📋 Key Information Summary
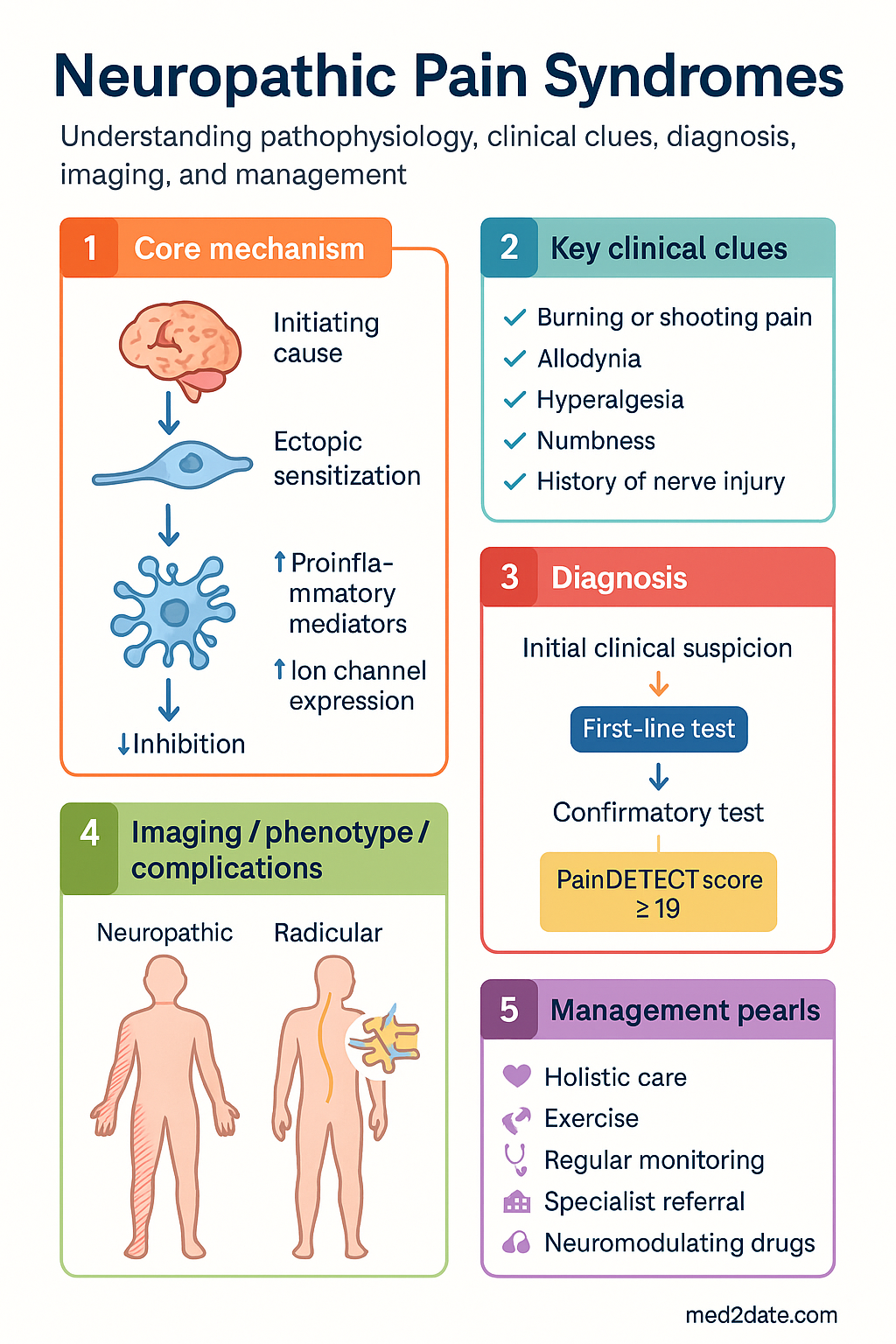
- Neuropathic pain affects 5–8% of Australians and arises from lesion or disease of the somatosensory nervous system; accurate diagnosis is critical because management differs fundamentally from nociceptive pain.
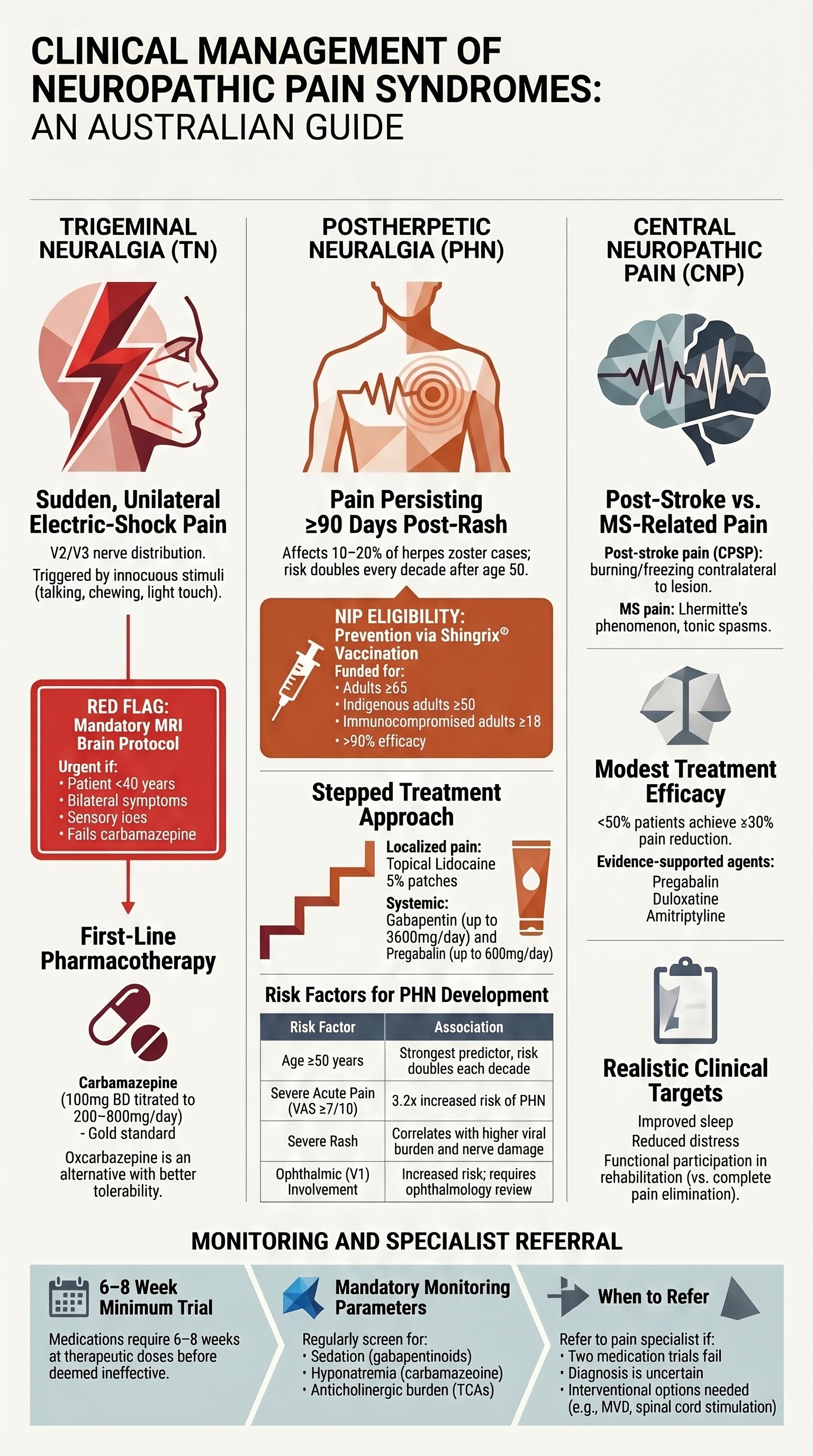
- Trigeminal neuralgia (TN) presents as sudden, severe, unilateral electric-shock-like pain in V2/V3 distribution; carbamazepine 100 mg BD titrated to effect remains first-line therapy with oxcarbazepine as an alternative with better tolerability.
- Red flags in suspected TN — young age (<40 years), bilateral symptoms, sensory loss, or persistent background pain — mandate MRI brain with trigeminal nerve protocol to exclude secondary causes such as multiple sclerosis or posterior fossa tumour.
- Postherpetic neuralgia (PHN) develops in 10–20% of herpes zoster cases over age 50; oral antivirals (valaciclovir or famciclovir) within 72 hours of rash onset and Shingrix® vaccination are the strongest preventive strategies.
- First-line pharmacotherapy for PHN includes gabapentin (titrated to 1800–3600 mg/day in three divided doses), pregabalin (150–600 mg/day in two divided doses), or tricyclic antidepressants (nortriptyline or amitriptyline 10–75 mg nocte).
- Central neuropathic pain after stroke or in multiple sclerosis is under-recognised; pregabalin, duloxetine, and amitriptyline are the most evidence-supported agents, but expectations must be realistic — ≥30% pain reduction in fewer than half of patients.
- Combination therapy (e.g., gabapentinoid + TCA or gabapentinoid + SNRI) should be considered when monotherapy provides inadequate relief after adequate titration.
- Topical lidocaine 5% patches (Lignoderm®) are effective for localised PHN with minimal systemic effects; capsaicin 8% patches (Qutenza®) require application in a specialist or trained-practice setting.
- All patients require monitoring for efficacy (numeric rating scale ≥30% or ≥50% reduction targets) and adverse effects — particularly sedation, dizziness, peripheral oedema (gabapentinoids) and anticholinergic burden (TCAs).
- Aboriginal and Torres Strait Islander Australians face barriers to neuropathic pain management including remote access to specialist services, higher rates of diabetes-related neuropathy, and lower rates of zoster vaccination — culturally safe models of care are essential.
- Referral to a pain medicine specialist or neurologist is indicated when two adequate medication trials have failed, when diagnosis is uncertain, or when interventional options (e.g., microvascular decompression for TN) are being considered.
- Neuromodulation (spinal cord stimulation, occipital nerve stimulation) is reserved for refractory cases and requires specialist assessment; MBS item numbers apply at designated centres.
Introduction & Australian Epidemiology
Neuropathic pain is defined by the International Association for the Study of Pain (IASP) as pain caused by a lesion or disease of the somatosensory nervous system. It encompasses a heterogeneous group of conditions ranging from peripheral nerve injury to central lesions in the brain and spinal cord. In Australia, population-based studies estimate a prevalence of 5–8%, with significant associated morbidity, reduced quality of life, and economic burden exceeding AUD $3.5 billion annually in direct and indirect costs.
The three most clinically significant neuropathic pain syndromes encountered in Australian primary and secondary care are trigeminal neuralgia (TN), postherpetic neuralgia (PHN), and central neuropathic pain (following stroke or in the context of multiple sclerosis). Each syndrome has distinct pathophysiology, diagnostic criteria, and therapeutic pathways, yet they share common principles of pharmacological management and the need for individualised, multidisciplinary care.
This guideline synthesises current Australian (eTG, NPS MedicineWise, RACGP) and international (NICE 2013/updated 2021, EFNS, AAN) recommendations for the diagnosis and management of these three neuropathic pain syndromes in the Australian healthcare context, including PBS availability, MBS-relevant investigations, and culturally safe care for Aboriginal and Torres Strait Islander Australians.
Trigeminal Neuralgia
Clinical Features
Trigeminal neuralgia is characterised by recurrent, unilateral, brief (lasting seconds to 2 minutes), electric-shock-like or lancinating pains in the distribution of one or more divisions of the trigeminal nerve (most commonly V2 and V3). Pain is typically triggered by innocuous stimuli — light touch, talking, chewing, brushing teeth, or exposure to wind — in a trigger zone on the face. Attacks occur in paroxysms that may cluster over hours or days, separated by refractory periods.
Diagnostic criteria (IHS ICHD-3 13.1.1):
- At least three attacks of unilateral facial pain fulfilling criteria B and C
- Pain occurring in one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal distribution
- Pain has at least three of: (a) paroxysmal attacks lasting from a fraction of a second to 2 minutes, (b) severe intensity, (c) electric-shock-like, shooting, stabbing, or sharp quality, (d) precipitated by innocuous stimuli to the affected side
- Not better accounted for by another ICHD-3 diagnosis
Red Flags Suggesting Secondary Causes
- Age of onset <40 years
- Bilateral trigeminal symptoms
- Sensory deficits on examination (decreased pinprick/light touch in trigeminal distribution)
- Persistent aching or burning background pain between paroxysms
- Involvement of the first division (V1) — strongly associated with secondary aetiology
- Associated neurological signs — hearing loss, ataxia, diplopia, facial weakness
- Known history of multiple sclerosis or other CNS disease
- Failure to respond to adequate carbamazepine trial
Carbamazepine / Oxcarbazepine Therapy
Carbamazepine is the only medication with Level A evidence for TN and is recommended as first-line therapy by the AAN, NICE, and eTG. Oxcarbazepine has comparable efficacy with a more favourable side-effect profile and is considered an equivalent first-line option by many experts.
Second-Line & Adjunctive Agents for TN
Interventional Options for Refractory TN
When pharmacotherapy fails or is not tolerated, referral to a neurosurgeon with expertise in trigeminal neuralgia is indicated. Microvascular decompression (MVD) via posterior fossa craniotomy offers the best long-term outcomes (70–80% pain-free at 5 years) for classical TN with neurovascular compression. Percutaneous procedures (balloon compression, radiofrequency thermocoagulation, glycerol rhizolysis) and stereotactic radiosurgery (Gamma Knife) are alternatives for patients unfit for open surgery, with shorter recovery but higher recurrence rates.
Postherpetic Neuralgia
Definition & Risk Factors
Postherpetic neuralgia (PHN) is defined as pain persisting for ≥90 days after the onset of herpes zoster (HZ) rash. It is the most common complication of herpes zoster, affecting 10–20% of all HZ patients and up to 30–50% of those over 70 years of age.
| Risk Factor | Association | Notes |
|---|---|---|
| Age ≥50 years | Strongest predictor; risk doubles each decade after 50 | PHN rare under age 40 |
| Severe acute pain (VAS ≥7/10) | OR 3.2 for developing PHN | Aggressive acute pain management may be protective |
| Severe rash (dermatomal haemorrhagic/vesicular) | OR 2.8 | Greater viral burden correlates with nerve damage |
| Prodromal pain before rash | OR 2.1 | May indicate greater neural involvement |
| Ophthalmic division (V1) involvement | Increased risk | Requires ophthalmology review regardless |
| Immunosuppression | Variable; more severe HZ, but PHN rates uncertain | HIV, transplant, chemotherapy |
| Female sex | OR 1.3–1.5 | Consistent across studies |
| Diabetes mellitus | OR 1.5–2.0 | Synergistic with pre-existing neuropathy |
Prevention: Antivirals & Vaccination
Antiviral Therapy (Acute Herpes Zoster)
Oral antiviral therapy initiated within 72 hours of rash onset reduces viral replication, accelerates healing, and reduces the severity and duration of acute pain. Evidence for PHN prevention is modest but consistent.
Herpes Zoster Vaccination
Shingrix® (recombinant zoster vaccine, adjuvanted — GSK) is the only zoster vaccine funded under the National Immunisation Program (NIP) in Australia since November 2023. It replaced Zostavax® and is recommended for all adults aged ≥65 years (NIP-funded), immunocompromised adults ≥18 years (NIP-funded), and Aboriginal and Torres Strait Islander adults ≥50 years (NIP-funded from February 2025). Two doses are administered intramuscularly, 2–6 months apart (or ≥1 month for immunocompromised individuals).
First-Line Pharmacotherapy for Established PHN
Three medication classes have Level A evidence for PHN: gabapentinoids, tricyclic antidepressants (TCAs), and topical lidocaine. Selection should be individualised based on age, comorbidities, side-effect profile, and patient preference.
Topical Agents for Localised PHN
Stepped Approach to PHN Management
Central Neuropathic Pain
Overview & Aetiologies
Central neuropathic pain (CNP) arises from lesions or disease of the central somatosensory nervous system. The two most common causes in Australian clinical practice are post-stroke pain (central post-stroke pain, CPSP) and pain associated with multiple sclerosis (MS). CNP is under-recognised: prevalence estimates are 8–10% after stroke (typically thalamic) and 25–50% of MS patients report at least one pain syndrome attributable to CNS disease.
Central Post-Stroke Pain (CPSP)
- Typically develops weeks to months after stroke (can be delayed up to 2 years)
- Most commonly associated with thalamic (ventral posterolateral nucleus) or lateral medullary (Wallenberg syndrome) infarction
- Characterised by constant or intermittent burning, aching, tingling, or freezing pain in the contralateral body, often with allodynia and hyperalgesia
- Diagnosis of exclusion — must differentiate from musculoskeletal pain, spasticity-related pain, shoulder subluxation, and complex regional pain syndrome
MS-Related Central Pain
- Often described as burning, band-like, or squeezing sensations; Lhermitte's phenomenon (electric sensation down spine on neck flexion) suggests cervical cord involvement
- Tonic spasms — brief, painful involuntary contractions of a limb, often stereotyped and recurrent
- Trigeminal neuralgia in a young person should always prompt investigation for MS (2–4% of MS patients)
- Pain may coexist with spasticity, fatigue, and depression — requiring holistic management
Drug Options for Central Neuropathic Pain
Evidence for pharmacotherapy in CNP is weaker than for peripheral neuropathic pain. Most recommendations are extrapolated from PHN and painful diabetic neuropathy trials, with fewer dedicated CNP RCTs. Realistic expectations are essential.
Realistic Goals
- Only 30–40% of patients with CNP achieve ≥50% pain reduction with any single agent
- NNT for central pain syndromes ranges from 5–8 (higher than peripheral neuropathic pain)
- Goals should include: improved function, improved sleep, reduced distress, and ability to participate in rehabilitation — not necessarily complete pain elimination
- A ≥30% reduction in pain intensity on the numeric rating scale is considered a meaningful clinical response
- Non-pharmacological strategies (graded motor imagery, mirror therapy, cognitive behavioural therapy, mindfulness-based stress reduction) should be integrated from the outset
Referral When Refractory
Referral to a pain medicine specialist or appropriate subspecialist neurologist should be considered when:
- Two adequate medication trials (at maximum tolerated dose for ≥6–8 weeks each) have failed
- Diagnostic uncertainty exists (e.g., differentiating CPSP from musculoskeletal or spasticity-related pain)
- Significant comorbid psychiatric disease (depression, anxiety, PTSD) requires integrated management
- Interventional neuromodulation is being considered (motor cortex stimulation for CPSP; spinal cord stimulation in selected cases)
- Opioid dependence has developed — requires specialist pain/addiction medicine input
Investigations
Investigations serve three purposes in neuropathic pain: confirming the neuropathic nature of pain, identifying the underlying cause, and excluding treatable secondary aetiologies.
Monitoring
Systematic monitoring is essential for all neuropathic pain treatments. Use a structured approach combining pain intensity scales, functional assessment, and adverse effect screening.
| Parameter | Tool / Method | Frequency | Target |
|---|---|---|---|
| Pain intensity | Numeric Rating Scale (NRS 0–10) | Every visit (minimum 4-weekly during titration) | ≥30% reduction (meaningful); ≥50% reduction (optimal) |
| Functional impact | Patient Global Impression of Change (PGIC); PainDETECT (for neuropathic component) | 8–12 weeks after treatment initiation; then 3–6 monthly | "Much improved" or "Very much improved" on PGIC |
| Sleep quality | Pittsburgh Sleep Quality Index (PSQI) or single-item NRS | Every visit | Improved sleep duration and quality |
| Mood | PHQ-9 (depression); GAD-7 (anxiety) | Baseline, 3 months, then 6-monthly | Screening for comorbid depression/anxiety |
| Adverse effects | Structured questioning; falls risk assessment (elderly) | Every visit | Manage dose-limiting side effects; switch agent if intolerable |
| FBC (carbamazepine) | Full blood count | Baseline, 2 weeks, 4 weeks, then every 3 months for year 1, then every 6 months | WCC >4.0 × 10⁹/L; neutrophils >1.5 × 10⁹/L |
| Sodium (oxcarbazepine, carbamazepine) | Serum sodium | Baseline, 2 weeks, then every 3 months for first year | Na⁺ >130 mmol/L |
| Weight (gabapentinoids) | Weight measurement; BMI calculation | Every visit | Monitor for weight gain >5% of baseline |
| ECG (TCAs) | 12-lead ECG | Baseline (all patients >40 years or cardiac risk factors); repeat if dose >100 mg/day | PR <200 ms; QRS <100 ms; QTc <470 ms (M)/480 ms (F) |
Special Populations
Pregnancy
Paediatrics
Older Adults (>65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience a disproportionate burden of neuropathic pain, driven by higher prevalence of diabetes (3.5 times the non-Indigenous rate), chronic kidney disease, and delayed access to specialist services. Culturally safe, community-based models of care are essential for effective neuropathic pain management.
📚 References
- 1. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101(1):259-301.
- 2. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211.
- 3. Cruccu G, Di Stefano G, Truini A. Trigeminal neuralgia. N Engl J Med. 2020;383(8):754-762.
- 4. Bendtsen L, Zakrzewska JM, Abbott J, et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019;26(6):831-849.
- 5. Cohen JI. Herpes zoster. N Engl J Med. 2013;369(3):255-263.
- 6. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health. Updated 2024. Canberra: Australian Government.
- 7. Dworkin RH, O'Connor AB, Audette J, et al. Recommendations for the pharmacological management of neuropathic pain: an overview and literature update. Mayo Clin Proc. 2010;85(3 Suppl):S3-S14.
- 8. Attal N, Cruccu G, Baron R, et al. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol. 2010;17(9):1113-e88.
- 9. National Institute for Health and Care Excellence (NICE). Neuropathic pain in adults: pharmacological management in non-specialist settings. Clinical guideline [CG173]. Updated 2021. London: NICE.
- 10. Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and management. Lancet Neurol. 2009;8(9):857-868.
- 11. Foley PL, Vesterinen HM, Laird BJ, et al. Prevalence and natural history of pain in adults with multiple sclerosis: systematic review and meta-analysis. Pain. 2013;154(5):632-642.
- 12. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. 2023 report. Canberra: AIHW.
- 13. Wiffen PJ, Derry S, Bell RF, et al. Gabapentin for chronic neuropathic pain in adults. Cochrane Database Syst Rev. 2017;6(6):CD007938.
- 14. Derry S, Rice AS, Cole P, et al. Topical lidocaine for neuropathic pain in adults. Cochrane Database Syst Rev. 2014;(7):CD010958.
- 15. Moore RA, Wiffen PJ, Derry S, et al. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2014;(4):CD007938.
- 16. Faculty of Pain Medicine, Australian and New Zealand College of Anaesthetists (FPM ANZCA). Recommended Definitions and Terminology for Persistent Pain. Melbourne: FPM ANZCA; 2020.