📋 Key Information Summary
- Gait disorders affect approximately 30% of Australians aged ≥65 years and are an independent predictor of falls, disability, hospitalisation, and mortality.
- Every older person presenting with a fall requires a multifactorial risk assessment addressing intrinsic factors (vision, cognition, neuropathy, medication) and extrinsic factors (home hazards, footwear).
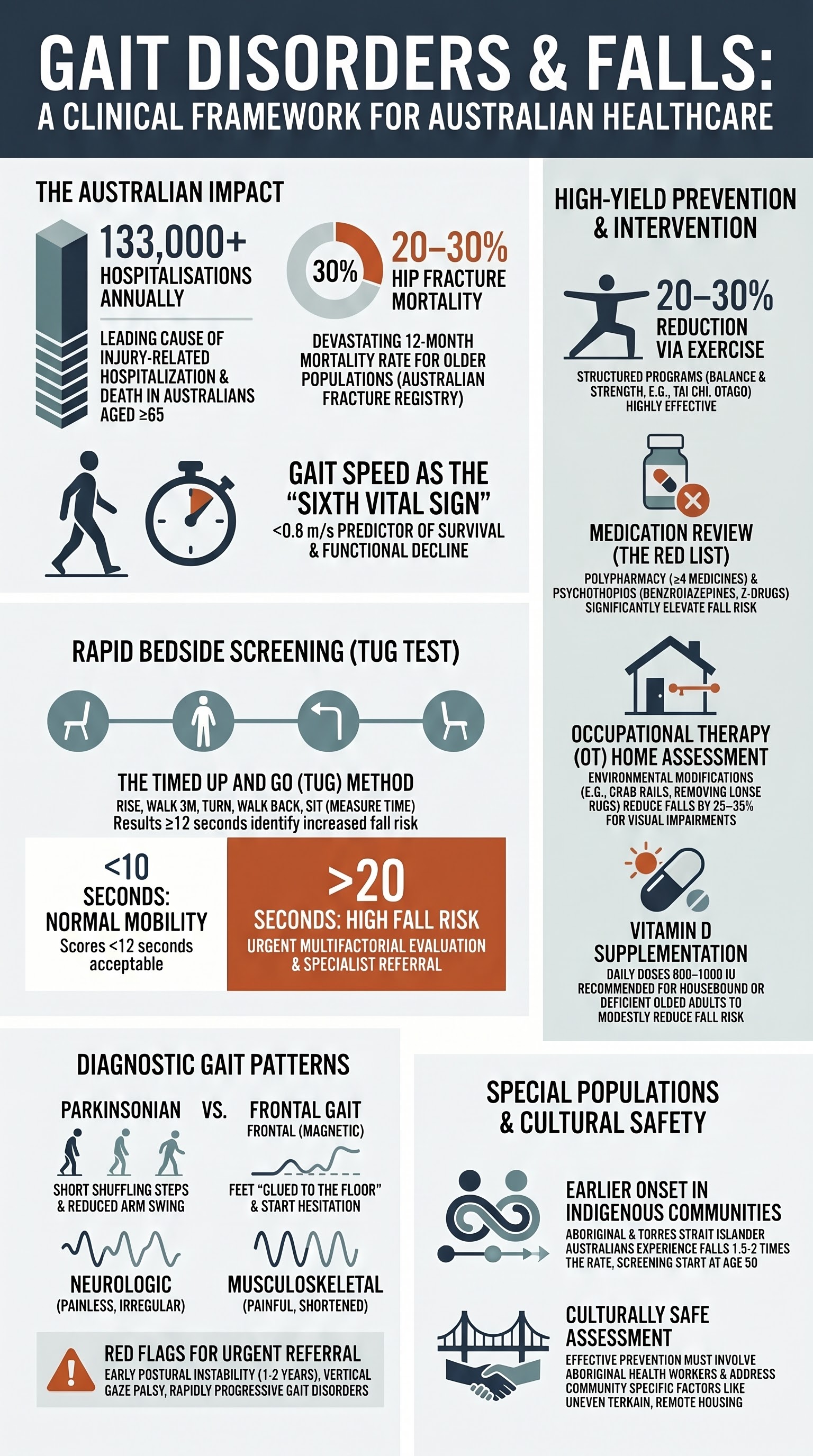
- The Timed Up and Go (TUG) test is a validated bedside screen — a result ≥12 seconds identifies increased fall risk and warrants further evaluation.
- Distinguish neurologic gait (shuffling, festinating, ataxic, magnetic) from musculoskeletal gait (antalgic, Trendelenburg, shortened stride due to joint disease) through structured observation of initiation, stride length, base width, arm swing, turning, and postural stability.
- A parkinsonian gait (short shuffling steps, reduced arm swing, festination, postural instability) mandates urgent neurological referral — early diagnosis of Parkinson's disease enables timely initiation of levodopa and allied health support.
- Frontal gait disorder (magnetic gait, wide base, short steps, start hesitation, freezing) suggests normal pressure hydrocephalus, vascular parkinsonism, or frontal lobe pathology — brain imaging with CT or MRI is essential.
- Medication review is a high-yield falls-prevention intervention — sedatives, antihypertensives (particularly alpha-blockers), anticholinergics, opioids, and polypharmacy (≥4 medicines) significantly increase fall risk.
- Vitamin D supplementation (800–1000 IU daily) is recommended for older adults who are housebound, institutionalised, or have documented deficiency, as it modestly reduces fall risk.
- Structured exercise programs combining balance, strength, and gait training (e.g., Otago Exercise Program, tai chi) reduce falls by 20–30% and should be offered to all at-risk older adults.
- Home hazard assessment by an occupational therapist — removing loose rugs, improving lighting, installing grab rails — reduces falls, especially in those with visual impairment.
- Patients must be counselled on driving restrictions; in most Australian states, a diagnosis of Parkinson's disease or moderate-to-severe gait disorder is notifiable to the driver licensing authority.
- Aboriginal and Torres Strait Islander Australians experience falls at 1.5–2 times the rate of non-Indigenous Australians, with earlier onset and higher rates of hospitalisation — culturally safe assessment and community-based prevention programs are essential.
Introduction & Australian Epidemiology
Gait disorders represent one of the most common and consequential geriatric syndromes encountered in Australian primary care and emergency departments. Normal gait is a complex motor task requiring integrated function of the musculoskeletal system, peripheral and central nervous systems, vestibular apparatus, vision, and cognition. Disruption at any level produces characteristic gait patterns that provide valuable diagnostic clues.
In Australia, falls are the leading cause of injury-related hospitalisation and death in people aged ≥65 years. According to the Australian Institute of Health and Welfare (AIHW), approximately 133,000 older Australians were hospitalised due to falls in 2021–22, with over 5,300 deaths attributable to falls in 2021. The direct healthcare cost exceeds $2.3 billion annually. Hip fractures, the most feared consequence, carry a 12-month mortality of 20–30% in Australian populations.
The prevalence of gait abnormalities increases sharply with age: approximately 10% of community-dwelling adults aged 60–69 have gait impairment, rising to 30–40% in those aged ≥80, and >60% in residential aged care facilities. Gait speed — often called the "sixth vital sign" — is a powerful predictor of survival, hospitalisation, and functional decline. A gait speed <0.8 m/s is associated with increased mortality and disability in Australian cohort studies.
| Statistic | Value | Source |
|---|---|---|
| Annual fall-related hospitalisations (≥65 yrs) | ~133,000 | AIHW 2022 |
| Fall-related deaths (≥65 yrs, 2021) | >5,300 | AIHW 2023 |
| Annual healthcare cost of falls | >$2.3 billion AUD | AIHW 2022 |
| Prevalence of gait disorder ≥80 yrs | 30–40% | Verghese et al. 2006 |
| Hip fracture 12-month mortality | 20–30% | Australian Fracture Registry |
| Proportion of falls with identifiable modifiable risk factors | >75% | RACGP Silver Book 2023 |
Assessment of Gait
A systematic gait assessment is the cornerstone of evaluating any patient presenting with unsteadiness, falls, or mobility complaints. The clinician should observe the patient walking at their normal pace, at a fast pace, and (if safe) on tandem (heel-to-toe) walking. Gait analysis should be integrated with a targeted neurological and musculoskeletal examination.
Structured Gait Observation
Observe the following parameters systematically. Each parameter provides localising and diagnostic information:
| Parameter | Normal | Abnormal Pattern | Significance |
|---|---|---|---|
| Gait initiation | Prompt (<2 seconds) | Start hesitation >3 sec | Parkinsonism, frontal lobe dysfunction |
| Stride length | Symmetrical, age-appropriate | Short shuffling steps | Parkinsonism, frontal gait, musculoskeletal restriction |
| Base width | 5–10 cm between heels | Wide-based (>15 cm) | Cerebellar ataxia, sensory ataxia, vestibular disease |
| Arm swing | Bilateral, symmetric | Reduced or absent unilateral | Parkinsonism (early ipsilateral sign), hemiparesis |
| Cadence | 100–120 steps/min | Festination (accelerating, involuntarily) | Parkinsonism, frontal gait |
| Turning | Fluid, multi-step turn | En bloc (turning as a unit), >3 steps | Parkinsonism, balance impairment |
| Postural stability | Retained on pull test | Retropulsion, inability to recover | Parkinsonism (late), multisensory deficit |
| Floor contact | Heel strike → toe-off | Foot flat, shuffling, no clearance | Parkinsonism, foot drop (L5 radiculopathy, peroneal neuropathy) |
Standardised Gait and Balance Tests
Standardised tests provide objective, reproducible measures that facilitate communication between clinicians, track progression, and guide intervention. The following are recommended in Australian practice:
Distinguishing Neurologic from Musculoskeletal Gait
A critical clinical skill is distinguishing gait disorders arising from neurological pathology (requiring investigation, specialist referral, and disease-specific treatment) from those caused by musculoskeletal problems (requiring orthopaedic/physiotherapy management, analgesia, and joint protection). The table below summarises key distinguishing features:
| Feature | Neurologic Gait | Musculoskeletal Gait |
|---|---|---|
| Stride pattern | Irregular, may include freezing or festination | Regular but shortened on painful side (antalgic) |
| Pain association | Often painless (especially parkinsonian/ataxic) | Directly related to weight-bearing on affected joint |
| Arm swing | Reduced (parkinsonism), absent (hemiparesis) | Preserved or compensatory increased |
| Base width | Wide (ataxia, sensory loss) or narrow (parkinsonism) | Usually normal or slightly widened for stability |
| Trendelenburg sign | May be present (proximal myopathy — neurogenic or myopathic) | Positive in hip OA, gluteal tendinopathy |
| Foot drop | Steppage gait (L5 radiculopathy, peroneal neuropathy, MND) | Uncommon unless post-surgical or severe equinus contracture |
| Response to cueing | Improves with external cues (parkinsonism) or visual input (sensory ataxia) | Not affected by cueing; pain-limited |
| Associated signs | Tremor, rigidity, reflex changes, upgoing plantars, cerebellar signs | Joint swelling/crepitus, reduced ROM, muscle wasting localised to affected joint |
Common Neurologic Gait Patterns
| Gait Type | Key Features | Common Causes |
|---|---|---|
| Parkinsonian | Short shuffling steps, reduced arm swing, festination, en bloc turns, freezing on initiation/doorways | Parkinson's disease, vascular parkinsonism, drug-induced parkinsonism, DLB |
| Cerebellar ataxic | Wide-based, irregular, lurching, difficulty with tandem, truncal instability | Cerebellar stroke/haemorrhage, MS, alcohol-related cerebellar degeneration, SCA |
| Sensory ataxic | Wide-based, heavy foot-stomping, worsens with eyes closed (positive Romberg) | B12 deficiency, diabetic neuropathy, dorsal column lesions, chronic inflammatory demyelinating polyneuropathy (CIDP) |
| Frontal / Magnetic | Short steps, wide base, "magnetic" feet stuck to floor, start hesitation, difficulty lifting feet, poor balance | Normal pressure hydrocephalus, vascular dementia, frontal lobe tumour, progressive supranuclear palsy |
| Spastic (Hemiparetic / Paraparetic) | Circumduction, stiff-legged, scissoring, equinovarus foot posture | Stroke, MS, spinal cord compression, hereditary spastic paraplegia |
| Steppage | High-stepping to clear foot, slapping foot down | Foot drop: common peroneal neuropathy, L5 radiculopathy, peripheral neuropathy, MND |
| Psychogenic | Variable, inconsistent, excessive slowness, knee buckling, distractibility | Functional neurological disorder; diagnosis of exclusion |
Falls in Older Adults
Falls in older adults are rarely due to a single cause. The RACGP's Guidelines for Preventive Activities in General Practice (Red Book) and the Australasian Journal of Ageing consensus statements recommend a comprehensive, multifactorial approach to falls risk assessment and prevention. In Australia, the NHMRC-endorsed best practice is to screen all community-dwelling adults aged ≥65 (≥50 for Aboriginal and Torres Strait Islander people) for falls annually.
Multifactorial Falls Risk Assessment
The following domains must be systematically evaluated in every older person presenting with a fall or identified as at risk:
High-Risk Medications and Falls
Medication-related falls are among the most modifiable risk factors. The following medication classes carry the highest fall risk in Australian older adults:
| Drug Class | Examples | Mechanism of Increased Risk | Action |
|---|---|---|---|
| Benzodiazepines / Z-drugs | Diazepam, temazepam, zolpidem | Sedation, impaired cognition, reduced reaction time, ataxia | Gradual taper per RACGP deprescribing guidelines; avoid abrupt cessation |
| Antihypertensives | Prazosin, doxazosin, frusemide, amlodipine | Orthostatic hypotension, volume depletion | Review targets (relax BP targets in frail elderly ≥80 yrs); check lying/standing BP |
| Antidepressants | Sertraline, amitriptyline, mirtazapine | SSRIs: orthostasis, hyponatraemia; TCAs: anticholinergic, sedation, QTc | Minimise dose; consider non-pharmacological approaches; avoid TCAs |
| Opioids | Oxycodone, tramadol, codeine, tapentadol | Sedation, dizziness, constipation, cognitive impairment | Multimodal analgesia; paracetamol first-line; wean opioids |
| Antipsychotics | Quetiapine, risperidone | Extrapyramidal symptoms, sedation, orthostasis, QTc | Review indication; deprescribe if used for behavioural symptoms of dementia without clear indication |
| Anticholinergics | Oxybutynin, hyoscine, promethazine | Confusion, blurred vision, urinary retention, constipation | Calculate anticholinergic burden score; substitute non-anticholinergic alternatives |
Evidence-Based Falls Prevention Interventions
| Intervention | Effect Size | Key Details | Australian Access |
|---|---|---|---|
| Exercise (balance + strength) | 20–30% fall reduction (RR 0.76) | ≥2 hrs/week; must include challenging balance training. Otago program, tai chi, group exercise classes | Otago funded via CHSP; physiotherapy via Medicare CDM items (10958–10970); community falls prevention programs in most PHNs |
| Home modification | 25–35% fall reduction in those with visual impairment | OT home assessment: grab rails, lighting, remove trip hazards, handrails on stairs | CHSP / state HACC programmes; OT via Medicare CDM items; My Aged Care referral for >65 yrs |
| Medication review | 15–25% fall reduction | Reduce/withdraw psychotropics, minimise polypharmacy, medication review via GP or pharmacist (RMMR/HMR) | PBS-funded Home Medicines Review (HMR, MBS item 900); Residential Medication Management Review (RMMR) |
| Vitamin D supplementation | Modest (~10–15% in deficient/institutionalised) | 800–1000 IU cholecalciferol daily; recommended for housebound, residential care, or documented deficiency | PBS Authority Required for cholecalciferol in CKD or documented deficiency; OTC available cheaply |
| Vision correction | Variable; cataract surgery reduces falls ~30% | Annual eye examination; avoid multifocal glasses during walking; cataract surgery if visually significant | Medicare-funded optometry; cataract surgery via public/private hospitals |
| Footwear advice | Supportive evidence, less quantified | Low-heel, firm-fitting, slip-resistant soles; podiatry referral for foot pathology | Podiatry via Medicare CDM items; CHSP for >65 yrs |
| Cardiac pacing (if indicated) | Significant fall reduction in carotid sinus hypersensitivity | Carotid sinus massage under monitoring; pacemaker if cardioinhibitory response with symptoms | Cardiology referral; MBS-funded procedure |
Vitamin D Supplementation
Parkinsonian & Frontal Gait
Parkinsonian and frontal gait disorders are among the most disabling and therapeutically impactful gait disturbances. They reflect dysfunction of the basal ganglia-thalamo-cortical circuits and frontal lobe motor planning areas, respectively. Early recognition and appropriate referral can substantially improve quality of life and slow functional decline.
Parkinsonian Gait — Clinical Features
The hallmark features of parkinsonian gait result from the combination of bradykinesia, rigidity, and postural instability that characterise basal ganglia dysfunction:
- Festination: Involuntary acceleration of gait with progressively shortening steps — the patient's centre of gravity moves forward faster than their feet can keep up, increasing fall risk
- Freezing of gait (FOG): Sudden, transient inability to initiate or continue stepping — most troublesome on initiation ("start hesitation"), when approaching doorways or obstacles, and during turns. May be "on" phenomenon (wearing-off related) or independent of levodopa cycle
- Reduced arm swing: Often the earliest visible sign; typically asymmetric, preceding the onset of lower limb involvement
- Shuffling gait: Short stride length with reduced foot clearance, increasing trip risk
- En bloc turning: Loss of segmental rotation; the head, trunk, and pelvis turn as a single unit, requiring multiple small steps
- Postural instability: Impaired postural reflexes — a pull test showing retropulsion requiring >2 steps to recover indicates Hoehn & Yahr stage ≥3
Frontal Gait Disorder (Gait Apraxia)
Frontal gait disorder, sometimes called "gait apraxia" or "magnetic gait," results from disruption of the frontal-subcortical circuits that mediate motor planning and execution of locomotion. The patient's legs feel "glued to the floor," and the gait is characterised by:
- Magnetic gait: Feet appear stuck to the floor with difficulty initiating stepping despite normal leg strength
- Wide base: Compensatory widening for balance impairment
- Short shuffling steps: Distinct from parkinsonism — often with preserved arm swing
- Start hesitation: May be overcome by visual cueing (stepping over a line or object) or auditory cueing (counting, marching music)
- Difficulty with dual-tasking: Gait deteriorates markedly when walking and talking simultaneously — a key early sign of frontal-subcortical dysfunction
- Urinary urgency/incontinence: Often accompanies gait disorder in normal pressure hydrocephalus (NPH) — the classic Hakim's triad of gait disturbance, cognitive decline, and urinary incontinence
Key Differentials and Investigation Pathway
| Condition | Distinguishing Features | First-Line Investigation | Referral Pathway |
|---|---|---|---|
| Idiopathic Parkinson's Disease | Asymmetric onset, resting tremor, good levodopa response, progressive | DaTSCAN (if diagnostic doubt); MRI to exclude structural cause | Neurology — ideally movement disorder specialist within 6 weeks of suspected diagnosis |
| Normal Pressure Hydrocephalus | Hakim's triad (gait, cognition, continence); "magnetic" gait; ventriculomegaly out of proportion to atrophy | CT/MRI brain (EVANS index >0.3); large-volume lumbar puncture (tap test) with pre/post TUG | Neurosurgery referral if tap test positive (>20% TUG improvement after removal 30–50 mL CSF) |
| Vascular Parkinsonism | Stepwise progression, lower-body predominance ("lower-half parkinsonism"), history of cerebrovascular risk factors, poor levodopa response | MRI brain (white matter hyperintensities, lacunar infarcts) | Neurology + stroke prevention optimisation |
| Progressive Supranuclear Palsy (PSP) | Early falls (within 1–2 years), vertical supranuclear gaze palsy, axial rigidity, retrocollis, pseudobulbar affect | MRI brain (hummingbird sign — midbrain atrophy) | Urgent neurology referral; PSP is a tauopathy with poor prognosis (median survival 6–9 years) |
| Dementia with Lewy Bodies (DLB) | Fluctuating cognition, visual hallucinations, REM sleep behaviour disorder, parkinsonism, neuroleptic sensitivity | DaTSCAN; MRI to exclude vascular/other causes; neuropsychology | Neurology / geriatrics; avoid antipsychotics (severe sensitivity reactions) |
| Drug-Induced Parkinsonism | Symmetric onset, history of dopamine-blocking drugs (metoclopramide, haloperidol, prochlorperazine, risperidone) | Review medication history; withdraw offending agent (may take 3–6 months to resolve) | GP-initiated deprescribing; neurology referral if persistent >6 months after withdrawal |
Referral Timelines
- Suspected Parkinson's disease: Referral to neurology/movement disorder specialist within 6 weeks of clinical suspicion. Early treatment initiation improves quality of life and functional outcomes.
- Atypical features (PSP, MSA, CBD): Urgent referral — within 2 weeks — as these conditions progress more rapidly and require multidisciplinary management.
- Suspected NPH: Referral to neurosurgery via neurology within 4 weeks for tap test and potential VP shunt assessment. Shunting has ~70–80% gait improvement in carefully selected cases.
- Unexplained falls with frontal signs: Urgent CT brain (within 48 hours if in ED) to exclude subdural haematoma, hydrocephalus, or space-occupying lesion.
Driving and Mobility Aids
Driving assessment is a critical responsibility when managing patients with gait disorders. Australian road safety legislation requires clinicians to consider fitness to drive in patients with neurological conditions that may impair driving ability.
Mobility Aids and Assistive Technology
Appropriate mobility aids improve safety, independence, and community participation. The choice must be individualised and regularly reassessed:
| Aid | Indication | Key Considerations |
|---|---|---|
| Walking stick | Mild balance impairment, unilateral weakness | Hold in contralateral hand to affected leg; correct height = wrist crease at greater trochanter |
| Four-wheel walker (4WW) | Moderate balance impairment, bilateral weakness, post-stroke, parkinsonism | NOT recommended for patients with festination (may increase fall risk — patient walks faster than walker); consider glider frames or front-wheeled walkers for parkinsonism |
| Rollator with seat | Fatigue-limiting conditions, long-distance community mobility | Must have reliable hand-brake function; encourage sitting breaks |
| Pick-up walker (non-wheeled) | Significant bilateral weakness requiring maximum stability | Slowest but most stable; requires adequate upper limb strength to lift |
| Laser-line cueing devices | Freezing of gait in Parkinson's disease | Projects a horizontal laser line to step over; evidence for reducing FOG episodes. Available via occupational therapy or Parkinson's Australia |
| Wheelchair / scooter | Severe mobility limitation, falls despite optimal aids | Does not negate need for continued exercise; funded via NDIS (if <65) or My Aged Care (if ≥65) |
Pathophysiology
Human gait is a complex, largely automatic motor programme that requires the integration of multiple neural systems:
Central Pattern Generators
Locomotion is initiated and modulated by central pattern generators (CPGs) in the spinal cord, which produce the rhythmic alternating pattern of leg movements. These CPGs are under the control of supraspinal centres:
- Mesencephalic locomotor region (MLR): Initiates and modulates gait speed; connected to the basal ganglia and cerebellum
- Basal ganglia: The subthalamic locomotor region and substantia nigra pars reticulata modulate gait initiation and automatic stepping via dopaminergic pathways
- Frontal cortex (supplementary motor area, prefrontal cortex): Voluntary gait control, obstacle avoidance, dual-task gait adaptation, and motor planning
- Cerebellum: Coordination, balance, postural adjustments, and gait rhythm; vermis for truncal control, hemispheres for limb coordination
Pathophysiology of Parkinsonian Gait
Dopamine depletion in the substantia nigra pars compacta (exceeding 60–80% before motor symptoms appear) leads to:
- Reduced basal ganglia output via the globus pallidus internus → decreased thalamo-cortical excitation → bradykinesia and hypokinesia of gait
- Impaired scaling of movement amplitude — the automatic "internal cueing" for step length is lost
- Freezing of gait is thought to result from an inability to appropriately switch between locomotion and postural control, particularly when environmental demands change (doorways, turns)
- Non-dopaminergic systems (cholinergic pedunculopontine nucleus, noradrenergic locus coeruleus) contribute to postural instability and freezing, explaining why these features respond poorly to levodopa
Pathophysiology of Frontal Gait Disorder
Disruption of the frontal-subcortical white matter tracts or basal ganglia-frontal connections impairs the motor planning and execution of gait. This may result from:
- Normal pressure hydrocephalus — dilated ventricles compress periventricular white matter tracts carrying corticospinal and fronto-pontine fibres
- Vascular white matter disease — chronic small vessel ischaemia damages the frontal-subcortical circuits (leukoaraiosis)
- Frontal lobe tumours or trauma — direct disruption of supplementary motor area and prefrontal motor planning regions
Clinical Presentation & Diagnostic Criteria
Clinical Presentation by Cause
The clinical presentation of gait disorders varies by underlying aetiology. A thorough history should address onset (acute vs. subacute vs. chronic), progression (stepwise vs. gradual vs. fluctuating), associated symptoms, and functional impact.
| Presentation | Suggestive Cause | Key History Points |
|---|---|---|
| Acute unilateral gait difficulty | Stroke, acute disc prolapse, hip fracture | Sudden onset; neurological deficits (stroke) vs. pain (musculoskeletal) |
| Subacute progressive gait difficulty with falls | Subdural haematoma, NPH, spinal cord compression | Weeks–months progression; anticoagulant use (SDH); back pain (cord compression) |
| Insidious asymmetric tremor + stiffness + shuffling | Parkinson's disease | Often noticed by spouse; micrographia, reduced arm swing, constipation (prodromal) |
| Gait + cognition + continence decline | Normal pressure hydrocephalus | Months–years; ventriculomegaly on prior imaging may be noted |
| Early falls + vertical gaze palsy + rigidity | Progressive supranuclear palsy | Falls within first 1–2 years; personality change; dysphagia |
| Worsening on standing, improves with support | Orthostatic hypotension, vestibular dysfunction | Light-headedness on standing; worse in morning or after meals |
| Fear-avoidance with normal examination | Post-fall syndrome, anxiety, deconditioning | Previous fall event; activity restriction; social withdrawal |
Diagnostic Criteria — Parkinson's Disease (MDS Clinical Criteria 2015)
The Movement Disorder Society (MDS) criteria for Parkinson's disease require:
- Parkinsonism: bradykinesia plus rest tremor and/or rigidity
- At least 2 supportive criteria (clear and dramatic levodopa response, levodopa-induced dyskinesias, rest tremor of a limb, positive olfactory loss or cardiac sympathetic denervation on MIBG scintigraphy)
- No absolute exclusion criteria (cerebellar abnormalities, supranuclear gaze palsy, frontotemporal dementia within 5 years, parkinetic features restricted to lower limbs for >3 years)
- No red flags that must be counterbalanced by supportive criteria (rapid gait impairment, early severe dysphonia, early severe dysarthria, etc.)
Investigations
First-Line Investigations (GP / ED)
Second-Line / Specialist Investigations
Australian MBS Items — Relevant Investigations
| MBS Item | Investigation | Referral Requirement |
|---|---|---|
| 66823 | Carotid sinus massage (head-up tilt table) | Cardiologist |
| 56001 | CT Brain non-contrast | GP or specialist |
| 63001 | MRI Brain | Specialist (GP referral if urgent ED) |
| 61336 | DaTSCAN (Dopamine transporter SPECT) | Specialist (neurologist) |
| 11105 | Lying/standing BP measurement | GP |
Risk Stratification & Severity Scoring
Falls Risk Stratification
Stratifying falls risk guides the intensity and setting of intervention:
Hoehn & Yahr Staging (Parkinson's Disease)
| Stage | Description | Gait & Falls Implications |
|---|---|---|
| 1 | Unilateral involvement only | Minimal gait impact; reduced arm swing may be only sign |
| 1.5 | Unilateral + axial involvement | Early postural awareness; slight gait change |
| 2 | Bilateral without balance impairment | Bilateral bradykinesia; gait slower but no falls |
| 2.5 | Bilateral, mild balance impairment (pull test recovers) | Gait unsteadiness; "pulling back" on recovery |
| 3 | Bilateral, moderate balance impairment (pull test abnormal) | Falls begin at this stage; festination, freezing; still independent in ADLs |
| 4 | Severe disability; still able to walk/stand unassisted | Frequent falls; freezing of gait significant; needs walking aid; ADL assistance required |
| 5 | Wheelchair-bound or bedridden unless assisted | Cannot walk unassisted; high fall risk during transfers |
Empirical & Directed Therapy
Pharmacotherapy — Parkinson's Disease
The following medications are used in the management of parkinsonian gait disorders. All should be initiated by or in consultation with a neurologist or geriatrician with movement disorder expertise.
Freezing of Gait — Non-Pharmacological Strategies
Freezing of gait (FOG) often responds poorly to medication alone. The following cueing strategies are recommended and should be taught by physiotherapists:
- Visual cueing: Step over a line, laser line projected from a device attached to the walking frame or rollator
- Auditory cueing: Rhythmic counting ("1-2-3-STEP"), metronome apps, marching music
- Somatosensory cueing: Weight shift side to side before initiating stepping; rocking motion
- Cognitive strategies: Imagine stepping over an obstacle; consciously lift the foot high
- Environmental modification: Remove clutter, widen doorways, use contrasting colour strips at thresholds
Normal Pressure Hydrocephalus — Treatment
Gait Disorder Due to Orthostatic Hypotension
Monitoring
Monitoring Plan
| Parameter | Frequency | Tool / Method |
|---|---|---|
| Fall frequency and circumstances | Every visit (minimum 3-monthly for high-risk patients) | Patient/carer diary; structured fall history |
| Gait assessment (TUG, gait speed) | Every 3–6 months | TUG test; 4-metre gait speed; Mini-BESTest |
| Medication review | Every 6 months (or after any fall) | GP medication reconciliation; HMR annually (MBS item 900) |
| Blood pressure (lying/standing) | Every visit if on antihypertensives or with autonomic features | Automated sphygmomanometer; active stand protocol |
| Cognitive screening | 6-monthly if parkinsonian gait or frontal signs | MoCA (preferred for mild impairment); MMSE |
| Levodopa response / motor fluctuations | Every 3–6 months (neurology) | MDS-UPDRS Part III; patient motor diary; on/off documentation |
| Vitamin D level | Annually (or 3-monthly if supplementing and deficient) | Serum 25(OH)D; target ≥75 nmol/L |
| Fear of falling / activity restriction | Every 6 months | Falls Efficacy Scale – International (FES-I) |
| Walking aid suitability | After every fall or functional decline | Physiotherapy reassessment |
| Driving fitness | Annually; after any fall with injury; after medication changes | Austroads Assessing Fitness to Drive 2022; formal OT driving assessment if needed |
Special Populations
Paediatrics
Pregnancy
Elderly (≥80 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Royal Australian College of General Practitioners. Guidelines for Preventive Activities in General Practice (Red Book). 9th ed. Melbourne: RACGP; 2016 (updated 2023).
- 2. Australian Institute of Health and Welfare. Falls in Older Australians 2019–20: Hospitalisations and Deaths Among People Aged 65 and Over. AIHW Cat. No. INJ 4. Canberra: AIHW; 2022.
- 3. National Health and Medical Research Council. Preventing Falls and Harm from Falls in Older People: Best Practice Guidelines for Australian Community Care. Canberra: NHMRC; 2009.
- 4. Verghese J, LeValley A, Hall CB, Katz MJ, Ambrose AF, Lipton RB. Epidemiology of gait disorders in community-residing older adults. J Am Geriatr Soc. 2006;54(2):255–261.
- 5. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther. 2000;80(9):896–903.
- 6. Movement Disorder Society. MDS Clinical Diagnostic Criteria for Parkinson's Disease. Mov Disord. 2015;30(12):1591–1601.
- 7. Austroads. Assessing Fitness to Drive: Medical Standards for Licensing and Clinical Management Guidelines — A Resource for Health Professionals in Australia. Sydney: Austroads; 2022.
- 8. Panel on Prevention of Falls in Older Persons, American Geriatrics Society, British Geriatrics Society. Summary of the updated AGS/BGS clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. 2011;59(1):148–157.
- 9. Stroke Foundation (Australia). Clinical Guidelines for Stroke Management. Melbourne: Stroke Foundation; 2022 (updated).
- 10. Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;1(1):CD012424.
- 11. Religa D, Cermakova P, Lundin A, et al. Treatment of normal pressure hydrocephalus — a comprehensive review. J Alzheimers Dis. 2021;84(3):927–942.
- 12. Australian Institute of Health and Welfare. The Health and Welfare of Australia's Aboriginal and Torres Strait Islander Peoples. Canberra: AIHW; 2023.
- 13. Barban F, Annicchiarico R, Pantelopoulos S, et al. Harnessing virtual reality and augmented reality to combat falls in older adults. Ageing Res Rev. 2020;63:101143.
- 14. Menant JC, Weber F, Lo J, et al. Best practice recommendations for the choice of footwear for older adults. J Foot Ankle Res. 2023;16(1):33.
- 15. Galna B, Rochester L, Burn DJ. The impact of motor cognitive interference on gait in people with Parkinson's disease: influence of task complexity and dual-task type. J Parkinsons Dis. 2015;5(2):267–276.