📋 Key Information Summary
- Back pain is the leading cause of disability in Australia, affecting ~4 million Australians annually and costing over $4.8 billion per year (AIHW 2023). Most episodes are mechanical and self-limiting.
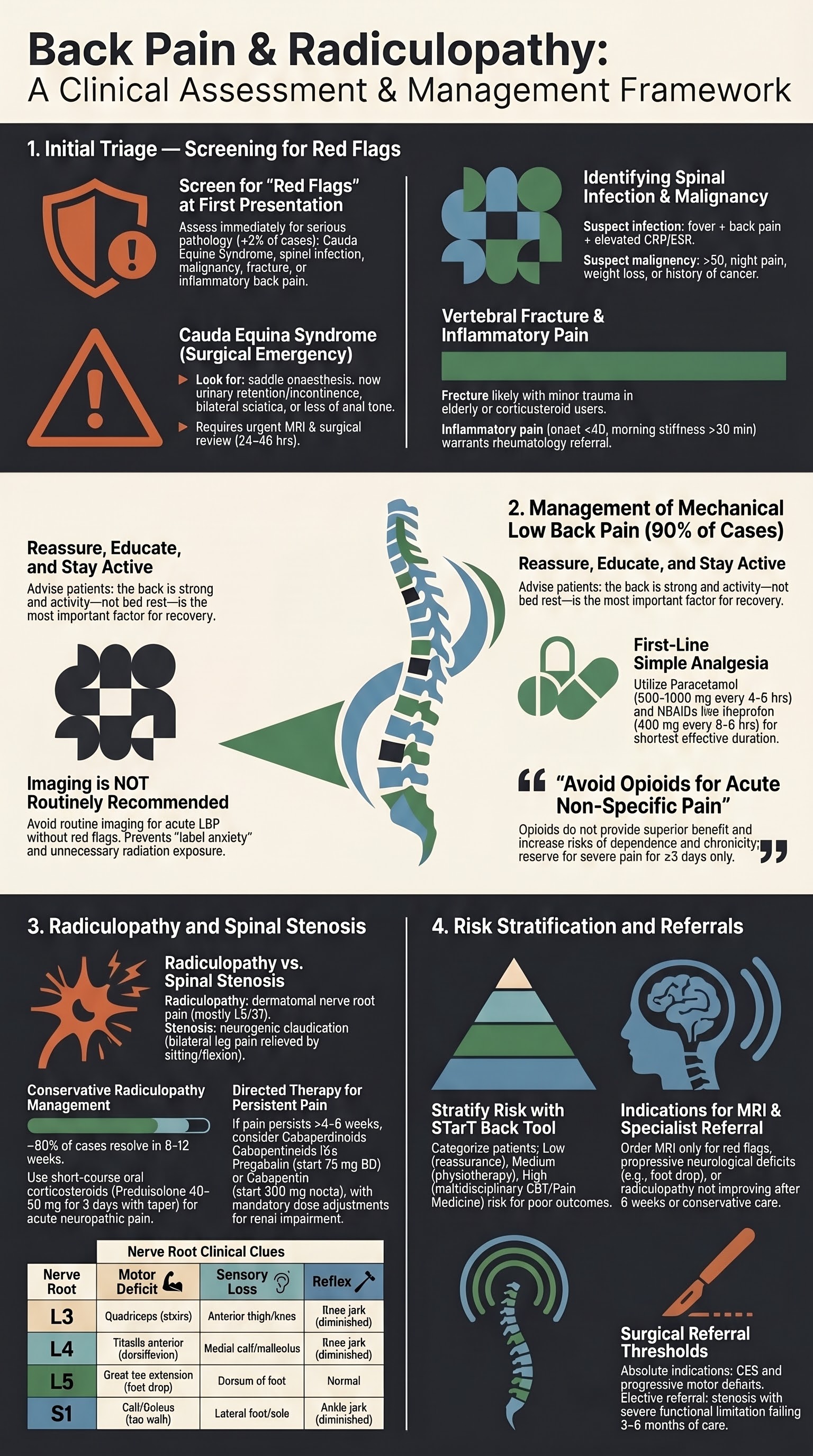
- Red flags must be screened at first presentation: cauda equina syndrome (saddle anaesthesia, urinary retention, bilateral sciatica) requires emergent MRI and surgical review within 24–48 hours.
- Suspect spinal infection in immunocompromised patients, IVDU, or those with fever + back pain + elevated CRP/ESR. Blood cultures and urgent MRI with gadolinium are first-line.
- Spinal malignancy should be considered in patients >50 years with unexplained weight loss, night pain, prior cancer history, or failure to improve after 4–6 weeks.
- Vertebral fracture is likely with minor trauma in the elderly, corticosteroid use, or osteoporosis. Plain X-ray is first-line; CT or MRI if equivocal.
- Inflammatory back pain (morning stiffness >30 min, improves with activity, onset <40 years, night waking) warrants HLA-B27, ESR/CRP, and sacroiliac joint imaging — refer rheumatology.
- Mechanical low back pain: reassure patients, encourage continued activity (avoid bed rest), first-line analgesia with paracetamol ± NSAIDs. Routine imaging is NOT recommended unless red flags or radiculopathy present.
- Imaging indications: red flags, progressive neurological deficit, radiculopathy not improving after 6 weeks, or pre-procedural planning. MRI is preferred for soft-tissue evaluation.
- Radiculopathy presents with dermatomal pain, sensory loss, motor weakness, and diminished reflexes. L5 and S1 nerve roots are most commonly affected.
- Conservative management for radiculopathy (education, activity modification, physiotherapy, short-course oral corticosteroids or gabapentinoids) resolves ~90% of cases within 6–12 weeks.
- Lumbar spinal stenosis causes neurogenic claudication: bilateral buttock/leg pain worsened by extension and walking, relieved by sitting or flexion. MRI confirms diagnosis.
- Refer for interventional or surgical assessment when conservative care fails after 6–12 weeks, there is progressive neurological deficit, cauda equina syndrome, or severe functional limitation.
- Aboriginal and Torres Strait Islander Australians experience higher rates of back pain disability, delayed presentation, reduced access to specialist and allied health services, and poorer pain management outcomes.
Introduction & Australian Epidemiology
Back pain, encompassing low back pain, thoracic pain, and neck pain, is the leading cause of years lived with disability (YLD) in Australia and globally. Radiculopathy — nerve root compression causing radiating limb pain, sensory disturbance, and/or motor weakness — is one of the most common complications of degenerative spinal disease and a frequent reason for specialist referral.
In Australia, the burden is substantial:
- Prevalence: Approximately 4.0 million Australians (16% of the population) report back problems as a chronic condition (AIHW 2023). Lifetime prevalence of low back pain is estimated at 80%.
- Health system impact: Back problems are the 4th leading cause of total disease burden and account for ~$4.8 billion in direct healthcare costs annually, including GP visits, imaging, pharmaceuticals, allied health, and surgery.
- GPs manage ~85% of back pain presentations in primary care. Lumbar radiculopathy accounts for approximately 5–10% of all low back pain presentations.
- Spinal surgery rates in Australia have increased by ~50% over the past two decades, driven by spinal fusion and decompression procedures. Evidence supports surgery only for specific indications (e.g., cauda equina syndrome, progressive deficit, confirmed stenosis with refractory symptoms).
- Imaging overuse: Despite guideline recommendations, approximately 25–30% of patients with simple low back pain in Australian general practice receive imaging within 6 weeks of presentation — a key target for quality improvement under the ACSQHC Lumbar Spinal Conditions Clinical Care Standard.
This guideline covers the systematic assessment of back pain to identify serious pathology ("red flags"), evidence-based management of mechanical low back pain and radiculopathy, and pathways for specialist referral in the Australian context.

Red Flags in Back Pain
Red flag screening is the single most important step in the initial assessment of back pain. The purpose is to identify the small proportion of patients (<2%) with serious underlying pathology — cauda equina syndrome, spinal infection, malignancy, fracture, or inflammatory spondyloarthropathy — requiring urgent investigation and management.
Cauda Equina Syndrome (CES)
CES is a surgical emergency caused by compression of the cauda equina nerve roots, most commonly by a massive lumbar disc herniation, tumour, epidural abscess, or traumatic fracture.
| Feature | Key Findings | Immediate Action |
|---|---|---|
| Urinary symptoms | Retention, overflow incontinence, loss of sensation during voiding | Post-void bladder scan; if residual >200 mL → urgent referral |
| Saddle anaesthesia | Reduced sensation over perineum, buttocks, inner thighs, genitalia | Document dermatomal pattern; urgent MRI |
| Bilateral sciatica | Pain radiating below knees bilaterally — more concerning than unilateral | Urgent MRI lumbar spine |
| Motor deficit | Bilateral foot drop, bilateral ankle/knee weakness, wide-based gait | Urgent MRI; spinal surgical review |
| Anal tone | Reduced or absent anal sphincter contraction on digital rectal examination | Urgent MRI and surgical consultation |
Spinal Infection
Spinal infections include vertebral osteomyelitis, discitis, and epidural abscess. Staphylococcus aureus (including MRSA in healthcare-associated and some community settings) is the most common causative organism. Gram-negative bacilli and Mycobacterium tuberculosis should be considered in immunocompromised, migrant, and Indigenous populations.
Spinal Malignancy
Metastatic disease to the spine is far more common than primary spinal tumours. The most common primaries include lung, breast, prostate, renal, and thyroid cancers, as well as multiple myeloma. Approximately 5–10% of cancer patients develop spinal metastases.
| Red Flag for Malignancy | Significance |
|---|---|
| Age >50 years with first episode of back pain | Higher malignancy prevalence in this age group |
| Unexplained weight loss (>5% body weight in 3 months) | Suggests systemic disease |
| Night pain / pain at rest that wakes from sleep | Inflammatory or neoplastic pain pattern |
| Previous history of cancer | High risk of osseous metastases |
| Failure to improve after 4–6 weeks of appropriate care | Warrants further investigation for occult pathology |
| Thoracic back pain in an older adult | Thoracic pain is less commonly mechanical; higher concern for malignancy or fracture |
Vertebral Fracture
Vertebral fractures may be traumatic or atraumatic (osteoporotic). Risk factors include age >65, osteoporosis (T-score ≤ −2.5), prolonged corticosteroid use (>3 months of ≥5 mg prednisolone daily), minimal trauma (fall from standing height), and history of fragility fracture.
- Clinical suspicion: focal bony tenderness, age >65, recent fall or trauma, corticosteroid use, known osteoporosis
- Initial imaging: plain X-ray (lateral and AP views) — sensitivity ~80% for osteoporotic fractures
- If X-ray equivocal: CT for bony detail or MRI (STIR sequences) to detect occult fracture and bone marrow oedema
- Assess for osteoporosis: request DEXA scan if not recently performed; consider initiating anti-resorptive therapy
Inflammatory Back Pain (Axial Spondyloarthropathy)
Axial spondyloarthropathy (including ankylosing spondylitis and non-radiographic axial SpA) affects predominantly young adults (onset <45 years) and is frequently diagnosed 5–10 years after symptom onset due to delayed recognition. Early identification allows initiation of disease-modifying therapy.
| Feature Suggesting Inflammatory Back Pain | Detail |
|---|---|
| Age of onset <40 years | Most patients present between 20–35 years |
| Insidious onset | Gradual, not linked to specific injury |
| Duration >3 months | Persistent rather than episodic |
| Morning stiffness >30 minutes | Improves with movement and warm showers |
| Improves with exercise, worsens with rest | Opposite pattern to mechanical back pain |
| Night pain — waking in second half of night | Characteristic of inflammatory pain |
| Alternating buttock pain | Sacroiliitis pattern |
Investigations for suspected inflammatory back pain: ESR, CRP, HLA-B27, and plain X-ray of pelvis (AP) with sacroiliac joint views. MRI of the sacroiliac joints (STIR and T1 sequences) is the preferred first-line imaging if available, as it can detect active sacroiliitis before radiographic changes develop. Refer to rheumatology for confirmation and management.
Summary of Red Flags by Category
| Category | Key Red Flag Features | First Investigation | Urgency |
|---|---|---|---|
| Cauda equina | Saddle anaesthesia, urinary retention, bilateral sciatica, reduced anal tone | Urgent MRI | Emergent — within 24 h |
| Infection | Fever, IVDU, immunosuppression, raised CRP/ESR | Blood cultures, CRP/ESR, MRI with gad | Urgent — within 24–48 h |
| Malignancy | Age >50, weight loss, night pain, cancer history | MRI, FBC, ESR/CRP, calcium, PSA (if prostate suspected) | Urgent — within 2 weeks |
| Fracture | Trauma, age >65, corticosteroid use, osteoporosis | Plain X-ray; CT if equivocal | Prompt — within 48 h |
| Inflammatory SpA | Onset <40, morning stiffness >30 min, improves with activity | ESR/CRP, HLA-B27, SIJ MRI | Non-urgent — rheumatology referral |
Mechanical Low Back Pain
Mechanical (non-specific) low back pain accounts for over 90% of presentations. It arises from the lumbar intervertebral discs, facet joints, sacroiliac joints, ligaments, and paraspinal muscles. The exact anatomical source of pain can rarely be identified, and this does not impede effective management.
Clinical Assessment
- History: site, onset, duration, radiation, aggravating/relieving factors, functional impact, psychosocial yellow flags (fear-avoidance beliefs, catastrophising, workplace dissatisfaction, compensation)
- Examination: lumbar range of motion, straight leg raise (SLR), neurological examination of lower limbs (L4–S1 myotomes, dermatomes, reflexes), gait assessment
- Red flag screen: systematically exclude cauda equina, infection, malignancy, fracture, inflammatory pain (see Red Flags section above)
Initial Management Principles
Activity Advice
- Do NOT prescribe bed rest — bed rest beyond 24–48 hours worsens outcomes and increases chronicity
- Encourage gentle, graduated return to normal daily activities and work (even with some discomfort)
- Walking programme: 20–30 minutes daily, progressing as tolerated
- Avoid prolonged sitting (>30 minutes without movement breaks)
- Heat therapy (heat packs, warm showers) provides modest short-term symptom relief
Simple Analgesics
Short-Term Muscle Relaxants (for significant muscle spasm)
Imaging Indications
Routine imaging for acute low back pain (presenting within 6 weeks, no red flags) is not recommended and may cause harm through label anxiety, unnecessary procedures, and radiation exposure.
| Imaging Indication | Preferred Modality | Notes |
|---|---|---|
| Suspected fracture | Plain X-ray (AP + lateral) | CT if X-ray equivocal; MRI for occult fractures |
| Red flags for infection or malignancy | MRI with gadolinium (± contrast) | Highest sensitivity for soft tissue, marrow infiltration, epidural collections |
| Cauda equina syndrome | Urgent MRI | MRI of choice; CT myelography if MRI unavailable |
| Radiculopathy not improving after 6 weeks | MRI lumbar spine | Confirms disc herniation, nerve root compression, stenosis |
| Pre-procedural planning (injection/surgery) | MRI lumbar spine | Required before any interventional procedure |
| Suspected inflammatory sacroiliitis | MRI sacroiliac joints (STIR + T1) | Detects active inflammation before radiographic change |
Common incidental findings on MRI that are NOT necessarily the cause of pain (present in asymptomatic individuals): disc bulges (30–60% of asymptomatic adults), degenerative disc changes (60% over age 40), facet joint arthrosis, Schmorl's nodes, and mild foraminal stenosis. These findings should be interpreted in clinical context and not used to label patients with frightening diagnoses.
Radiculopathy & Lumbar Spinal Stenosis
Lumbar Radiculopathy
Lumbar radiculopathy is caused by compression, inflammation, or ischaemia of a spinal nerve root, most commonly by a disc herniation at L4–L5 or L5–S1. It affects the L5 and S1 nerve roots in approximately 90% of cases. The annual incidence is approximately 3–5% in adults aged 25–55 years.
Clinical Features by Nerve Root
| Nerve Root | Pain Distribution | Motor Deficit | Sensory Loss | Reflex |
|---|---|---|---|---|
| L3 | Anterior thigh to knee | Quadriceps weakness (difficulty climbing stairs) | Anterior thigh / medial knee | Knee jerk diminished |
| L4 | Anterolateral thigh to medial malleolus | Tibialis anterior weakness (foot dorsiflexion) | Medial calf / medial malleolus | Knee jerk diminished |
| L5 | Lateral leg, dorsum of foot, great toe | Extensor hallucis longus / tibialis anterior (foot drop) | Dorsum of foot, first web space | Usually normal |
| S1 | Posterior leg, lateral foot, sole | Gastrocnemius/soleus (difficulty walking on toes, impaired push-off) | Lateral foot, sole, 4th–5th toes | Ankle jerk diminished or absent |
Key clinical tests:
- Straight leg raise (SLR) test: positive when leg elevation to 30–70° reproduces radicular pain below the knee. Sensitivity ~90%, specificity ~30% for L4–S1 disc herniation.
- Crossed SLR: positive when raising the unaffected leg reproduces symptoms in the affected leg. Specificity ~90% — highly suggestive of disc herniation.
- Femoral nerve stretch test (reverse SLR): positive when prone knee flexion reproduces anterior thigh pain — suggests upper lumbar radiculopathy (L2–L4).
Lumbar Spinal Stenosis
Lumbar spinal stenosis (LSS) is narrowing of the spinal canal, lateral recess, or neural foramina, most commonly due to degenerative changes (ligamentum flavum hypertrophy, facet joint arthrosis, disc bulging). It is the most common reason for spinal surgery in patients over 65 years.
| Feature | Neurogenic Claudication (Stenosis) | Vascular Claudication (PAD) |
|---|---|---|
| Pain location | Buttock → thigh → leg (bilateral common) | Calf (usually unilateral initially) |
| Provocation | Walking, standing, lumbar extension | Walking (consistent distance) |
| Relief | Sitting, forward flexion, lying | Standing still |
| Walking distance | Variable; may be better uphill/worse downhill | Reproducible fixed distance |
| Peripheral pulses | Present and normal | Diminished or absent |
| ABPI | Normal (>0.9) | Reduced (<0.9) |
Conservative Management of Radiculopathy & Stenosis
When to Order MRI
- Radiculopathy with progressive or severe neurological deficit (foot drop, significant weakness)
- Radiculopathy not improving after 6 weeks of conservative management
- Suspected cauda equina syndrome (emergent — same-day MRI)
- Suspected spinal infection or malignancy
- Neurogenic claudication consistent with spinal stenosis — MRI confirms diagnosis and guides treatment planning
- Pre-procedural planning for epidural injection or surgery
MRI availability in Australia: MRI lumbar spine is available on Medicare (MBS) for patients referred by a medical practitioner for clinically suspected radiculopathy or spinal stenosis meeting specific criteria. Bulk-billed MRI services are widely available in metropolitan areas but may be limited in rural and remote settings, where CT is the more accessible alternative.
Referral for Interventional Procedures
| Procedure | Indication | Evidence | Access |
|---|---|---|---|
| Epidural corticosteroid injection (transforaminal) | Unilateral radiculopathy with confirmed disc herniation on MRI; conservative care failed 6+ weeks | Short-term relief (4–12 weeks); moderate evidence | Pain specialist, interventional radiologist, or spinal surgeon |
| Epidural corticosteroid injection (interlaminar/caudal) | Bilateral radiculopathy or spinal stenosis with neurogenic claudication | Short-term benefit; weaker evidence for stenosis than radiculopathy | Pain specialist or spinal surgeon |
| Facet joint injection / medial branch block | Suspected facet joint pain (axial pain, extension-provoked, no radiculopathy) | Diagnostic; may guide radiofrequency denervation | Pain specialist, interventional radiologist |
Surgical Referral Indications
- Absolute: cauda equina syndrome (emergent decompression); progressive motor deficit despite conservative care
- Strong indication: radiculopathy with confirmed large disc herniation causing significant motor deficit (e.g., foot drop) — best outcomes with surgery within 6 months
- Elective indication: neurogenic claudication from spinal stenosis with severe functional limitation not responding to 3–6 months of conservative management and/or epidural injections
- Spinal surgery consultation (neurosurgery or orthopaedic spine) should be arranged when surgery is being considered. In Australia, public wait times can be 3–12 months; private referral may be faster.
Surgery for radiculopathy: Microdiscectomy is the most common surgical procedure. Evidence from the SPORT trial and subsequent studies shows that surgery provides faster relief of leg pain compared to conservative management, but differences narrow by 1–2 years. Most patients still recover with conservative management.
Surgery for spinal stenosis: Decompressive laminectomy is the standard procedure. The SPORT trial showed superior outcomes for surgery over conservative care at 2 and 4 years in patients with confirmed stenosis and persistent symptoms. Spinal fusion is reserved for cases with instability or spondylolisthesis.
Pathophysiology
Sources of Back Pain
The lumbar spine is a complex biomechanical structure. Pain may originate from multiple structures, and in most cases of non-specific back pain, the exact source cannot be identified with certainty.
- Intervertebral disc: Annular tears, internal disc disruption, and degenerative disc disease. The nucleus pulposus is avascular and has poor healing capacity. Disc degeneration begins in the second decade of life.
- Facet (zygapophyseal) joints: Arthrosis, synovitis, and capsular irritation. These joints are innervated by the medial branch of the dorsal ramus. Responsible for ~15–30% of chronic low back pain.
- Sacroiliac joints: Dysfunction or inflammation. Accounts for ~15–25% of low back pain. Provocation tests (FABER, compression, distraction) aid diagnosis.
- Paraspinal muscles and ligaments: Muscle strain, myofascial trigger points, and ligamentous sprain — common in acute presentations.
- Spinal nerve roots: Compression or inflammation by disc herniation, osteophytes, or stenosis causes radiculopathy. Biochemical mediators (phospholipase A2, TNF-α, IL-1β, IL-6) released from herniated disc material cause chemical radiculitis independent of mechanical compression.
Disc Herniation & Radiculopathy Mechanism
Disc herniation occurs when nuclear material breaches the annulus fibrosus. The postero-lateral position is most common (where the annulus is thinnest), directing herniation toward the traversing nerve root within the spinal canal or the exiting nerve root within the foramen. The L4–L5 and L5–S1 levels account for ~95% of lumbar disc herniations due to the high biomechanical loads at these segments.
Stenosis Pathophysiology
Spinal stenosis is a progressive condition resulting from degenerative changes that narrow the spinal canal. The pathological cascade includes: (1) disc degeneration and bulging, (2) facet joint hypertrophy and osteophyte formation, (3) ligamentum flavum thickening and buckling, and (4) loss of disc height causing foraminal narrowing. Symptoms are related to posture-dependent compression of neural structures — extension narrows the canal by up to 15%, while flexion increases it.
Investigations
Investigations in back pain are guided by the clinical context — red flag screening, assessment of radiculopathy severity, and pre-procedural planning. Routine laboratory and imaging investigations are not indicated for simple mechanical low back pain.
Laboratory Investigations
Imaging
Electrodiagnostic Studies
Risk Stratification
Risk stratification for chronicity and poor outcome is essential to guide management intensity. The STarT Back Screening Tool (SBST) and assessment of "yellow flags" (psychosocial risk factors) are recommended in Australian guidelines.
STarT Back Screening Tool — Risk Categories
Yellow Flags — Psychosocial Risk Factors for Chronicity
| Domain | Yellow Flag Indicators |
|---|---|
| Beliefs & attitudes | "My spine is damaged"; fear of movement; belief that pain equals harm; expectation that passive treatments are required |
| Emotional state | Depression, anxiety, irritability, catastrophising, low self-efficacy |
| Behavioural | Avoidance of activity, excessive rest, over-reliance on medication, withdrawal from social activities |
| Work-related | Job dissatisfaction, heavy physical demands, unsupportive employer, workplace conflict, pending workers' compensation claim |
| Social | Social isolation, low socioeconomic status, poor family support, compensation/litigation involvement |
Patients with high yellow flag burden benefit most from multidisciplinary pain management programmes combining physical rehabilitation with cognitive-behavioural therapy. In Australia, these are available through public pain management clinics and some private providers, though wait times can be significant (3–12 months in public settings).
Pharmacological Management
Empirical Therapy — Acute Mechanical Low Back Pain
Empirical Therapy — Acute Radiculopathy
Directed Therapy — Neuropathic Pain Component
When radiculopathy persists beyond the acute phase (>4–6 weeks) or neuropathic pain is prominent (burning, shooting, electric, paraesthesiae), gabapentinoids or duloxetine should be considered. These medications target neuropathic pain mechanisms rather than nociceptive inflammation.
Monitoring
Monitoring Plan
Neurological Monitoring in Radiculopathy
- Motor function: test foot dorsiflexion (L4/L5), great toe extension (L5), plantarflexion (S1) at every visit
- Reflexes: knee jerk (L4), ankle jerk (S1) — document changes
- Sensory testing: light touch and pinprick in L4, L5, S1 dermatomes
- Gait assessment: heel walk (L5), toe walk (S1), tandem gait
Pharmacological Monitoring
- NSAIDs: renal function (eGFR) at baseline and after 2 weeks if prolonged use; blood pressure monitoring; GI risk assessment
- Gabapentinoids: renal function before initiation and dose titration; assess for sedation, dizziness, peripheral oedema; monitor for misuse/dependence
- Oral corticosteroids: blood glucose monitoring in diabetics (short course); monitor for GI side effects
- Amitriptyline: ECG before initiation if cardiac history or age >50; monitor for anticholinergic effects
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Back pain is one of the most prevalent chronic conditions among Aboriginal and Torres Strait Islander Australians, contributing significantly to disability and reduced quality of life. The AIHW reports that musculoskeletal conditions (including back pain) are the second leading cause of disease burden for Indigenous Australians. Important considerations include:
📚 References
- 1. Australian Commission on Safety and Quality in Health Care (ACSQHC). Lumbar Spinal Conditions Clinical Care Standard. Sydney: ACSQHC; 2023.
- 2. National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management. NICE guideline [NG59]. London: NICE; 2016 (updated 2020).
- 3. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–747.
- 4. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383.
- 5. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478–491.
- 6. Traeger AC, Henschke N, Hübscher M, et al. Estimating the risk of chronic pain: development and validation of a prognostic model (PICKUP) for patients with acute low back pain. PLoS Med. 2016;13(5):e1002019.
- 7. Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378(9802):1560–1571.
- 8. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA. 2006;296(20):2441–2450.
- 9. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis: four-year results of the Spine Patient Outcomes Research Trial (SPORT). Spine. 2010;35(14):1329–1338.
- 10. Australian Institute of Health and Welfare (AIHW). Back problems. AIHW; 2023. Available from: https://www.aihw.gov.au/reports/chronic-musculoskeletal-conditions/back-problems
- 11. Royal Australian College of General Practitioners (RACGP). Guideline for the management of knee, hip and osteoarthritis. Melbourne: RACGP; 2018 (with musculoskeletal pain sections).
- 12. Stynes S, Konstantinou K, Ogollah R, et al. Clinical diagnostic model for sciatica developed in primary care patients with low back-related leg pain. PLoS One. 2018;13(4):e0191682.
- 13. Chou R, Deyo R, Friedly J, et al. Systemic pharmacologic therapies for low back pain: a systematic review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017;166(7):480–492.
- 14. Lin CWC, Verwoerd AJH, Mahnke AN, et al. How is radiating leg pain defined in clinical trials? A systematic review. Eur Spine J. 2020;29(3):466–478.
- 15. RHDAustralia (Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine — Northern Territory Chapter). NT Antimicrobial Treatment Guidelines — Spinal Infections. Darwin: RHDAustralia; 2023.