📋 Key Information Summary
- Multiple sclerosis (MS) is the most common chronic inflammatory demyelinating disease of the central nervous system, affecting approximately 33,000 Australians, with prevalence highest in temperate southern states (Tasmania, Victoria).
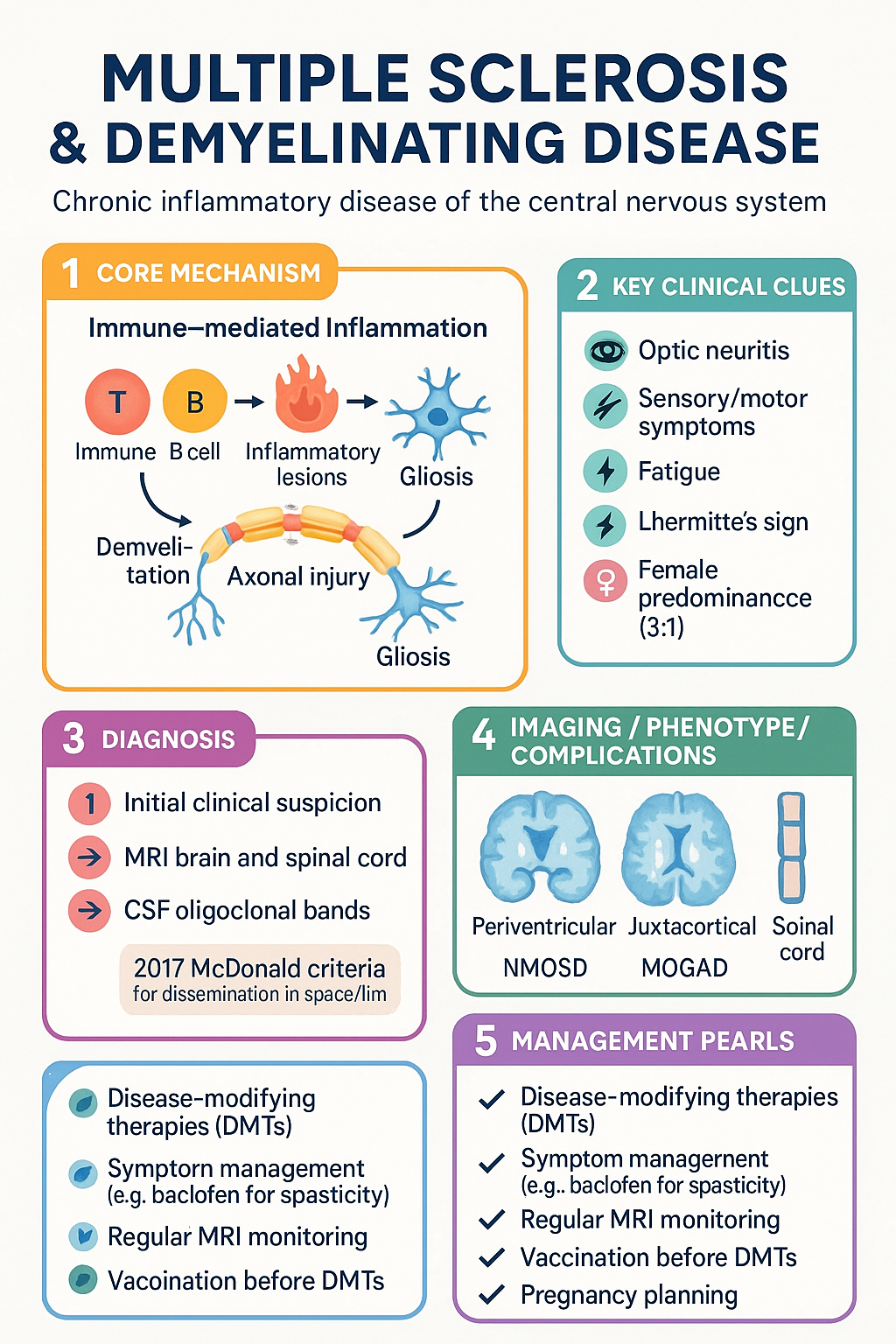
- Clinically isolated syndrome (CIS) is a first clinical episode suggestive of demyelination; MRI lesions fulfilling the 2017 McDonald criteria allow dissemination in space and time to be satisfied at presentation, enabling earlier diagnosis.
- CSF oligoclonal bands are detected in ≥90% of MS patients and can substitute for dissemination in time when MRI criteria are not fully met (2017 McDonald revision).
- Diagnosis requires exclusion of MS mimics including neuromyelitis optica spectrum disorder (NMOSD), MOG antibody disease (MOGAD), systemic lupus erythematosus, sarcoidosis, and vitamin B12 deficiency.
- All suspected MS should be referred to neurology; urgent referral (within 2 weeks) is indicated for acute transverse myelitis, optic neuritis with severe visual loss, or suspected tumefactive MS.
- Disease-modifying therapies (DMTs) are PBS-listed and include injectable (interferon-β, glatiramer), oral (dimethyl fumarate, teriflunomide, fingolimod, siponimod, cladribine), and high-efficacy infused therapies (natalizumab, ocrelizumab, alemtuzumab).
- Symptom management in primary care covers spasticity (baclofen, gabapentin), fatigue (exercise, amantadine off-label), bladder dysfunction (oxybutynin, intermittent self-catheterisation), neuropathic pain (pregabalin, amitriptyline), and mood (SSRIs, psychological support).
- Vaccination should be completed before initiating immunosuppressive DMTs; live vaccines are contraindicated during treatment with most DMTs.
- Pregnancy planning is essential—teriflunomide and fingolimod are teratogenic and require washout; natalizumab and ocrelizumab have specific pre-conception timing guidelines.
- Regular monitoring includes MRI (annual for most DMTs), lymphocyte counts, liver function, JC virus antibody status (natalizumab), and screening for opportunistic infections.
- Aboriginal and Torres Strait Islander Australians face delayed diagnosis due to geographic barriers, reduced specialist access, and culturally inappropriate service delivery, requiring tailored outreach and telehealth solutions.
- Mental health screening with PHQ-9 and GAD-7 should occur at every clinic visit; depression affects up to 50% of people with MS and significantly impacts treatment adherence and quality of life.
Introduction & Australian Epidemiology
Multiple sclerosis is a chronic, immune-mediated demyelinating disease of the central nervous system characterised by inflammatory lesions, demyelination, axonal injury, and gliosis in the brain, spinal cord, and optic nerves. It is the most common acquired disabling neurological disease in young adults, typically presenting between ages 20–40 years, with a female-to-male ratio of approximately 3:1.
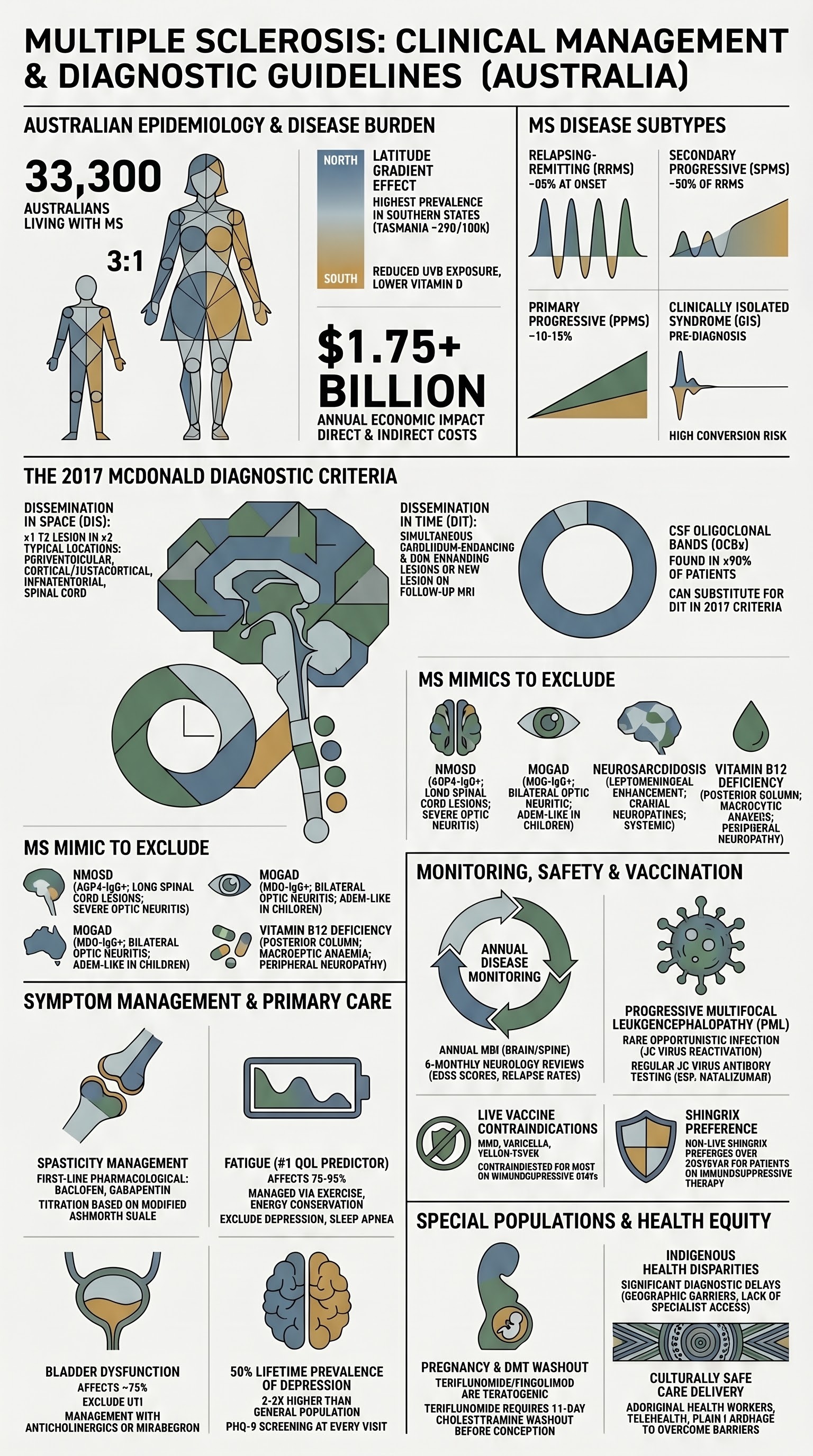
Australia has one of the highest prevalence rates of MS globally. The 2024 AIHW report estimates approximately 33,300 Australians live with MS, equating to a prevalence of around 130 per 100,000 population. Prevalence demonstrates a clear latitude gradient, with Tasmania (~290 per 100,000) and Victoria having the highest rates, consistent with the well-established relationship between distance from the equator, reduced ultraviolet B exposure, lower vitamin D levels, and MS risk.
Disease Subtypes
| Subtype | Frequency | Characteristics |
|---|---|---|
| Relapsing-remitting MS (RRMS) | ~85% at onset | Discrete relapses with full or partial recovery; stable between attacks |
| Secondary progressive MS (SPMS) | ~50% of RRMS after 15–20 years | Gradual neurological deterioration after initial RRMS course; may have superimposed relapses (active SPMS) |
| Primary progressive MS (PPMS) | ~10–15% | Steady decline from onset without discrete relapses; more common in men, older age at onset (~40–50 years) |
| Clinically Isolated Syndrome (CIS) | Precedes MS diagnosis | First clinical episode; may or may not convert to MS |
Risk Factors
- Genetic: HLA-DRB1*15:01 (strongest single risk factor, OR ~3); first-degree relative risk 2–4% (20–40× general population)
- Environmental: Low vitamin D, Epstein-Barr virus seropositivity (near-universal but higher titres associated), smoking, adolescent obesity
- Protective: High UV exposure, higher vitamin D levels, EBV vaccination (theoretical)
Clinically Isolated Syndrome
Clinically isolated syndrome (CIS) is defined as a first monophasic clinical episode with features suggestive of central nervous system demyelination, lasting at least 24 hours, in the absence of fever or infection. It is the earliest clinical presentation that may ultimately lead to a diagnosis of relapsing-remitting multiple sclerosis.
Typical Presentations
MRI Criteria in CIS
MRI brain and full spinal cord (with gadolinium) is the most important investigation in CIS. The presence of T2/FLAIR white matter lesions in typical periventricular, juxtacortical, infratentorial, or spinal cord distributions allows assessment of dissemination in space (DIS) per the 2017 McDonald criteria.
| MRI Finding | Prognostic Significance | Conversion Risk |
|---|---|---|
| ≥1 T2 lesion in ≥2 typical MS locations (periventricular, cortical/juxtacortical, infratentorial, spinal cord) | Meets DIS; high conversion risk | ~70–80% at 15 years |
| Gadolinium-enhancing + non-enhancing lesion simultaneously | Satisfies DIT without waiting for second clinical attack | ~80–90% at 15 years |
| Normal MRI brain | Lower but not negligible risk | ~20–25% at 15 years |
| Spinal cord lesions at presentation | Independent predictor of MS conversion | Increases conversion risk by ~2× |
CSF Oligoclonal Bands
Cerebrospinal fluid analysis for oligoclonal bands (OCBs) using isoelectric focusing is a key supporting investigation in CIS. OCBs present in CSF but absent from matched serum are found in ≥90% of MS patients and represent intrathecal immunoglobulin synthesis.
- In the 2017 McDonald criteria, CSF OCBs can substitute for dissemination in time (DIT) when MRI DIT criteria are not met — this is a critical change allowing earlier diagnosis
- OCBs are not specific to MS — also found in NMOSD (~30%), MOGAD (~15–20%), neurosarcoidosis, CNS infections, and lymphoma
- CSF cell count, protein, glucose, and cytology should also be analysed to exclude alternative diagnoses
- MBS item 65091 (lumbar puncture) and 73841 (CSF analysis including oligoclonal bands) are available at most Australian public hospitals; OCB testing requires paired serum and CSF samples
Risk of Conversion to MS
Early Disease-Modifying Therapy in CIS
Patients with CIS and high-risk features (≥1 T2 lesion on MRI, positive CSF OCBs) should be considered for early DMT initiation, as this reduces conversion to MS and long-term disability accumulation. Several DMTs have PBS authority approval for use in CIS with high-risk MRI features in Australia.
Diagnosis of Multiple Sclerosis
The diagnosis of MS requires objective evidence of demyelination disseminated in both space (DIS — multiple areas of the CNS affected) and time (DIT — lesions occurring at different time points). The 2017 McDonald criteria are the internationally accepted diagnostic framework, with specific modifications applicable to Australian practice.
2017 McDonald Diagnostic Criteria — Relapsing MS
| Clinical Presentation | Additional Data Needed for Diagnosis |
|---|---|
| ≥2 clinical attacks + objective clinical evidence of ≥2 lesions | None further required — clinical criteria sufficient |
| ≥2 attacks + objective evidence of 1 lesion | DIS by MRI (≥1 T2 lesion in ≥2 of 4 typical locations: periventricular, cortical/juxtacortical, infratentorial, spinal cord) OR await second clinical attack in different CNS location |
| 1 clinical attack + objective evidence of ≥2 lesions | DIT by MRI (simultaneous gadolinium-enhancing and non-enhancing lesions OR new T2/contrast-enhancing lesion on follow-up MRI) OR CSF OCBs OR await second clinical attack |
| 1 clinical attack + 1 lesion (clinically isolated syndrome) | DIS by MRI + DIT by MRI OR CSF OCBs + DIT by MRI OR await second clinical attack |
| Insidious neurological progression suggestive of MS (PPMS) | ≥1 year of disability progression (retrospective or prospective) PLUS 2 of 3: ≥1 T2 lesion in periventricular, cortical/juxtacortical, or infratentorial regions; ≥2 T2 lesions in spinal cord; CSF OCBs |
2017 McDonald Criteria — Key Revisions Relevant to Australian Practice
- Symptomatic lesions can now be counted toward DIS and DIT (previously excluded)
- Cortical lesions now count toward DIS alongside juxtacortical lesions
- CSF OCBs can substitute for DIT in all clinical presentations
- The criteria may be applied to diverse populations but were primarily validated in predominantly Caucasian cohorts; caution in Asian and Afro-Caribbean populations where NMOSD prevalence is higher
Differential Diagnosis — Must Not Be Missed
| Condition | Distinguishing Features | Key Investigations |
|---|---|---|
| NMOSD (AQP4-IgG) | Severe optic neuritis, complete transverse myelitis (≥3 vertebral segments), area postrema syndrome (intractable nausea/vomiting), bilateral or simultaneous CNS events | AQP4-IgG (serum cell-based assay); MRI long cord lesion ≥3 segments; brain MRI may be normal |
| MOG antibody disease (MOGAD) | Bilateral optic neuritis, ADEM-like presentation (especially children), conus/cauda equina lesions, relapsing course possible | MOG-IgG (live cell-based assay); MRI optic nerve enhancement; may have negative OCBs |
| Systemic lupus erythematosus / Sjögren's syndrome | Multisystem features, rash, arthritis, serositis; CNS vasculitis can mimic MS lesions | ANA, anti-dsDNA, ENA, complement levels, anti-Ro/anti-La |
| Neurosarcoidosis | Leptomeningeal enhancement, cranial neuropathies, hypothalamic/pituitary involvement, systemic features | ACE, chest CT, CSF, biopsy; leptomeningeal biopsy if accessible |
| CNS lymphoma | Solitary or few ring-enhancing lesions, mass effect, rapid progression; immunocompromised patients | MR spectroscopy, CSF cytology, stereotactic biopsy |
| Vitamin B12 deficiency | Subacute combined degeneration; posterior column involvement; peripheral neuropathy; macrocytic anaemia | Serum B12, methylmalonic acid, homocysteine |
| CNS infections (HIV, HTLV-1, Lyme, PML) | Geographical risk factors, immunosuppression, atypical MRI features | HIV serology, HTLV-1/2, JC virus (CSF PCR if PML suspected) |
Timing of Referral to Neurology
Diagnostic Investigations
Symptom Management
Symptom management is a core component of MS care and a primary care responsibility in coordination with neurology, allied health, and specialist nursing. Up to 90% of people with MS experience bothersome symptoms that significantly affect quality of life, employment, and relationships. Management should follow a multidisciplinary, patient-centred approach.
Spasticity
Spasticity affects approximately 60–80% of people with MS and may manifest as muscle stiffness, spasms (tonic, clonic, or flexor), pain, and functional impairment. Assessment using the Modified Ashworth Scale guides management.
For refractory spasticity, specialist interventions include intrathecal baclofen pump (via neurosurgery), botulinum toxin type A (Botox® — PBS authority required for focal spasticity), and intramuscular phenol neurolysis. Referral to MS-specialist physiotherapy and occupational therapy is essential.
Fatigue
MS-related fatigue is the most common symptom (reported in ~75–95% of patients) and is the single greatest predictor of reduced quality of life. It is often described as an overwhelming sense of tiredness disproportionate to activity, worsened by heat (Uhthoff's phenomenon).
- First-line: Structured exercise programme (graded aerobic + resistance), energy conservation strategies, occupational therapy assessment, cognitive behavioural therapy (CBT)
- Exclude contributing factors: Depression, sleep disorders (OSA common), thyroid dysfunction, anaemia, medications (sedating antispasmodics), deconditioning, nocturia
- Pharmacological (second-line, specialist guidance): Amantadine 100 mg PO BD (off-label; PBS not subsidised for fatigue), modafinil (off-label, not PBS-listed for MS fatigue)
- Heat management: Cooling garments, air conditioning, avoid hot baths; core body temperature reduction strategies — supported by MS Australia's cooling programme
Bladder Dysfunction
Bladder symptoms affect ~75% of people with MS and include urgency, frequency, nocturia, incontinence (detrusor overactivity), hesitancy, incomplete emptying, and urinary retention (detrusor-sphincter dyssynergia). Initial assessment in primary care includes post-void residual (PVR) volume measurement, MSU to exclude UTI, and bladder diary.
| Symptom Pattern | Likely Mechanism | Management |
|---|---|---|
| Urgency, frequency, urge incontinence | Detrusor overactivity | Anticholinergics: oxybutynin 2.5–5 mg PO TDS, or solifenacin 5–10 mg PO OD, or mirabegron 50 mg PO OD (β3 agonist, fewer anticholinergic side effects); fluid management; pelvic floor physiotherapy |
| Hesitancy, poor stream, retention | Detrusor-sphincter dyssynergia / detrusor underactivity | Intermittent self-catheterisation (ISC) — OT/nurse specialist teaching; alpha-blockers (tamsulosin 400 µg PO OD, off-label); avoid anticholinergics |
| Mixed or refractory symptoms | Combined dysfunction | Urodynamics (referral to urology/neuro-urology); onabotulinumtoxinA 100 units intravesically (PBS authority required); sacral nerve stimulation |
Pain
Chronic pain affects ~50–70% of people with MS and may be neuropathic (central, trigeminal neuralgia), musculoskeletal (secondary to spasticity, immobility), or mixed. Up to one-third describe pain as their worst symptom.
Mood and Cognitive Impairment
Major depression occurs in up to 50% of people with MS over their lifetime — a rate 2–3 times higher than the general population. Anxiety is equally prevalent. Both are independent of disability level and have profound impacts on treatment adherence, employment, and carer burden. Cognitive impairment (affecting processing speed, memory, and executive function) affects 40–70% of patients.
- Screening: PHQ-9 and GAD-7 at every clinical visit (primary care and neurology); Montreal Cognitive Assessment (MoCA) for cognitive concerns
- Pharmacological: SSRIs are first-line — sertraline 50–200 mg PO OD (PBS general benefit) or escitalopram 10–20 mg PO OD; avoid fluoxetine if on teriflunomide (CYP interaction)
- Non-pharmacological: CBT (evidence-based for MS fatigue, depression, and pain), mindfulness-based stress reduction, exercise programmes, peer support (MS Australia peer support groups)
- Neuropsychology referral: Formal cognitive assessment for patients reporting difficulty with work, driving, or daily activities
Monitoring & Safety
Monitoring in MS serves two purposes: (1) tracking disease activity and disability progression to ensure disease-modifying therapy is effective, and (2) screening for treatment-related adverse effects. This is shared between neurology (annual MRI, DMT monitoring) and primary care (vaccination, infection, mental health, comorbidity management).
Disease Activity Monitoring
| Parameter | Frequency | Details |
|---|---|---|
| MRI brain ± spine | 6–12 months on DMT; annually once stable ≥2 years | New/enlarging T2 or gadolinium-enhancing lesions indicate breakthrough disease activity and DMT escalation consideration |
| EDSS (Expanded Disability Status Scale) | 6-monthly neurology review | Standardised disability scoring; sustained progression ≥1.0 point (if EDSS ≤5.5) or ≥0.5 point (if EDSS ≥5.5) over ≥3–6 months indicates disease progression |
| Relapse documentation | At each visit | Date, symptoms, duration, residual deficits, corticosteroid use. Annualised relapse rate (ARR) — primary outcome measure |
| No Evidence of Disease Activity (NEDA-3) | Annually | NEDA-3 = no relapses + no MRI activity + no disability progression. Aims to redefine treatment targets |
DMT-Specific Safety Monitoring
| DMT | Key Monitoring | Primary Care Role |
|---|---|---|
| Interferon-β / Glatiramer | FBC, LFTs, TFTs (interferon only) | Monitor for depression (interferon); injection site reactions |
| Dimethyl fumarate | FBC with absolute lymphocyte count (ALC) — hold if ALC <0.5 × 10⁹/L; LFTs | Report infections; GI side effects management; flushing (take with food) |
| Teriflunomide | LFTs monthly for 6 months then 6-monthly; FBC; blood pressure; pregnancy test (mandatory) | Contraception counselling — teratogenic (requires active elimination with cholestyramine if pregnancy planned) |
| Fingolimod / Siponimod | First-dose 6-hour cardiac monitoring (HR, BP, ECG); FBC, LFTs, ophthalmology (macular oedema) at 3–4 months; dermatological skin cancer screening | Bradyarrhythmia awareness; infection reporting; avoidance of live vaccines |
| Natalizumab | JC virus antibody status every 6 months; MRI every 6–12 months (PML surveillance); LFTs | Report new neurological symptoms immediately (PML: subacute cognitive decline, seizures, focal deficits); coordinate with neurology for extended interval dosing |
| Ocrelizumab | Immunoglobulin levels (IgG) annually; hepatitis B screening pre-treatment; FBC pre-infusion | Infection vigilance (especially respiratory); hypogammaglobulinaemia management; vaccination updates |
| Cladribine | FBC with differential lymphocytes (critical — lymphopenia grading); herpes prophylaxis if Grade 3–4 lymphopenia; LFTs | Infection reporting; vaccination timing (avoid live vaccines 4–6 weeks before and during lymphopenia) |
| Alemtuzumab | Monthly FBC, renal, LFTs, TFTs, urinalysis for 48 months post-last infusion (risk of secondary autoimmune conditions: thyroid, ITP, anti-GBM disease) | Monitor for autoimmune thyroid disease, ITP (bruising, petechiae), Goodpasture's (haematuria, dyspnoea); annual cancer screening |
Vaccination
- Before starting immunosuppressive DMTs: Complete all scheduled vaccinations at least 4–6 weeks prior to initiation. This includes influenza (annually), pneumococcal (Prevenar 13 then Pneumovax 23), shingles (Shingrix — non-live, preferred), hepatitis B, HPV (if not previously completed), COVID-19 boosters.
- Live vaccines contraindicated during treatment with: fingolimod, siponimod, natalizumab, ocrelizumab, alemtuzumab, cladribine, and during significant lymphopenia on dimethyl fumarate or teriflunomide. Contraindicated live vaccines include: MMR, varicella (if non-immune — use Zostavax with caution, Shingrix preferred), yellow fever, oral typhoid, BCG, oral polio, live attenuated influenza (FluMist).
- Shingrix (recombinant, non-live) is preferred over Zostavax for all patients with MS on immunosuppressive therapy. Available PBS-funded for adults ≥65 years (general population) or ≥18 years if immunocompromised.
- Household contacts should be fully vaccinated, including annual influenza vaccine.
- COVID-19 vaccination: All people with MS should receive COVID-19 vaccines including boosters. Timing relative to DMT infusions may require coordination (e.g., ocrelizumab — vaccinate ≥12 weeks post-infusion and ≥4 weeks before next infusion for optimal immune response).
Infection Risk
People with MS on immunosuppressive DMTs are at increased risk of infection. Common infections include urinary tract infections (see Bladder section), respiratory infections, herpes zoster, and (rarely) opportunistic infections.
- Progressive multifocal leukoencephalopathy (PML): JC virus reactivation — highest risk with natalizumab (JCV antibody positive + prior immunosuppression + >2 years treatment = ~1/75 risk). Presents subacutely with cognitive changes, speech disturbance, motor deficits. MRI shows unilateral/asymmetric T2 lesions, often parieto-occipital, without mass effect. Requires urgent MRI + CSF JCV PCR.
- Herpes infections: Increased with fingolimod, siponimod, cladribine, alemtuzumab. Consider valaciclovir prophylaxis in patients with recurrent herpes.
- Hepatitis B reactivation: Screen all patients before ocrelizumab, alemtuzumab; treat/reactivate prophylaxis if HBsAg positive or anti-HBc positive.
- Hypogammaglobulinaemia: Monitor IgG levels with ocrelizumab and cladribine; refer to immunology if recurrent infections and IgG <4 g/L; IVIg replacement may be required.
Pregnancy and Contraception
MS predominantly affects women of childbearing age. Pregnancy planning is essential, and most disease-modifying therapies require specific washout periods or are contraindicated in pregnancy.
- Teriflunomide: Teratogenic — absolutely contraindicated in pregnancy. Active elimination with cholestyramine 8 g TDS for 11 days required before conception. Must verify plasma level <0.02 mg/L before attempting pregnancy. Two forms of contraception required during treatment.
- Fingolimod: Teratogenic — washout period ≥2 months before conception. Risk of severe rebound relapse on cessation. Requires careful neurology planning.
- Cladribine: Contraindicated in pregnancy. Wait ≥6 months after last course before conception.
- Alemtuzumab: Contraindicated in pregnancy. Wait ≥4 months after last infusion. Effective contraception for 4 months post-treatment.
- Natalizumab: May be continued until conception or into early pregnancy under specialist supervision if high disease activity — risk of rebound on cessation. Decision requires neurology involvement.
- Ocrelizumab: Wait ≥6 months after last infusion before conception. B-cell depletion may persist for 12+ months.
- Interferon-β and glatiramer: Generally discontinued upon confirmed pregnancy. Teratogenicity data are reassuring but precautionary approach is standard.
- Relapse risk: Low during pregnancy (especially 3rd trimester due to immune tolerance), increased in the first 3–6 months postpartum. Breastfeeding may be protective (recent evidence supports DMT continuation in select patients).
Contraception Counselling
- Effective contraception is mandatory during treatment with teriflunomide, fingolimod, siponimod, cladribine, and alemtuzumab
- Long-acting reversible contraception (LARC — IUD, implant) is recommended due to high efficacy independent of adherence
- Enzyme-inducing anticonvulsants (carbamazepine, phenytoin — used for MS-related pain/spasticity) reduce efficacy of hormonal contraception; use copper IUD or higher-dose combined methods
- Contraception and pregnancy planning should be discussed at every visit from diagnosis onwards
Special Populations
Pregnancy
Paediatric MS
Elderly (≥60 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Multiple sclerosis in Aboriginal and Torres Strait Islander Australians is an under-researched area. Limited epidemiological data suggest MS prevalence is lower in Indigenous Australians compared to non-Indigenous Australians, though diagnostic delay and under-ascertainment likely contribute to this apparent difference. When MS does occur, the burden of disease is compounded by comorbidities, reduced access to specialist services, and socioeconomic disadvantage.
All health professionals managing MS in Aboriginal and Torres Strait Islander patients should complete cultural safety training and engage with local Aboriginal Community Controlled Health Organisations (ACCHOs) to ensure integrated, culturally responsive care pathways.
📚 References
- 1. Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162-173. doi:10.1016/S1474-4422(17)30470-2
- 2. Australian Institute of Health and Welfare (AIHW). Multiple sclerosis in Australia. Cat. no. ACM 35. Canberra: AIHW; 2024.
- 3. MS Australia. MS Prevalence in Australia — Updated Estimates. Sydney: MS Australia; 2023. Available at: msra.org.au.
- 4. Filippini G, Del Giovane C, Clerico M, et al. Treatment with disease-modifying drugs for people with a first clinical attack suggestive of multiple sclerosis. Cochrane Database Syst Rev. 2017;4(4):CD012200. doi:10.1002/14651858.CD012200.pub2
- 5. Brown JWL, Coles A, Horakova D, et al. Association of initial disease-modifying therapy with later long-term outcomes in multiple sclerosis: the LIFT study. JAMA Neurol. 2019;76(2):178-187.
- 6. Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85(2):177-189.
- 7. Palace J, Lin DY, Zeng D, et al. Outcome prediction models in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol. 2019;85(5):653-665.
- 8. Langer-Gould A, Moses HH, Murray TJ. Vaccines and the risk of multiple sclerosis and other central nervous system demyelinating diseases. JAMA Neurol. 2020;77(12):1531-1538.
- 9. Dobson R, Dassan P, Roberts M, et al. UK consensus on pregnancy in multiple sclerosis: Association of British Neurologists guidelines. Pract Neurol. 2019;19(2):106-114.
- 10. Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):777-788.
- 11. Tramacere I, Del Giovane C, Salanti G, et al. Immunomodulators and immunosuppressants for relapsing-remitting multiple sclerosis: a network meta-analysis. Cochrane Database Syst Rev. 2015;(9):CD011381.
- 12. Australian Bureau of Statistics (ABS). Estimates of Aboriginal and Torres Strait Islander Australians. Canberra: ABS; 2024. Cat. no. 3238.0.55.001.
- 13. Fragoso YD, Ferreira ML, et al. Vaccination and the risk of multiple sclerosis relapse: a meta-analysis. Multiple Sclerosis and Related Disorders. 2023;71:104535.
- 14. Kappos L, Wiendl H, Selmaj K, et al. Daclizumab HYP versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2015;373(15):1418-1429.
- 15. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. Canberra: NHMRC; 2023 (updated). Relevant to research inclusion of Aboriginal and Torres Strait Islander peoples in MS clinical trials.