📋 Key Information Summary
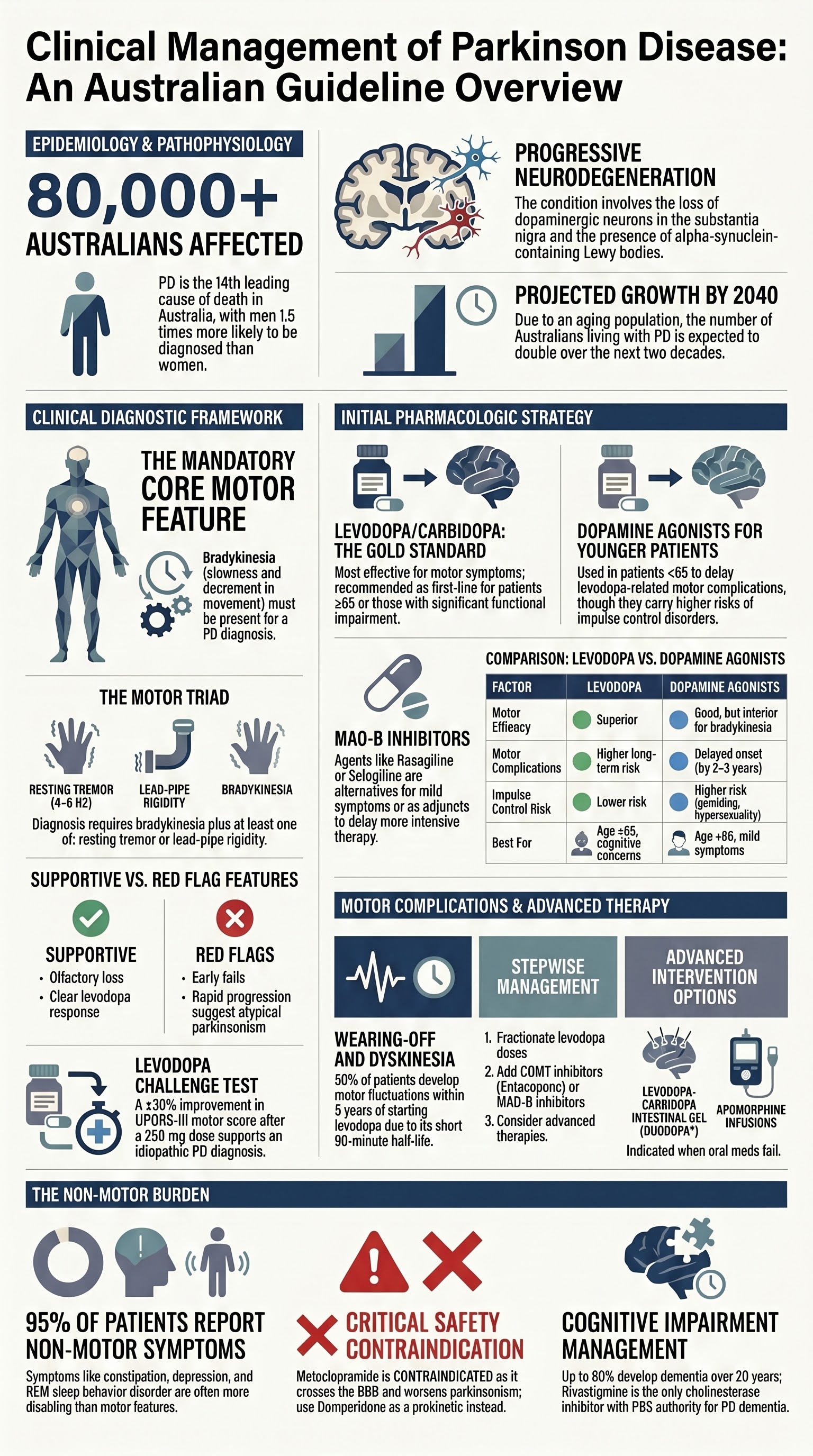
- Parkinson disease (PD) affects approximately 80,000 Australians and is the second most common neurodegenerative condition after Alzheimer disease; prevalence increases sharply after age 60.
- Diagnosis is clinical — the MDS Clinical Diagnostic Criteria (2015) require bradykinesia plus resting tremor and/or rigidity, with supportive features (clear levodopa response, rest tremor, olfactory loss) strengthening confidence.
- Red flags for atypical parkinsonism include early falls, symmetric onset, rapid progression, supranuclear gaze palsy, cerebellar signs, and early autonomic failure — these should prompt specialist reassessment.
- Levodopa/carbidopa (e.g. Sinemet®) remains the most effective symptomatic therapy across all ages; starting with levodopa is recommended for most patients aged ≥65 or those with significant functional impairment.
- Dopamine agonists (pramipexole, ropinirole, rotigotine) and MAO-B inhibitors (selegiline, rasagiline, safinamide) are alternatives for younger patients to delay levodopa-related motor complications.
- Motor complications — wearing-off, peak-dose dyskinesia, and on–off phenomena — affect up to 50% of patients within 5–10 years of levodopa initiation and require stepwise pharmacologic adjustment.
- Non-motor symptoms (constipation, orthostatic hypotension, REM sleep behaviour disorder, depression, cognitive impairment, pain) are common, often more disabling than motor features, and must be actively screened.
- A levodopa challenge test (single-dose 250 mg levodopa with objective UPDRS-III scoring) is recommended when diagnostic uncertainty exists — a ≥30% improvement supports PD diagnosis.
- Advanced therapies — deep brain stimulation (DBS), levopa–carbidopa intestinal gel (Duodopa®), and subcutaneous apomorphine infusion — should be considered when motor complications are inadequately controlled by oral medications.
- Aboriginal and Torres Strait Islander Australians may face delayed diagnosis due to limited specialist access in remote areas; culturally appropriate education and telehealth neurology services are essential.
- All patients require a multidisciplinary team approach including physiotherapy, speech pathology, occupational therapy, dietetics, and psychology, coordinated through the GP.
Introduction & Australian Epidemiology
Parkinson disease (PD) is a progressive neurodegenerative disorder characterised by the loss of dopaminergic neurons in the substantia nigra pars compacta and the accumulation of alpha-synuclein-containing Lewy bodies. It is the second most common neurodegenerative condition in Australia after Alzheimer disease and is the fastest-growing neurological disorder globally in terms of prevalence, disability, and deaths.
Australian Burden of Disease
- An estimated 80,000–100,000 Australians are living with PD (AIHW 2023), with approximately 30–40 new diagnoses per 100,000 population per year.
- Prevalence increases with age: approximately 1–2% of Australians aged ≥65 and up to 4% of those aged ≥85 are affected.
- Men are 1.5 times more likely to be diagnosed than women.
- The total economic cost of PD in Australia exceeds $10.7 billion annually (including direct health costs, informal carer costs, and lost productivity).
- PD is the 14th leading cause of death in Australia, with a median survival of 12–15 years from diagnosis when optimally managed.
Risk Factors
| Factor | Detail |
|---|---|
| Age | Strongest risk factor; incidence rises sharply after age 60 |
| Male sex | Male-to-female ratio approximately 1.5:1 |
| Genetic | LRRK2, GBA, SNCA, PINK1, PARK7 mutations; family history increases risk 2–5× |
| Environmental | Pesticide exposure (rotenone, paraquat), rural living, heavy metals, well-water drinking |
| Protective | Caffeine consumption, smoking (epidemiological association only — not a therapeutic recommendation), physical activity |
| Head injury | Moderate-to-severe traumatic brain injury increases risk approximately 1.5–2× |
Diagnosis of Parkinson Disease
The diagnosis of PD remains fundamentally clinical. There is no single confirmatory laboratory test or imaging modality. The Movement Disorder Society (MDS) Clinical Diagnostic Criteria (2015) provide a structured framework with ascending levels of diagnostic certainty.
MDS Clinical Diagnostic Criteria (2015)
Core motor feature (mandatory): Bradykinesia, defined as slowness of movement and progressive decrement in amplitude or speed with repeated actions, must be present.
Supportive Criteria (increase diagnostic confidence)
- Clear and dramatic beneficial response to dopaminergic therapy (levodopa or dopamine agonist challenge)
- Presence of levodopa-induced dyskinesias
- Rest tremor of a limb (documented on examination)
- Positive olfactory loss or cardiac sympathetic denervation on MIBG scintigraphy
Absolute Exclusion Criteria
- Cerebellar abnormalities (gait ataxia, limb ataxia, cerebellar oculomotor dysfunction)
- Supranuclear gaze palsy (vertical down-gaze limitation characteristic of PSP)
- Primary progressive aphasia or semantic/alogic variant frontotemporal dementia within 5 years of motor onset
- Parkinsonism restricted to lower limbs for >3 years (consider vascular parkinsonism)
- Treatment with a dopamine-blocking agent consistent with drug-induced parkinsonism
Red Flags for Atypical Parkinsonism
| Atypical Condition | Key Distinguishing Features |
|---|---|
| Multiple System Atrophy (MSA) | Early autonomic failure (urinary incontinence, orthostatic hypotension), cerebellar ataxia (MSA-C) or parkinsonism (MSA-P), stridor, poor levodopa response |
| Progressive Supranuclear Palsy (PSP) | Vertical supranuclear gaze palsy, early falls (within 1 year), axial rigidity, retrocollis, pseudobulbar palsy |
| Corticobasal Degeneration (CBD) | Asymmetric limb rigidity, alien limb phenomenon, cortical sensory loss, apraxia, myoclonus |
| Dementia with Lewy Bodies (DLB) | Dementia preceding or within 1 year of parkinsonism, visual hallucinations, fluctuating cognition, REM sleep behaviour disorder |
Investigations
No routine blood test confirms PD. Investigations serve to exclude secondary causes and support diagnosis where clinical uncertainty exists.
Levodopa Challenge Test
When diagnostic uncertainty remains, a supervised levodopa challenge is the gold-standard supportive test:
- Withhold all dopaminergic medications for ≥12 hours (≥24 hours for extended-release formulations)
- Administer a single dose of levodopa/carbidopa 250/25 mg (Sinemet®) or dispersible levodopa/benserazide 100/25 mg (Madopar®)
- Score UPDRS-III (motor) before and 60–90 minutes after dosing
- A ≥30% improvement in UPDRS-III motor score is considered a positive response and strongly supports idiopathic PD
- False negatives may occur in early disease or with inadequate dosing
Initial Pharmacologic Therapy
The choice of initial dopaminergic therapy in PD is one of the most important treatment decisions and must be individualised based on patient age, symptom severity, functional impact, comorbidities, and patient preference. There is no single "correct" first-line agent — the key decision is between levodopa and dopamine agonists, with MAO-B inhibitors as a third option for mild symptoms.
Treatment Algorithm by Age and Severity
First-Line Agents
MAO-B Inhibitors
Levodopa vs Dopamine Agonists — Key Trade-offs
| Factor | Levodopa | Dopamine Agonists | ||
|---|---|---|---|---|
| Motor efficacy | Superior; most effective agent for motor symptoms | Good but generally inferior to levodopa for bradykinesia and rigidity | ||
| Motor complications | Higher risk of wearing-off and dyskinesia with long-term use | Delayed onset of motor complications (by 2–3 years on average) | ||
| Impulse control disorders | Lower risk | Hallucinations/psychosis | Risk increases with dose and disease duration | Higher risk, particularly in elderly and those with cognitive impairment |
| Peripheral ADRs | Nausea, orthostatic hypotension (reduced by carbidopa/benserazide) | Nausea, oedema (peripheral), somnolence, sleep attacks | ||
| Best for | Patients ≥65, significant functional impairment, cognitive concerns | Younger patients (<65), mild symptoms, desire to delay motor complications |
Adjunctive Therapies for Early Disease
Motor Complications
Motor complications are the hallmark of advancing PD and are directly related to chronic levodopa use, progressive dopaminergic denervation, and the short half-life of standard levodopa formulations (approximately 90 minutes). Up to 50% of patients develop motor fluctuations within 5 years of levodopa initiation, rising to 70–80% at 10 years.
Types of Motor Complications
Diphasic Dyskinesia
A less common pattern where dyskinesia occurs at both the onset and end of a levodopa dose, with a relatively immobile period in between. Often painful (dystonic) and more difficult to manage than peak-dose dyskinesia.
Stepwise Management of Motor Complications
Step 1: Optimise Levodopa Delivery
- Fractionate doses — smaller, more frequent doses of levodopa (e.g. 100/25 mg four to five times daily instead of 200/50 mg three times daily)
- Use dispersible levodopa (Madopar® dispersible) for faster onset during "off" periods
- Take levodopa on an empty stomach (30 minutes before meals) — protein competes with levodopa for intestinal absorption; advise consistent protein distribution across the day
- Consider controlled-release formulations (e.g. Sinemet CR, Madopar HBS) for nighttime symptoms — note: may worsen daytime dyskinesia due to unpredictable absorption
Step 2: Add Adjunct Therapies
Step 3: Consider Advanced Therapies
Referral to a movement disorder specialist should be considered when motor fluctuations are not adequately controlled with oral medication adjustments (Step 1 and 2). Advanced therapies include:
| Therapy | Mechanism | Indications | Availability |
|---|---|---|---|
| Deep Brain Stimulation (DBS) | Bilateral STN or GPi electrode implantation delivering continuous high-frequency stimulation | Motor fluctuations and/or dyskinesia inadequately controlled medically; good cognitive function; no active psychiatric illness; good levodopa response (≥30% improvement) | Available at major centres: Royal Melbourne, Westmead, Flinders, Royal Brisbane, Sir Charles Gairdner |
| Levodopa–Carbidopa Intestinal Gel (Duodopa®) | Continuous jejunal infusion via PEG-J stoma providing stable levodopa levels | Severe motor fluctuations and dyskinesia refractory to optimised oral therapy; unsuitable for DBS | PBS Authority Required — specialist-initiated only |
| Subcutaneous Apomorphine Infusion | Continuous SC apomorphine via pump, providing 12–16 hours of continuous dopaminergic stimulation | Motor fluctuations in patients not suitable for DBS or Duodopa; can be trialled before more invasive options | Specialist-initiated; requires domperidone cover |
Non-Motor Symptoms
Non-motor symptoms (NMS) are ubiquitous in PD and are often more disabling than the motor features. They may precede motor onset by years (prodromal PD), contribute significantly to reduced quality of life, predict nursing home placement, and are frequently under-recognised. Up to 95% of patients with PD report at least one NMS, and the mean number per patient is 7–10.
Autonomic Dysfunction
| Symptom | Prevalence | First-Line Treatment |
|---|---|---|
| Constipation | 60–80% | Dietary fibre, adequate fluids, regular exercise; macrogol 3350 (Movicol®); osmotic laxatives; if refractory: prucalopride (Resotran®) 2 mg daily — PBS Authority Required |
| Orthostatic hypotension | 30–50% | Review and reduce antihypertensives; increase salt and fluid intake; compression stockings; fludrocortisone 50–200 mcg/day PO (PBS General Benefit); midodrine 2.5–10 mg PO TDS (PBS Authority Required for orthostatic hypotension) |
| Urinary dysfunction | 30–70% | Exclude UTI; bladder training; avoid evening fluids; for overactive bladder: solifenacin (Vesicare®) 5–10 mg/day or mirabegron (Betmiga®) 25–50 mg/day — specialist advice for refractory cases |
| Sialorrhoea (drooling) | 30–50% | Glycopyrrolate (glycopyrronium) 1 mg PO BD–TDS; botulinum toxin injections to salivary glands (specialist); speech therapy for swallow strategies |
| Gastroparesis | 20–50% | Small frequent meals; avoid high-fat meals; may impair levodopa absorption — consider liquid levodopa or jejunal delivery; domperidone 10 mg PO TDS (PBS General Benefit) — preferred prokinetic in PD (does not cross BBB) |
Sleep Disorders
| Sleep Disorder | Features & Treatment |
|---|---|
| REM Sleep Behaviour Disorder (RBD) | Dream enactment behaviour (punching, kicking, shouting during sleep); very common in PD (30–50%); may precede motor symptoms by decades. First-line: clonazepam 0.5–2 mg PO nocte or melatonin 3–12 mg PO nocte. Safety measures: remove sharp objects from bedside, place mattress on floor, consider bed rails. |
| Excessive Daytime Somnolence | Affects 20–40%. Review dopaminergic medications (DA agonists and levodopa are common causes); address sleep hygiene; exclude sleep apnoea (polysomnography referral). Modafinil 100–200 mg mane may be considered — not PBS-listed for PD. |
| Insomnia | Common; often multifactorial (nocturia, off-periods, pain, RBD, mood disorder). Optimise dopaminergic therapy for nocturnal off-periods (controlled-release levodopa at bedtime). Avoid benzodiazepines long-term in elderly — prefer melatonin or trazodone. |
| Restless Legs Syndrome | Overlap with PD is common. Dopamine agonists (pramipexole, ropinirole) or gabapentin enacarbil (Horizant®) are first-line. Check ferritin level — supplement if <75 mcg/L. |
Mood and Cognitive Changes
Depression
- Prevalence: 40–50% of PD patients; may be reactive or neurobiological (related to serotonin and dopamine depletion)
- Screening: PHQ-9 or Montgomery–Åsberg Depression Rating Scale (MADRS) at diagnosis and annually
- First-line pharmacotherapy: SSRIs (citalopram 10–20 mg/day or sertraline 50–100 mg/day) — generally well-tolerated in PD
- SNRIs (venlafaxine 75–150 mg/day, desvenlafaxine 50–100 mg/day) are an alternative — may also help with pain and fatigue
- Tricyclic antidepressants (nortriptyline 25–75 mg nocte) may be useful when insomnia and pain are comorbid — caution with anticholinergic burden and cardiac effects
- Non-pharmacological: cognitive behavioural therapy (CBT) has level-1 evidence in PD depression; exercise therapy is beneficial
Anxiety
- Prevalence: 25–40%; frequently co-exists with depression and often fluctuates with motor "off" periods
- SSRIs/SNRIs as above; benzodiazepines to be avoided long-term due to fall risk and cognitive effects
- Psychological therapies (CBT, mindfulness-based stress reduction) are effective
Cognitive Impairment and Dementia
- Mild cognitive impairment (PD-MCI) affects 20–30% at diagnosis; PD dementia (PDD) develops in up to 80% over 15–20 years
- Screening: Montreal Cognitive Assessment (MoCA) — validated in PD; repeat annually
- PDD treatment: rivastigmine (Exelon®) 1.5 mg PO BD, titrate to 6 mg BD over 4–8 weeks — PBS Authority Required for PDD; transdermal patch (4.6 mg/24 hours, titrate to 9.5 mg/24 hours) available for patients with swallowing difficulties
- Avoid anticholinergics (benztropine, trihexyphenidyl) in patients with cognitive impairment — will worsen cognition
- Review and reduce polypharmacy; avoid anticholinergic medications and benzodiazepines
Psychosis and Hallucinations
Pain in Parkinson Disease
Pain affects 40–80% of PD patients and is classified into five types (PD Pain Classification Scale):
| Type | Description | Management |
|---|---|---|
| Musculoskeletal | Joint stiffness, frozen shoulder, postural deformities | Physiotherapy, optimise dopaminergic therapy, simple analgesics |
| Dystonic | Early morning foot dystonia, "off"-period dystonia | Optimise levodopa; botox for focal dystonia |
| Central / Neuropathic | Burning, tingling, diffuse pain not explained by musculoskeletal cause | Duloxetine 60 mg/day; gabapentin/pregabalin; amitriptyline (caution in elderly) |
| Akathitic | Restlessness and inner unease, often during "off" periods | Optimise dopaminergic therapy; clonazepam |
| Primary (central) | Unexplained, unresponsive to levodopa | May require opioid-based analgesia under specialist guidance |
Other Non-Motor Symptoms
- Fatigue: Affects 30–50%. Assess for depression, sleep disorders, anaemia. Exercise, energy conservation strategies. Modafinil (off-label) may be considered.
- Anosmia / Hyposmia: Present in >90% of PD patients, often earliest prodromal feature. No effective treatment; advise on food safety (inability to detect spoiled food or gas leaks).
- Dysphagia: Progressive; speech pathology assessment essential; modified diet textures (IDDSI framework); swallowing exercises (Lee Silverman Voice Treatment — LSVT LOUD).
- Sexual dysfunction: Common and under-discussed. May be dopaminergic medication-related (hypersexuality) or disease-related (erectile dysfunction, vaginal dryness). PDE5 inhibitors for erectile dysfunction; dose adjustment of dopamine agonists for ICD-related hypersexuality.
Special Populations
Pregnancy
Elderly (≥75 years)
Renal Impairment
Hepatic Impairment
Cognitive Impairment / Dementia
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians have a lower overall prevalence of diagnosed PD compared with non-Indigenous Australians, but this may reflect under-diagnosis rather than a true lower incidence. Barriers to early diagnosis and optimal management are significant, particularly in remote and very remote communities.
📚 References
- 1. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord. 2015;30(12):1591–1601.
- 2. Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021;397(10291):2284–2303.
- 3. Fox SH, Katzenschlager R, Lim SY, et al. International Parkinson and Movement Disorder Society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson's disease. Mov Disord. 2018;33(8):1248–1266.
- 4. Seppi K, Ray Chaudhuri K, Coelho M, et al. Update on treatments for nonmotor symptoms of Parkinson's disease — an evidence-based medicine review. Mov Disord. 2019;34(2):180–198.
- 5. Australian Institute of Health and Welfare (AIHW). Dementia in Australia: Impacts of dementia. AIHW, Canberra. 2024.
- 6. Parkinson's Australia. Living with Parkinson's Disease — National Survey Report. Parkinson's Australia, 2023.
- 7. de Bie RMA, Clarke CE, Espay AJ, et al. Initiation of pharmacological therapy in Parkinson's disease: when, why, and how. Lancet Neurol. 2023;22(5):436–446.
- 8. Rinaldi D, Assogna F, Casula EP, et al. Impulse control disorders in Parkinson's disease: clinical features, pathophysiology and management. J Neurol Neurosurg Psychiatry. 2023;94(2):149–158.
- 9. Titova N, Chaudhuri KR. Non-motor Parkinson disease: new concepts and personalised management. Med J Aust. 2018;208(9):404–409.
- 10. Royal Australian College of General Practitioners (RACGP). Management of Parkinson's disease in primary care. Aust J Gen Pract. 2022;51(6):364–370.
- 11. Deuschl G, Paschen S, Witt K. Clinical outcome of deep brain stimulation for Parkinson's disease. Handb Clin Neurol. 2013;116:107–128.
- 12. Australian Government Department of Health and Aged Care. Pharmaceutical Benefits Scheme (PBS) — Schedule of Pharmaceutical Benefits. Canberra: Commonwealth of Australia; 2025.
- 13. Marsden CD, Parkes JD. "On-off" effects in patients with Parkinson's disease on chronic levodopa therapy. Lancet. 1976;1(7954):292–296.
- 14. Chaudhuri KR, Martinez-Martin P, Brown RG, et al. The metric properties of a novel non-motor symptoms scale for Parkinson's disease: results from an international pilot study. Mov Disord. 2007;22(13):1901–1911.
- 15. Djamshidian A, O'Sullivan SS, Lees A, Averbeck BB. Stimulation of the subthalamic nucleus impairs reversal learning and decision-making. Brain. 2013;136(Pt 1):223–233.