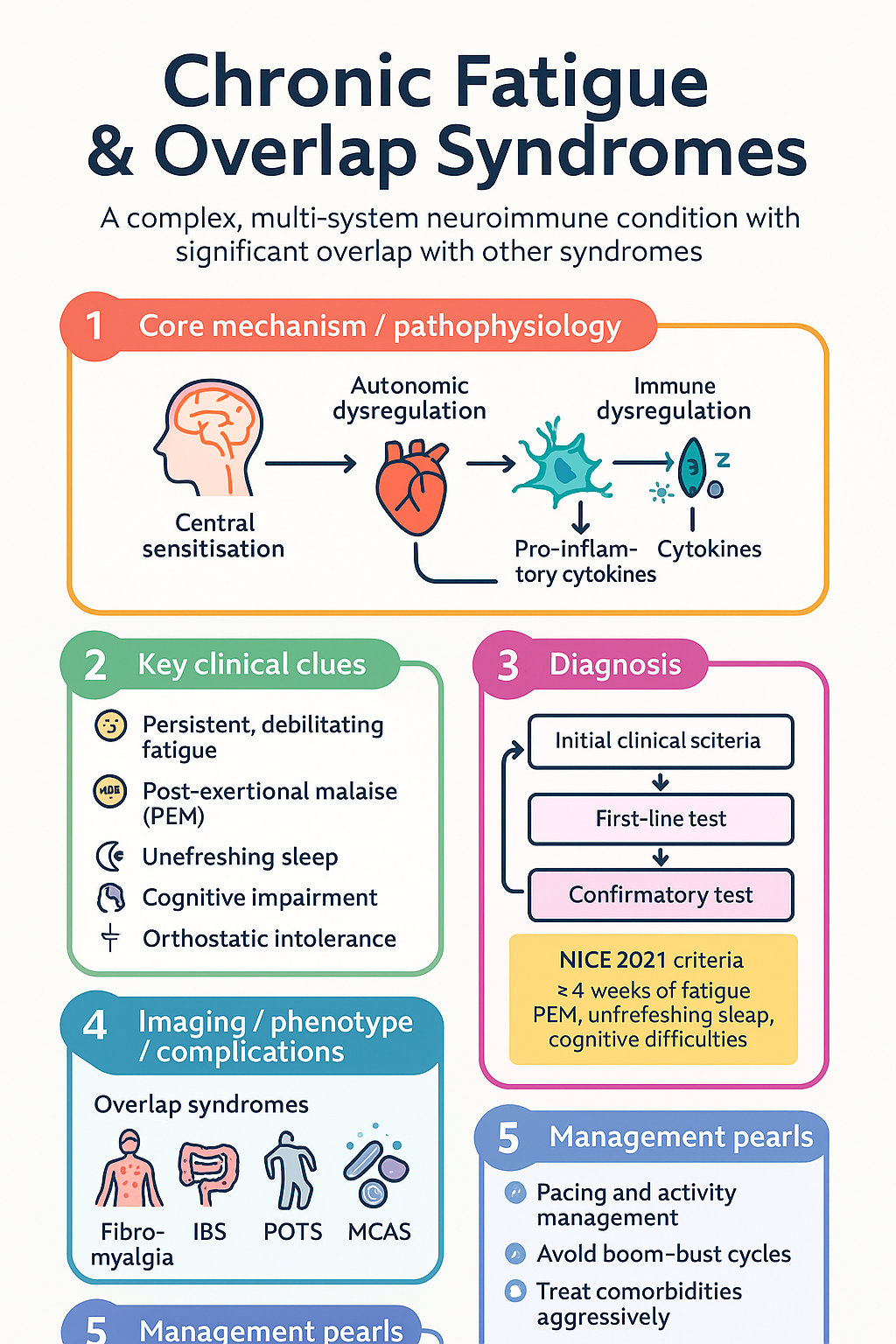
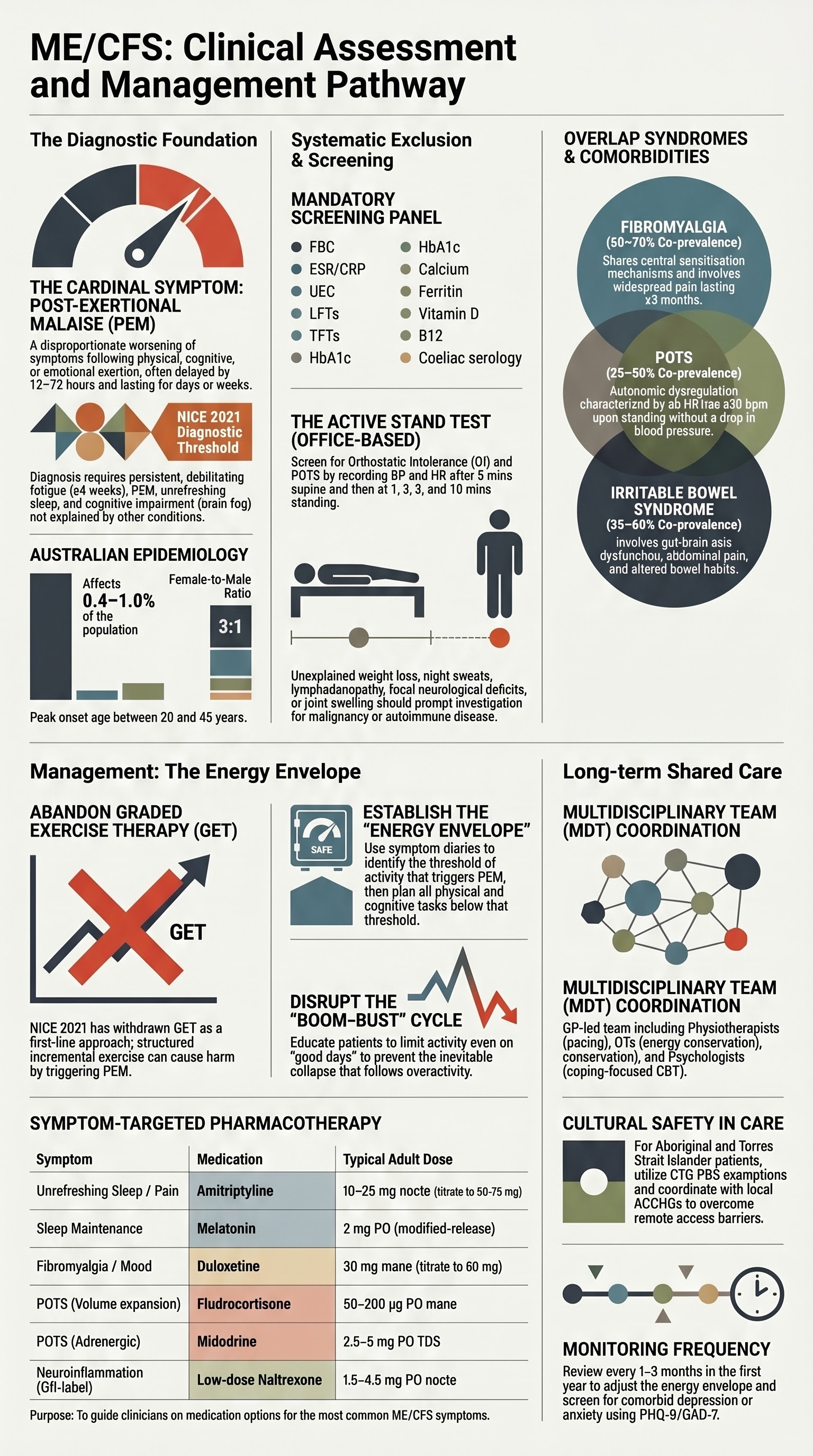
- Diagnosis is clinical — based on the 2021 NICE criteria or 2015 IOM criteria — and requires ≥4 weeks of persistent, debilitating fatigue not explained by another medical condition, plus post-exertional malaise (PEM), unrefreshing sleep, and cognitive impairment.
- A structured fatigue assessment must systematically exclude anaemia, hypothyroidism, diabetes, coeliac disease, sleep apnoea, cardiac failure, adrenal insufficiency, and psychiatric disorders (major depression, anxiety) before a diagnosis of ME/CFS is made.
- Screen for orthostatic intolerance and autonomic dysfunction using active stand test or tilt-table; postural orthostatic tachycardia syndrome (POTS) co-occurs in 25–50% of ME/CFS patients.
- Routine bloods should include FBC, ESR/CRP, UEC, LFTs, TFTs, glucose/HbA1c, calcium, ferritin, vitamin D, B12, folate, coeliac serology (anti-tTG), and urinalysis.
- There is no single curative pharmacotherapy; management centres on pacing and activity management within the patient's energy envelope, avoiding boom–bust cycles.
- Graded exercise therapy (GET) as previously recommended has been withdrawn by NICE 2021 as a first-line approach; pacing-based strategies are now preferred. Exercise, if introduced, must be at a level that does not trigger PEM.
- CBT may help patients adjust to living with a chronic illness and manage comorbid anxiety/depression but is not a treatment for ME/CFS itself.
- Treat comorbidities aggressively — sleep disturbance (melatonin, amitriptyline), orthostatic intolerance (fludrocortisone, midodrine), pain (low-dose amitriptyline, duloxetine), and mood disorders (SSRIs, psychological therapy).
- Aboriginal and Torres Strait Islander Australians face barriers including limited specialist access in remote areas, culturally inappropriate service models, and higher rates of undiagnosed comorbidities; culturally safe, community-led approaches are essential.
- Overlap syndromes include fibromyalgia, irritable bowel syndrome, POTS, mast cell activation syndrome, and functional neurological disorder — many patients meet criteria for multiple conditions simultaneously.
- A multidisciplinary team (GP, physiotherapist, occupational therapist, psychologist, dietitian) with a shared care plan and regular review is the cornerstone of long-term management.
Introduction & Australian Epidemiology
Chronic fatigue syndrome (CFS), now most commonly referred to as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), is a chronic, debilitating, multi-system illness characterised by profound fatigue lasting ≥6 months (≥4 weeks per NICE 2021 for earlier diagnosis), post-exertional malaise (PEM), unrefreshing sleep, and cognitive difficulties ("brain fog"). It is classified by the World Health Organization as a neurological disorder (ICD-10 G93.3).
The condition overlaps significantly with other functional somatic syndromes including fibromyalgia, irritable bowel syndrome (IBS), temporomandibular joint disorder, interstitial cystitis, and functional neurological disorder (FND). These overlap syndromes share common pathophysiological mechanisms including central sensitisation, autonomic dysregulation, and neuroinflammation.
Australian Burden of Disease
- Prevalence: Estimated 0.4–1.0% of the Australian population, equating to approximately 100,000–250,000 affected individuals (AIHW, 2023 estimates).
- Sex distribution: Female-to-male ratio approximately 3:1, though male cases may be underreported.
- Age of onset: Peak incidence 20–45 years; can occur in children and adolescents (estimated prevalence 0.1–0.5% in paediatric populations).
- Post-COVID overlap: An estimated 10–20% of Long COVID patients meet criteria for ME/CFS, substantially increasing case numbers since 2020.
- Economic impact: Significant — estimated annual cost per patient of AUD $16,000–$25,000 including lost productivity, healthcare utilisation, and informal care costs (Jason et al.; Australian ME/CFS data).
- Severity spectrum: Approximately 25% are housebound or bedbound; the majority have moderate illness with significant functional impairment affecting work, education, and social participation.
Assessment of Fatigue
The assessment of persistent fatigue requires a systematic, thorough approach to exclude treatable medical, psychiatric, and sleep-related causes before arriving at a diagnosis of ME/CFS. A structured history, targeted examination, and rational investigation panel are essential.
Clinical History — Key Domains
- Character of fatigue: Onset (acute vs gradual), duration (≥6 months for ME/CFS), pattern (waxing/waning, relation to activity), severity and functional impact.
- Post-exertional malaise (PEM): Cardinal feature of ME/CFS — disproportionate worsening of symptoms following physical, cognitive, or emotional exertion, often delayed by 12–72 hours and lasting days to weeks.
- Sleep: Unrefreshing sleep despite adequate duration; hypersomnia or insomnia; sleep quality vs quantity mismatch.
- Cognitive dysfunction: Difficulty concentrating, word-finding problems, slowed processing, short-term memory impairment.
- Orthostatic symptoms: Dizziness, lightheadedness, palpitations on standing; pre-syncope or syncope.
- Pain: Myalgia, arthralgia, headache (often new type or severity), widespread pain suggesting fibromyalgia overlap.
- Infectious onset: Up to 70% of ME/CFS cases report an acute infectious trigger; document timing and nature.
- Functional capacity: Use the Bell Disability Scale (0–100) or the ME/CFS Symptom Severity Questionnaire; document impact on work, education, ADLs.
- Medication review: Fatigue as an adverse effect (beta-blockers, opioids, antihistamines, gabapentinoids, antihypertensives).
- Psychiatric screen: PHQ-9 (depression), GAD-7 (anxiety) — note that comorbid mood disorders are common and should be treated, but their presence does not exclude ME/CFS.
- Social history: Occupational impact, relationship changes, loss of income, social isolation.
Physical Examination
- Vital signs including lying and standing blood pressure and heart rate (active stand test — check at 1, 3, 5, and 10 minutes).
- General examination: lymphadenopathy, hepatosplenomegaly, thyroid enlargement, signs of anaemia.
- Cardiovascular: murmurs, signs of heart failure.
- Neurological examination: rule out focal deficits (would prompt further investigation for alternative diagnoses).
- Musculoskeletal: tender points (fibromyalgia), joint swelling.
- Mental health assessment: affect, cognition, suicidal ideation screening.
Medical Causes to Exclude
| Category | Condition | Key Investigation | Red Flags |
|---|---|---|---|
| Haematological | Iron deficiency anaemia, B12/folate deficiency, haematological malignancy | FBC, ferritin, iron studies, B12, folate, film | Pallor, lymphadenopathy, unexplained weight loss, night sweats |
| Endocrine | Hypothyroidism, type 2 diabetes, adrenal insufficiency, Cushing syndrome | TSH, fT4, HbA1c, morning cortisol (± short Synacthen test) | Weight change, heat/cold intolerance, polyuria/polydipsia, postural hypotension |
| Autoimmune | Coeliac disease, SLE, rheumatoid arthritis, Sjögren syndrome | Anti-tTG IgA (coeliac), ANA, ESR/CRP (if indicated) | Diarrhoea, weight loss, joint swelling, rash, sicca symptoms |
| Sleep disorders | Obstructive sleep apnoea, restless legs syndrome, narcolepsy | Epworth Sleepiness Scale; polysomnography referral if indicated | Snoring, witnessed apnoeas, excessive daytime sleepiness, cataplexy |
| Cardiac | Heart failure, valvular disease | ECG, echocardiography (if clinical suspicion) | Exertional dyspnoea, orthopnoea, peripheral oedema |
| Neurological | Multiple sclerosis, myasthenia gravis | MRI brain/spine, nerve conduction (if focal signs) | Focal weakness, visual changes, Uhthoff phenomenon |
| Infectious | HIV, hepatitis B/C, chronic infection | HIV Ab, hepatitis serology (if risk factors) | Risk behaviours, persistent fevers, weight loss |
| Respiratory | COPD, interstitial lung disease | Spirometry, CXR (if indicated) | Smoking history, chronic cough, exertional breathlessness |
| Malignancy | Occult malignancy (especially haematological, GI, lung) | Age-appropriate screening; targeted imaging if red flags | Unexplained weight loss, night sweats, new pain, changing bowel habit |
First-Line Investigations — Screening Panel
Autonomic Dysfunction Assessment
Orthostatic intolerance (OI) and postural orthostatic tachycardia syndrome (POTS) are increasingly recognised as common comorbidities in ME/CFS, present in 25–50% of patients. Routine screening is recommended.
Active Stand Test (Office-Based)
- Patient lies supine for ≥5 minutes; record baseline BP and HR.
- Patient stands; record BP and HR at 1, 3, 5, and 10 minutes.
- Orthostatic hypotension: Drop in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing.
- POTS: Rise in HR ≥30 bpm (≥40 bpm in adolescents) within 10 minutes of standing, without orthostatic hypotension, with symptoms of OI.
- Document symptoms during standing: lightheadedness, palpitations, tremor, visual disturbance, nausea, pre-syncope.
Psychiatric Comorbidity Screening
Comorbid depression and anxiety are common (prevalence 30–50%) and should be screened for systematically using validated tools:
- PHQ-9 (Patient Health Questionnaire-9) for depression — score ≥10 warrants further evaluation and treatment.
- GAD-7 (Generalised Anxiety Disorder-7) for anxiety — score ≥10 warrants further evaluation and treatment.
- K10 (Kessler Psychological Distress Scale) — Australian tool, widely used in primary care.
- Suicidal ideation screening should be routine — patients with ME/CFS have an elevated suicide risk due to chronicity, functional loss, and historical medical disbelief.
Diagnostic Criteria
| Criteria | Core Requirements | Key Features |
|---|---|---|
| NICE 2021 | Debilitating fatigue ≥4 weeks; PEM; unrefreshing sleep; cognitive difficulties | Lower threshold for symptom duration; emphasises PEM as cardinal feature; opposes GET |
| IOM 2015 | ≥6 months; substantial reduction in activity; PEM; unrefreshing sleep; cognitive impairment or orthostatic intolerance | Renamed "systemic exertion intolerance disease" (SEID) — less widely adopted term |
| Canadian Consensus 2003 | ≥6 months; PEM; sleep dysfunction; pain; neurological/cognitive manifestations; autonomic, neuroendocrine, immune manifestations (≥2 required) | More comprehensive; captures multi-system involvement |
Overlap Syndromes
ME/CFS rarely exists in isolation. Many patients meet criteria for multiple overlapping conditions, which share pathophysiological mechanisms including central sensitisation, autonomic dysfunction, neuroinflammation, and immune dysregulation. Recognising and addressing overlap syndromes is critical for comprehensive care.
| Overlap Syndrome | Estimated Co-prevalence with ME/CFS | Key Features | Shared Mechanism |
|---|---|---|---|
| Fibromyalgia | 50–70% | Widespread pain ≥3 months, tenderness, fatigue, cognitive dysfunction | Central sensitisation, altered pain processing |
| Irritable bowel syndrome (IBS) | 35–60% | Abdominal pain, altered bowel habit, bloating | Gut-brain axis dysfunction, visceral hypersensitivity |
| POTS / Orthostatic intolerance | 25–50% | Tachycardia on standing, dizziness, palpitations, exercise intolerance | Autonomic dysregulation, hypovolaemia |
| Mast cell activation syndrome (MCAS) | 10–30% (estimated) | Flushing, urticaria, GI symptoms, anaphylaxis-like episodes | Mast cell mediator release, immune dysregulation |
| Ehlers-Danlos syndrome — hypermobility type (hEDS) | 10–20% | Joint hypermobility, chronic pain, skin elasticity, POTS | Connective tissue disorder, autonomic dysfunction |
| Functional neurological disorder (FND) | Overlapping population | Motor/sensory symptoms not consistent with neurological disease | Altered brain network function, central sensitisation |
| Temporomandibular joint disorder | 15–25% | Jaw pain, clicking, headache | Central sensitisation, musculoskeletal dysfunction |
Pathophysiology
The pathophysiology of ME/CFS is complex and multi-systemic. No single biomarker has been identified, but converging evidence points to several interrelated mechanisms:
- Immune dysregulation: Chronic low-grade immune activation with elevated pro-inflammatory cytokines (IL-1β, IL-6, TNF-α), impaired NK cell function, and T-cell abnormalities. These changes are more pronounced following exertion.
- Autonomic dysfunction: Sympathetic predominance with impaired parasympathetic tone, manifesting as POTS, orthostatic intolerance, and impaired heart rate variability.
- Neuroinflammation: PET studies demonstrate microglial activation in brain regions associated with fatigue, pain processing, and cognition (e.g., hippocampus, thalamus, amygdala).
- Central sensitisation: Amplified pain signalling and sensory processing abnormalities, shared with fibromyalgia and other functional somatic syndromes.
- Energy metabolism dysfunction: Impaired mitochondrial function, altered fatty acid oxidation, and reduced oxidative phosphorylation, leading to inadequate ATP production under metabolic stress.
- Gut microbiome alterations: Reduced microbial diversity, altered short-chain fatty acid production, and increased gut permeability ("leaky gut"), potentially driving systemic inflammation.
- Genetic predisposition: HLA associations and familial clustering suggest a genetic component, likely interacting with environmental triggers (infection, trauma, stress).
Management Strategies
Management of ME/CFS requires a person-centred, multidisciplinary approach. There is no single curative treatment. Goals include symptom management, preservation and gradual improvement of functional capacity, and quality of life. The approach must be individualised and flexible.
Pacing and Activity Management
Pacing is the cornerstone of ME/CFS management. It involves understanding the patient's energy envelope — the total amount of physical, cognitive, and emotional activity they can undertake without triggering PEM — and planning activities within that envelope.
CBT-Based Approaches
Cognitive behavioural therapy (CBT) in ME/CFS should be used as a supportive, coping-focused intervention — not as a curative therapy. It helps patients:
- Develop realistic illness beliefs (validating the biological basis of ME/CFS while addressing unhelpful catastrophising or avoidance).
- Manage comorbid anxiety and depression.
- Improve sleep hygiene and address cognitive barriers to pacing.
- Adjust to life changes — loss of employment, social roles, and independence.
- Develop problem-solving strategies for managing daily life with fluctuating symptoms.
Pharmacological Management of Symptoms
No medication is specifically approved or PBS-listed for ME/CFS in Australia. Pharmacotherapy targets individual symptoms and comorbidities.
Non-Pharmacological Strategies
- All activity within the energy envelope — below the PEM threshold.
- Gentle movement: stretching, yoga, tai chi, short walks — as tolerated.
- Aquatic therapy in warm water (hydrotherapy) — buoyancy reduces energy cost.
- Heart rate monitoring — stay below the anaerobic threshold (commonly calculated as 55–60% of age-predicted max HR, or personalised via CPET if available).
- Rest and recovery are as important as activity.
- Occupational therapy for activity planning, energy conservation, and adaptive strategies.
- Cognitive aids: lists, reminders, reducing cognitive multitasking.
- "Cognitive pacing" — limiting mentally demanding tasks and interspersing with rest.
- Return-to-work/study plans — graded, flexible, with workplace/school accommodations.
Treating Comorbidities
Multidisciplinary Team Approach
Monitoring
ME/CFS is a fluctuating condition requiring regular, structured monitoring to adjust management plans, detect evolving comorbidities, and maintain therapeutic rapport.
Useful Outcome Measures
- Bell Disability Scale (0–100): Simple self-rated functional capacity. Widely used in ME/CFS research and practice.
- Chalder Fatigue Scale: 11-item questionnaire; validated for fatigue severity in ME/CFS.
- SF-36 (Short Form-36): General health status and quality of life; useful for tracking change over time.
- PHQ-9 / GAD-7: Repeat at each visit if comorbid mood/anxiety disorder is being treated.
- Activity diary: Patient-recorded daily activity, rest, and symptom log — essential for pacing.
Special Populations
Pregnancy
Paediatrics
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Quick Reference — Assessment & Management Pathway
📚 References
- 1. National Institute for Health and Care Excellence (NICE). Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. NICE guideline NG206. London: NICE; October 2021 (updated 2024).
- 2. Institute of Medicine (IOM). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington, DC: The National Academies Press; 2015.
- 3. Carruthers BM, Jain AK, De Meirleir KL, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: clinical working case definition, diagnostic and treatment protocols. J Chronic Fatigue Syndr. 2003;11(1):7–115.
- 4. Emerge Australia. ME/CFS: A guide for healthcare professionals. Melbourne: Emerge Australia; 2023. Available at: emerge.org.au.
- 5. Australian Institute of Health and Welfare (AIHW). Chronic fatigue syndrome: Australian burden of disease study. Canberra: AIHW; 2023.
- 6. Jason LA, Mirin AA. Updating the National Academy of Medicine ME/CFS prevalence and economic impact figures to account for population growth and inflation. Fatigue: Biomedicine, Health & Behavior. 2021;9(1):9–13.
- 7. Sandler CX, Lloyd AR. Chronic fatigue syndrome: progress and possibilities. Med J Aust. 2020;212(9):426–431.
- 8. Bested AC, Marshall LM. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians. Rev Environ Health. 2015;30(4):223–249.
- 9. Davenport TE, Stevens SR, Stevens J, et al. Properties of measurements obtained during cardiopulmonary exercise testing in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Work. 2020;66(2):247–256.
- 10. Bateman L, Bested AC, Bonilla HF, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: essentials of diagnosis and management. Mayo Clin Proc. 2021;96(11):2861–2878.
- 11. Royal Australian College of General Practitioners (RACGP). Management of chronic fatigue syndrome in primary care. Melbourne: RACGP; 2023.
- 12. Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Washington (DC): National Academies Press; 2015.
- 13. Centre for Disease Control and Prevention (CDC). Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Atlanta: CDC; 2024. Available at: cdc.gov/me-cfs.
- 14. Low DA, Vichayanrat E, Iodice V, et al. Exercise hemodynamics in myalgic encephalomyelitis/chronic fatigue syndrome and postural orthostatic tachycardia syndrome. Circulation. 2022;146(7):549–557.
- 15. Close S, Marshall-Gradisnik S, Byrnes J, et al. The economic impacts of myalgic encephalomyelitis/chronic fatigue syndrome in an Australian cohort. Front Public Health. 2020;8:406.