📋 Key Information Summary
- Sleep disorders are highly prevalent in neurologic patients and significantly worsen quality of life, cognitive function, and disease outcomes; always screen for sleep disturbance during neurological consultations.
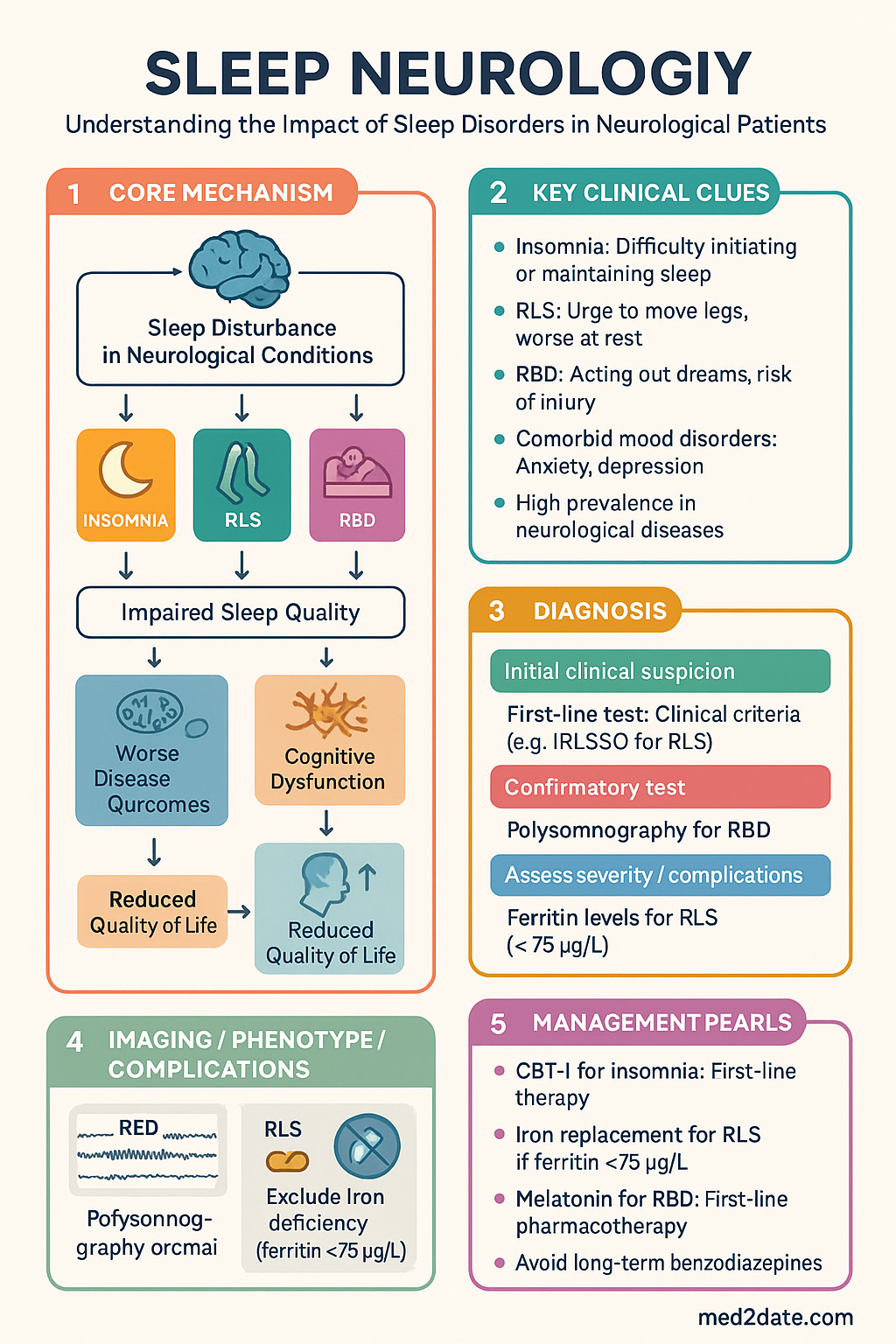
- Insomnia in neurological patients requires CBT-I as first-line therapy; short-term hypnotics (zolpidem, melatonin) may be adjunctive but carry fall and cognitive risks, particularly in the elderly and those with neurodegenerative disease.
- Comorbid mood disorders (anxiety, depression) frequently co-exist with insomnia; address both concurrently to optimise outcomes.
- Restless Legs Syndrome (RLS) diagnosis is clinical using IRLSSG criteria; exclude iron deficiency (ferritin <75 µg/L) and secondary causes before initiating pharmacotherapy.
- First-line RLS pharmacotherapy: iron replacement if ferritin <75 µg/L; then α-2δ ligands (gabapentin enacarbil, pregabalin) preferred over dopamine agonists (pramipexole, ropinirole) to avoid augmentation.
- RLS augmentation (worsening symptoms on dopaminergic therapy) is best managed by switching to an α-2δ ligand, avoiding evening caffeine, and optimising iron stores.
- REM Sleep Behavior Disorder (RBD) is a strong prodromal marker of synucleinopathies (Parkinson disease, dementia with Lewy bodies, MSA); ≥80% conversion over 15 years.
- RBD management centres on bedroom safety measures (padded bed rails, mattress on floor, removing weapons/sharp objects) to prevent self-injury or harm to bed partner.
- RBD pharmacotherapy: immediate-release melatonin 2–12 mg nocte is first-line; clonazepam 0.5–2 mg nocte is second-line with caution for falls, respiratory depression, and cognitive impairment.
- Polysomnography (PSG) is essential for RBD diagnosis (RWA ≥severity) and recommended when sleep-disordered breathing, parasomnias, or diagnostic uncertainty exists in any sleep disorder.
- Serotonergic agents (SSRIs, SNRIs) and some antipsychotics can precipitate or mask RBD; review medications when RBD is suspected.
- Aboriginal and Torres Strait Islander Australians experience higher rates of sleep disorders driven by chronic disease burden; culturally appropriate screening and access to sleep services remain critical gaps.
Introduction & Australian Epidemiology
Sleep disorders are among the most common yet under-recognised comorbidities in neurological practice. Disturbed sleep contributes to accelerated cognitive decline, worsened seizure control, increased falls, reduced rehabilitation gains, and higher mortality across a broad spectrum of neurological conditions including stroke, epilepsy, Parkinson disease, multiple sclerosis, and traumatic brain injury.
In Australia, approximately 33–45% of adults report inadequate sleep quality or duration. Among neurological populations, the prevalence is substantially higher: up to 60% of Parkinson disease patients experience insomnia, 50–70% exhibit RBD symptoms, and 20–30% meet criteria for restless legs syndrome. Following stroke, sleep-disordered breathing affects 50–70% of patients and insomnia is present in 30–50%. Epilepsy patients have a 2–3-fold increased prevalence of insomnia and excessive daytime sleepiness compared with the general population.
The Australian Sleep Health Foundation estimates the economic cost of inadequate sleep at $26.2 billion annually (2016–17 figures), encompassing health system costs, productivity losses, and carer burden. Access to sleep medicine services remains inequitable, with long wait times for public polysomnography (often 3–12 months) and limited specialist availability in regional and remote areas. Telehealth-based sleep medicine and home sleep testing have expanded since the COVID-19 pandemic, improving access for rural Australians.
Insomnia in Neurologic Patients
Definition & Diagnostic Criteria
Insomnia disorder (DSM-5 / ICSD-3) is defined as dissatisfaction with sleep quantity or quality, with difficulty initiating sleep, maintaining sleep, or early-morning awakening, occurring ≥3 nights/week for ≥3 months, causing clinically significant distress or functional impairment, and not better explained by another sleep disorder or coexisting condition.
In neurological patients, insomnia is frequently comorbid with the primary neurological diagnosis and driven by pain, nocturia, medication effects, anxiety/depression, circadian rhythm disruption (particularly in neurodegenerative diseases), and reduced daytime activity.
Sleep Hygiene — Foundation of Management
Sleep hygiene education is a prerequisite for all patients and forms the foundation of CBT-I. Key components include:
- Consistent wake time 7 days/week (±30 minutes), irrespective of sleep onset the previous night
- Bed used only for sleep and sexual activity; remove screens, work materials, and food from the bedroom
- Avoid caffeine after midday and limit total daily caffeine to <400 mg
- Avoid alcohol within 3 hours of bedtime (fragmented sleep architecture)
- Regular daytime exercise, preferably completed ≥4 hours before bedtime
- Limit daytime naps to ≤30 minutes, before 14:00 (with individualisation for narcolepsy/excessive sleepiness)
- Optimise bedroom environment: cool (18–20°C), dark, quiet; use earplugs or white noise if needed
- Blue-light restriction (night-mode devices, amber glasses) in the 2 hours before bed — particularly important in neurodegenerative disease with circadian disruption
Cognitive Behavioural Therapy for Insomnia (CBT-I)
CBT-I is first-line treatment for chronic insomnia in all patients, including those with neurological disease. It comprises cognitive restructuring of maladaptive beliefs about sleep, stimulus control, sleep restriction, relaxation training, and sleep hygiene education. CBT-I typically requires 4–8 sessions delivered by a trained psychologist.
Adaptations for neurological patients:
- In Parkinson disease: shortened sleep restriction protocols, flexible scheduling to accommodate motor fluctuations and nocturnal akinesia
- Post-stroke: address positional factors, nocturia management, spasticity-related awakening
- Epilepsy: avoid excessive sleep deprivation (seizure trigger); moderate sleep restriction titrated carefully
- In cognitively impaired patients: CBT-I adapted for carer-assisted delivery; simplified stimulus control and sleep hygiene components
Pharmacological Management — Cautious Hypnotic Use
Pharmacotherapy should be considered only when CBT-I is insufficient, unavailable, or when acute symptomatic relief is needed while CBT-I is commenced. Long-term hypnotic use is discouraged due to dependence, tolerance, fall risk, cognitive impairment, and rebound insomnia.
Comorbid Mood Disorders
Depression and anxiety are present in 30–50% of neurological patients with insomnia and perpetuate sleep disturbance through rumination, hyperarousal, and maladaptive sleep behaviours. A bidirectional relationship exists: insomnia increases depression risk 2–3-fold, and depression independently disrupts sleep architecture.
- Screen all insomnia patients with the PHQ-9 and GAD-7
- CBT-I is effective for insomnia with comorbid depression and should be prioritised
- SSRIs (sertraline, escitalopram) are preferred when pharmacotherapy for depression is indicated; note that SSRIs can suppress REM sleep and may worsen RBD
- Mirtazapine at low dose (7.5–15 mg) has dual benefit for depression and insomnia
- Tricyclic antidepressants (amitriptyline 10–25 mg nocte) may be useful but carry anticholinergic burden — avoid in dementia, urinary retention, glaucoma
- Refer to GP Mental Health Treatment Plan and psychologist for concurrent CBT-I and mood disorder management
Restless Legs Syndrome (RLS)
Diagnostic Criteria (IRLSSG 2014 — updated)
Diagnosis of RLS is clinical. All five essential criteria must be met:
- An urge to move the legs, usually accompanied by uncomfortable and unpleasant sensations in the legs (sometimes the urge occurs without discomfort; sometimes arms or other body parts are also involved)
- The urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity such as lying or sitting
- The urge to move or unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least for as long as the activity continues
- The urge to move or unpleasant sensations are worse in the evening or night than during the day, or only occur in the evening or night
- The above features are not solely accounted for by another medical or behavioural condition (e.g., myalgia, venous stasis, leg oedema, arthritis, leg cramps, positional discomfort, habitual foot tapping)
Iron Studies & Iron Replacement
Iron deficiency is the most important reversible cause of RLS. All patients require serum ferritin, transferrin saturation (TSAT), iron studies, and full blood count. A ferritin level <75 µg/L (regardless of anaemia) warrants iron replacement; some experts recommend targeting ferritin ≥100 µg/L.
Pharmacological Management — First-Line: α-2δ Ligands
Current international guidelines (AASM 2012, ERLSSG 2018, updated AAN 2023) recommend α-2δ ligands as first-line over dopamine agonists due to lower augmentation risk. Iron replacement is first-line if ferritin <75 µg/L.
Augmentation Management
Augmentation is the most important complication of dopaminergic therapy for RLS, occurring in 6–50% of patients on dopamine agonists over months to years. It is characterised by:
- Earlier onset of symptoms (advancing into the afternoon)
- Increase in symptom intensity
- Spread to previously unaffected body regions (arms, trunk, face)
- Shorter latency to symptom onset with rest
- Decreased duration of effect of the dopaminergic agent
Refractory RLS — Second-Line & Specialist Options
- Low-dose opioids: Oxycodone 2.5–10 mg nocte or tramadol 50–200 mg nocte — reserved for refractory cases with specialist oversight; risk of dependence, respiratory depression
- Clonazepam: 0.5–1 mg nocte — limited evidence; risk of daytime sedation, falls, dependence
- Buprenorphine patch: Emerging evidence for severe refractory RLS; specialist initiation only
- IV iron infusion: Even when ferritin is 75–100 µg/L, IV iron may benefit refractory patients — sleep neurologist referral recommended
REM Sleep Behavior Disorder (RBD)
Definition & Pathophysiology
REM sleep behaviour disorder is a parasomnia characterised by loss of normal REM sleep atonia, resulting in dream-enacting behaviours that may cause self-injury or harm to the bed partner. RBD may be idiopathic or symptomatic (associated with medication use, other sleep disorders, or neurological disease).
Normal REM atonia is mediated by glutamatergic neurons in the sublaterodorsal nucleus (SLD) and glycinergic/GABAergic inhibition of spinal motor neurons. In RBD, dysfunction of the SLD and pontomedullary pathways leads to REM sleep without atonia (RWA). This is most commonly caused by α-synuclein pathology in the brainstem, explaining the strong association with synucleinopathies.
Association with Synucleinopathies
Idiopathic RBD (iRBD) is now recognised as a prodromal synucleinopathy in the vast majority of cases. Longitudinal cohort studies demonstrate:
- 81–90% conversion to a defined synucleinopathy at 14–16 years follow-up (Iranzo et al., Lancet Neurol 2013; Postuma et al., Brain 2019)
- Annual conversion rate approximately 6–8% per year
- Most common eventual diagnoses: Parkinson disease (PD) ~45%, dementia with Lewy bodies (DLB) ~35%, multiple system atrophy (MSA) ~10%
- RBD is classified as a "core feature" in the DLB diagnostic criteria (McKeith et al., 2017) and a supportive biomarker for PD prodromal criteria (MDS, 2015)
Diagnostic Criteria (ICSD-3)
All four criteria must be met:
- Repeated episodes of sleep-related vocalisation and/or complex motor behaviours arising from REM sleep
- These behaviours are documented by PSG as occurring during REM sleep, or based on clinical history, are presumed to occur during REM sleep by the emergence of the abnormal behaviours from sleep
- PSG demonstrates REM sleep without atonia (RWA): sustained or excessive phasic EMG activity in the submentalis or flexor/extensor limb muscles during REM sleep
- The disturbance is not better explained by another sleep disorder, mental disorder, medication, or substance use
Polysomnography findings in RBD:
| PSG Feature | Finding in RBD | Diagnostic Utility |
|---|---|---|
| REM without atonia (RWA) | Excessive phasic or tonic EMG activity in submentalis or limb muscles during REM | Required for diagnosis; scored per SINBAR criteria (phasic density >15.7%) |
| Dream-enacting behaviours | Vocalisations (shouting, swearing, talking), limb jerking, punching, falling out of bed | Highly characteristic; bed partner history essential |
| Sleep fragmentation | Increased arousals, reduced sleep efficiency | Common but non-specific |
| Comorbid OSA | Coexists in 40–50% of RBD patients | Must treat OSA concurrently; CPAP may unmask true RBD |
Medication Review — Iatrogenic RBD
Several medication classes can precipitate or exacerbate RBD:
- SSRIs/SNRIs (sertraline, escitalopram, venlafaxine) — most common cause of iatrogenic RBD; REM suppression effects paradoxically reduce atonia
- Tricyclic antidepressants (amitriptyline, clomipramine)
- MAO-B inhibitors (selegiline, rasagiline) — used in PD; may unmask or worsen RBD
- Beta-blockers (propranolol, metoprolol) — occasional association
- Antipsychotics (can also mimic RBD features through NREM parasomnias)
When RBD is suspected, review and, where clinically safe, reduce or discontinue causative medications. Consult the prescribing specialist (psychiatrist, cardiologist, neurologist) before changes.
Safety Measures
Non-pharmacological safety interventions are the most important component of RBD management and should be implemented for all patients before or alongside pharmacotherapy:
Pharmacological Management of RBD
Pharmacotherapy is indicated for frequent or injurious RBD episodes despite safety measures. Evidence is limited to case series, expert consensus, and small RCTs (no large Phase III trials exist for RBD).
Follow-Up & Longitudinal Monitoring
- 6-monthly clinical review: assess RBD symptom frequency/severity, injury events, medication side effects, and emerging motor/cognitive features
- Annual screening for prodromal synucleinopathy features: olfaction (Sniffin' Sticks or UPSIT), colour vision (Farnsworth D-15), constipation assessment, orthostatic hypotension (lying/standing BP), subtle motor signs (MDS-UPDRS Part III)
- Cognitive screening every 12 months (MoCA); referral for neuropsychological assessment if decline detected
- DAT-SPECT (DaTscan) if parkinsonism suspected — available at major Australian nuclear medicine centres (MBS item 61393); wait times 2–8 weeks in metropolitan areas
- Consider referral to movement disorder/neurodegenerative disease research registries (e.g., Parkinson's cohort studies at Brain and Mind Centre, Florey Institute)

Investigations
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a significantly higher burden of sleep-related morbidity compared to non-Indigenous Australians. Chronic diseases including type 2 diabetes, chronic kidney disease, rheumatic heart disease, and obesity — all highly prevalent in Indigenous communities — are independent risk factors for obstructive sleep apnoea, restless legs syndrome, and insomnia. The AIHW reports that Indigenous Australians are 1.5–2 times more likely to report insufficient sleep, and sleep apnoea prevalence is significantly elevated, particularly in remote communities.
Rheumatic heart disease and subsequent valvular surgery may predispose to central sleep apnoea and disrupted sleep architecture. Chronic kidney disease (CKD stage 4–5) prevalence is up to 4 times higher in Indigenous Australians, directly increasing RLS prevalence. Iron deficiency is more common due to nutritional factors, parasitic infections, and chronic disease.
Culturally safe care requires acknowledging the social determinants of health (overcrowded housing, food insecurity, limited healthcare access, intergenerational trauma) that independently contribute to sleep disturbance. Screening for sleep disorders should be integrated into Indigenous health checks (MBS Item 715) and chronic disease management plans.
📚 References
- 1. Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria. Sleep Med. 2014;15(8):860–873.
- 2. Winkelman JW, Armstrong MJ, Allen RP, et al. Practice guideline summary: Treatment of restless legs syndrome in adults — Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2016;87(24):2585–2593.
- 3. Iranzo A, Tolosa E, Gelpi E, et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: an observational cohort study. Lancet Neurol. 2013;12(5):443–453.
- 4. Postuma RB, Iranzo A, Hu M, et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study. Brain. 2019;142(3):744–759.
- 5. Howell MJ, Schenck CH. Rapid eye movement sleep behavior disorder and neurodegenerative disease. JAMA Neurol. 2015;72(6):707–712.
- 6. Aurora RN, Zak RS, Maganti RK, et al. Best practice guide for the treatment of REM sleep behavior disorder (RBD). J Clin Sleep Med. 2010;6(1):85–95.
- 7. Mitchell UH, Obray JD, Hunsaker E, Garcia BT, Clarke TJ, Hope S. Peripheral dopamine in restless legs syndrome. Front Neurol. 2018;9:155.
- 8. Grigg-Damberger MM, Ralls F. Rapid eye movement sleep behavior disorder in adults with and without neurologic disease. Chest. 2014;145(5):1167–1177.
- 9. Trauer JM, Qian MY, Doyle JS, Rajaratnam SMW, Cunnington D. Cognitive behavioral therapy for chronic insomnia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(3):191–204.
- 10. Australian Institute of Health and Welfare (AIHW). Sleep problems as a risk factor for chronic conditions. Cat. no. PHE 306. Canberra: AIHW; 2022.
- 11. Sleep Health Foundation. Awake to the cost of sleep: Inquiry into sleep health awareness in Australia. Australian Parliamentary Inquiry Submission. Sydney: Sleep Health Foundation; 2019.
- 12. McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017;89(1):88–100.
- 13. Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson's disease. Mov Disord. 2015;30(12):1600–1611.
- 14. Garcia-Borreguero D, Silber MH, Winkelman JW, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation. Sleep Med. 2016;21:1–11.
- 15. McCarter SJ, Boswell CL, St Louis EK, et al. Treatment outcomes in REM sleep behavior disorder. Sleep Med. 2013;14(3):237–242.
- 16. Pamphlett R, Mor D, Hng TM. Restless legs syndrome in Aboriginal Australians: a preliminary study. Aust N Z J Med. 2000;30(4):438–441.