📋 Key Information Summary
- Dementia affects approximately 411,000 Australians, with numbers projected to exceed 800,000 by 2054; Aboriginal and Torres Strait Islander peoples experience dementia at 3–5 times the general population rate.
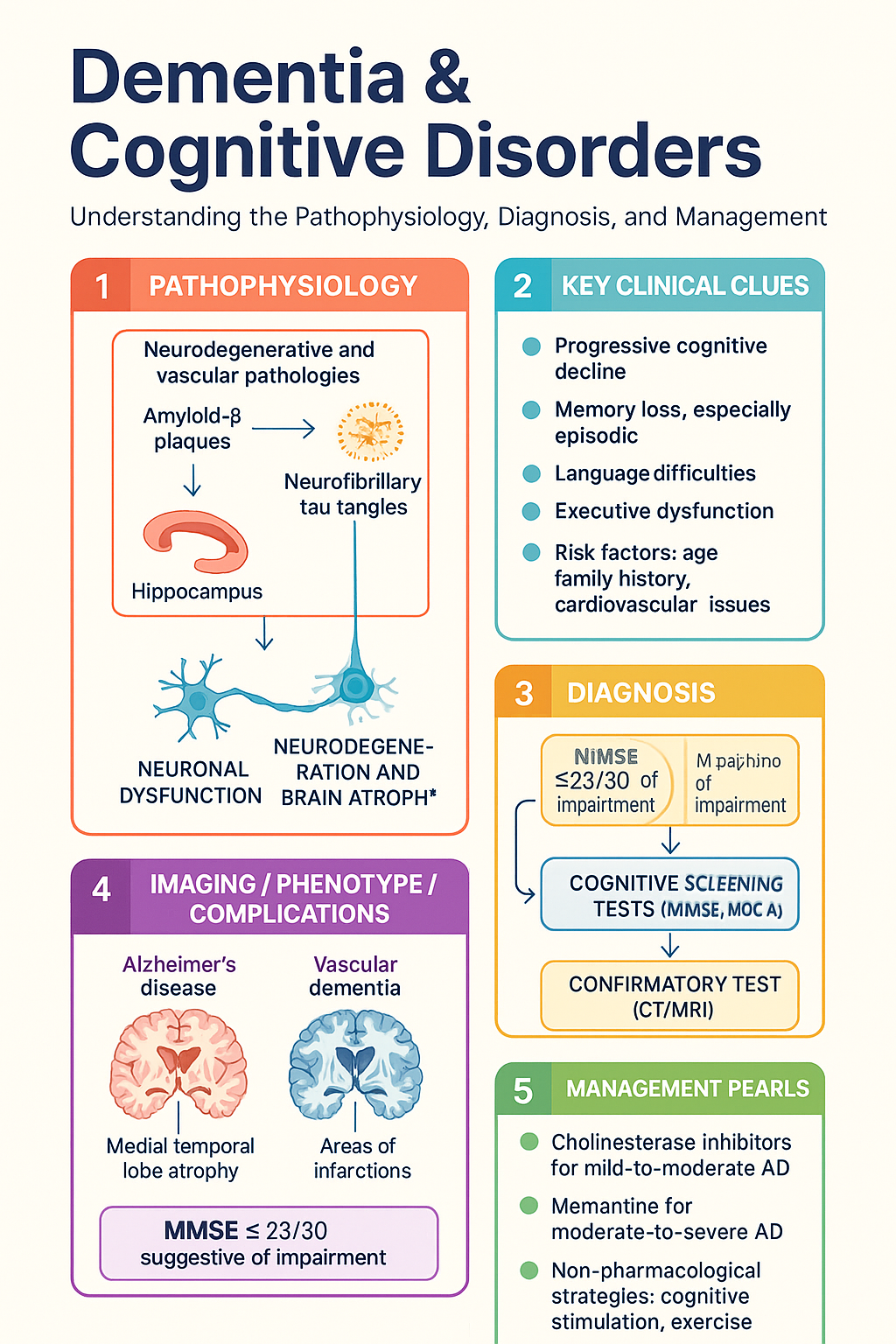
- Cognitive screening in primary care should be prompted by patient, family, or clinician concern — use the MMSE (≤23/30 suggestive), MoCA (≤25/30 suggestive), or clock-drawing test as a rapid bedside screen.
- Always exclude reversible causes of cognitive decline before diagnosing dementia: hypothyroidism, vitamin B12/folate deficiency, normal pressure hydrocephalus, neurosyphilis, and medication-related cognitive impairment (anticholinergics, benzodiazepines, opioids).
- Delirium must be distinguished from dementia — delirium has acute onset, fluctuating course, altered consciousness, and is a medical emergency requiring urgent assessment and treatment of underlying cause.
- Alzheimer disease (AD) accounts for 60–70% of dementia; vascular dementia is the second most common; dementia with Lewy bodies (DLB) and frontotemporal dementia (FTD) each account for 5–10%.
- Initial workup includes detailed collateral history, medication review, baseline bloods (B12, folate, TSH, FBC, UEC, LFTs, glucose, calcium, RPR/VDRL), and structural brain imaging (CT or MRI) when diagnosis is uncertain.
- Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) are PBS Authority Required for mild-to-moderate AD; memantine is PBS-listed for moderate-to-severe AD where cholinesterase inhibitors are not tolerated.
- Non-pharmacological strategies — cognitive stimulation therapy, physical exercise programmes, music therapy, and structured daily routines — have level A evidence and should be first-line alongside pharmacotherapy.
- Antipsychotics carry a boxed warning for increased mortality in dementia-related psychosis; use only for severe behavioural disturbance when non-pharmacological measures fail, at the lowest dose for the shortest duration.
- Driving assessment is mandatory — clinicians have a legal and ethical duty to assess fitness to drive; use the Austroads guidelines and refer for formal occupational therapy driving assessment when indicated.
- Carer burden is substantial — refer early to Dementia Australia (1800 100 500), My Aged Care (1800 200 422), and state-based carer support services; respite care should be discussed at diagnosis.
- Advance care planning should be initiated early while the patient retains decision-making capacity, including appointment of an enduring power of attorney and health directive.
Introduction & Australian Epidemiology
Dementia is a clinical syndrome characterised by progressive decline in cognitive function sufficient to interfere with daily activities and independence. It is not a single disease but rather a constellation of symptoms caused by various neurodegenerative and vascular pathologies. In Australia, dementia is the second leading cause of death and the leading cause of burden of disease among people aged 65 years and older.
According to the Australian Institute of Health and Welfare (AIHW), approximately 411,100 Australians were living with dementia in 2023, with this number projected to reach 849,300 by 2054. The total annual cost of dementia in Australia exceeds $26.6 billion, encompassing direct health costs, aged care, and informal carer contributions. Dementia is the leading cause of death in Australian women and the second leading cause overall.
| Parameter | Statistic |
|---|---|
| Prevalence (≥65 years) | Approximately 1 in 10 Australians aged ≥65; 1 in 3 aged ≥85 |
| Estimated Australians living with dementia (2023) | ~411,100 |
| Projected prevalence by 2054 | ~849,300 |
| Proportion in residential aged care | ~52% of permanent aged care residents have dementia |
| ATSI prevalence ratio | 3–5 times higher than non-Indigenous Australians |
| Younger-onset dementia (<65 years) | ~28,000 Australians; ~12,400 under 55 years |
| Annual cost | >$26.6 billion (direct + indirect + informal care) |
Risk factors for dementia include increasing age (strongest risk factor), family history, cardiovascular risk factors (hypertension, diabetes, obesity, physical inactivity), traumatic brain injury, depression, excessive alcohol consumption, hearing loss, social isolation, and air pollution exposure. Modifiable risk factors account for approximately 40% of dementia cases globally (Lancet Commission 2020).
Cognitive Screening in Primary Care
Cognitive screening in primary care is not recommended as a universal population-level screen for all older adults (USPSTF concludes insufficient evidence for universal screening). Instead, screening should be triggered by concerns raised by the patient, a family member, carer, or the treating clinician's observation of functional decline. The RACGP Red Book recommends routine enquiry about cognition at health assessments for patients aged ≥75 years (MBS Item 707).
When to Screen
- Patient or informant expresses concern about memory or cognitive changes
- Observed functional decline — missed appointments, medication errors, financial mismanagement, difficulty managing household tasks
- Annual health assessment for patients aged ≥75 years (MBS Item 707)
- Following an acute medical event (hospitalisation, fall, delirium episode)
- New psychiatric presentation in an older adult (depression, anxiety, behavioural changes) — consider cognitive component
- Patients with cardiovascular risk factors or known cerebrovascular disease at increased risk of vascular cognitive impairment
Screening Instruments
| Tool | Score / Interpretation | Time | Strengths | Limitations |
|---|---|---|---|---|
| Mini-Mental State Examination (MMSE) | ≤23/30 suggestive of cognitive impairment; 18–23 = mild; 10–17 = moderate; <10 = severe | 5–10 min | Most widely validated; good for moderate-severe impairment; well normed | Copyrighted (PAR Inc); ceiling effect in mild impairment; less sensitive to MCI; education bias |
| Montreal Cognitive Assessment (MoCA) | ≤25/30 suggestive (add 1 point if ≤12 years education); sensitive to MCI | 10–15 min | Superior sensitivity for MCI; assesses executive function; free to use (moCA test) | May be too sensitive (high false positive in low education/ESL); requires training |
| General Practitioner Assessment of Cognition (GPCOG) | Patient section: ≤4/9 suggests impairment; informant section adds 6 points | 5 min | Designed for Australian GPs; free; includes informant component; culturally appropriate | Less widely validated internationally than MMSE/MoCA |
| Clock Drawing Test (CDT) | Various scoring systems; qualitative assessment of visuospatial and executive function | 2–3 min | Quick; no language requirement; useful as adjunct; good for visuospatial assessment | No standardised scoring; limited sensitivity when used alone |
| Rowland Universal Dementia Assessment Scale (RUDAS) | ≤22/30 suggestive of cognitive impairment | 5–10 min | Designed for culturally and linguistically diverse populations; free; less education bias | Less normative data than MMSE; may miss subtle executive dysfunction |
Reversible Causes to Consider Before Diagnosis
Up to 5–15% of suspected dementia cases may have a partially or fully reversible cause. All patients with new cognitive complaints should be evaluated for:
- Hypothyroidism — TSH and free T4; treatable with levothyroxine
- Vitamin B12 and folate deficiency — common in elderly; may cause subacute combined degeneration and cognitive impairment; check serum B12, folate, methylmalonic acid if borderline
- Normal pressure hydrocephalus (NPH) — classic triad of gait disturbance, urinary incontinence, and dementia; treatable with ventriculoperitoneal shunting; CT/MRI shows ventriculomegaly disproportionate to sulcal widening
- Medication-related cognitive impairment — anticholinergics (antihistamines, TCAs, bladder antispasmodics), benzodiazepines, opioids, antipsychotics, corticosteroids, polypharmacy
- Depression (pseudodementia) — may mimic dementia, particularly in older adults; treat depression and reassess cognition
- Chronic subdural haematoma — history of falls/anticoagulation; CT head
- Neurosyphilis — RPR/VDRL and FTA-ABS if risk factors present
- Obstructive sleep apnoea — associated with cognitive impairment; sleep study if symptomatic
- HIV-associated neurocognitive disorder — consider in at-risk populations
- Alcohol-related brain damage — chronic excessive alcohol use
Differential Diagnosis of Dementia
Accurate differentiation of dementia subtypes is critical for prognosis, treatment selection, genetic counselling, and care planning. The most common differentials are outlined below.
Alzheimer Disease (AD)
- Accounts for 60–70% of all dementia cases
- Insidious onset with gradual progressive decline in episodic memory as the earliest and most prominent feature
- Early: difficulty forming new memories, repeating questions, misplacing items
- Middle: language difficulties (anomia, aphasia), visuospatial deficits, apraxia, executive dysfunction, behavioural changes
- Late: severe global impairment, loss of ambulation, incontinence, dysphagia
- Neuropathology: amyloid-β plaques and neurofibrillary tau tangles; medial temporal lobe (hippocampal) atrophy on MRI
- Risk factors: age, APOE ε4 allele (homozygous 8–15× increased risk), family history, Down syndrome, cardiovascular risk factors
Vascular Dementia
- Second most common cause (~15–20%); may co-exist with AD (mixed dementia — most common autopsy finding)
- Stepwise or gradual decline; executive dysfunction, psychomotor slowing, and impaired attention often more prominent than memory loss early
- Associated with cardiovascular risk factors: hypertension, diabetes, atrial fibrillation, smoking, hyperlipidaemia
- Subtypes: multi-infarct dementia, strategic single-infarct dementia, subcortical vascular dementia (Binswanger disease), post-stroke dementia
- Imaging: white matter hyperintensities, lacunar infarcts, cortical infarcts on MRI; Fazekas scale for white matter disease grading
- Prevention focus: aggressive cardiovascular risk factor management
Dementia with Lewy Bodies (DLB)
- Accounts for 5–10% of dementia cases
- Core features: fluctuating cognition with pronounced variations in attention and alertness, recurrent well-formed visual hallucinations, spontaneous parkinsonism (bradykiness, rigidity, postural instability)
- Supportive features: REM sleep behaviour disorder (may precede dementia by years), severe neuroleptic sensitivity, systematised delusions, falls and syncope
- DAT-SPECT (DaTSCAN) shows reduced dopamine transporter uptake in the putamen (distinguishes DLB from AD); available at nuclear medicine centres (MBS nuclear medicine items)
- Cholinesterase inhibitors are particularly effective in DLB and may improve cognition, hallucinations, and fluctuations
Frontotemporal Dementia (FTD)
- Accounts for 5–10% of all dementia; proportionally higher in younger-onset dementia (up to 20–30% of cases <65 years)
- Behavioural variant FTD (bvFTD): personality change, disinhibition, apathy, loss of empathy, dietary changes (sweet cravings, hyperorality), stereotyped behaviours, executive dysfunction with relatively preserved memory initially
- Primary progressive aphasias (PPA): semantic variant (loss of word meaning, face recognition), nonfluent/agrammatic variant (effortful speech, grammatical errors), logopenic variant (word-finding pauses, phonemic errors — may overlap with AD pathology)
- Imaging: bilateral frontal and/or anterior temporal lobe atrophy on MRI; often asymmetric; FFDG-PET shows frontotemporal hypometabolism
- Often misdiagnosed as depression, psychosis, or personality disorder in early stages; frequently negative on standard cognitive screening
- Cholinesterase inhibitors are NOT effective and may worsen behavioural symptoms in bvFTD
Depression-Related Cognitive Impairment (Pseudodementia)
- Major depressive disorder in older adults can cause significant cognitive impairment ("depression-related cognitive dysfunction")
- Clues: temporal relationship with mood symptoms, patient complains of memory loss and tries hard but performs poorly ("don't know" answers), affect is flat/tearful, vegetative symptoms present, relatively recent onset
- Contrast with AD: patient often minimises difficulties, confabulates, shows less distress
- Geriatric Depression Scale (GDS-15) is a useful adjunct; score ≥5 suggests depression
- Treat depression and reassess cognition at 8–12 weeks; persistent cognitive deficits after mood improvement suggest comorbid neurodegeneration
- Late-life depression may be both a prodrome and a risk factor for dementia
Delirium vs Dementia
| Feature | Delirium | Dementia |
|---|---|---|
| Onset | Acute (hours to days) | Insidious (months to years) |
| Course | Fluctuating, often worse at night (sundowning) | Gradual, progressive decline |
| Consciousness | Altered — clouded, drowsy, hyperalert | Normal until late stages |
| Attention | Markedly impaired (hallmark feature) | Relatively preserved until moderate–severe |
| Orientation | Impaired for time, often place | May be preserved early |
| Memory | Impaired, especially registration | Impaired, especially recall |
| Perception | Visual hallucinations common, illusions | Hallucinations less common except in DLB |
| Psychomotor | Hyperactive, hypoactive, or mixed | Usually normal early |
| Reversibility | Usually reversible with treatment of cause | Generally irreversible (except treatable causes) |
| Duration | Days to weeks (usually <1 week) | Years (progressive) |
Other Important Differentials
- Posterior cortical atrophy (PCA): Visual variant of AD; progressive visuospatial dysfunction, simultanagnosia, optic ataxia, oculomotor apraxia (Balint syndrome); patients often present to ophthalmology first
- Progressive supranuclear palsy (PSP): Parkinsonism, vertical supranuclear gaze palsy, early falls, frontal behavioural changes
- Corticobasal degeneration (CBD): Asymmetric parkinsonism, alien limb phenomenon, apraxia, cortical sensory loss
- Creutzfeldt-Jakob disease (CJD): Rapidly progressive dementia, myoclonus, cerebellar signs, periodic sharp wave complexes on EEG; refer urgently to state health authority
- HIV-associated neurocognitive disorder (HAND): Consider in at-risk populations; screen with HIV serology
- Chronic traumatic encephalopathy (CTE): History of repetitive head impacts (contact sports, military service)
