📋 Key Information Summary
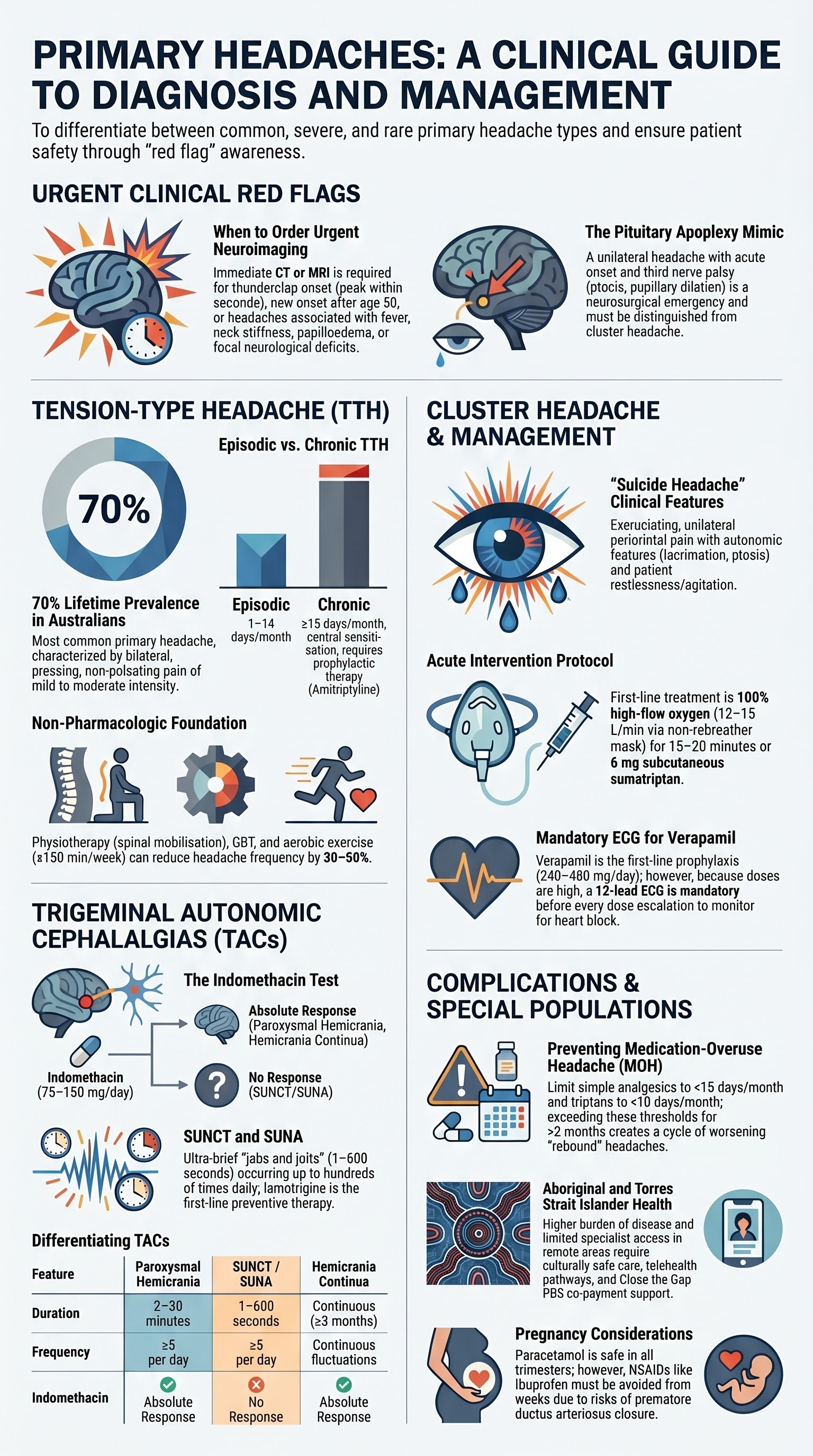
- Tension-type headache (TTH) is the most common primary headache worldwide, affecting up to 70% of Australians at some point in their lives; it is subdivided into infrequent episodic, frequent episodic, and chronic TTH.
- Simple analgesics (paracetamol, aspirin, ibuprofen, naproxen) are first-line for acute episodic TTH; limit use to <15 days/month to prevent medication-overuse headache (MOH).
- Chronic TTH (≥15 headache days/month) requires prophylaxis — amitriptyline 10–75 mg nocte is first-line, combined with non-pharmacologic strategies (physiotherapy, cognitive-behavioural therapy, stress management).
- Cluster headache is characterised by strictly unilateral, excruciating periorbital or temporal pain with ipsilateral autonomic features (lacrimation, rhinorrhoea, ptosis, miosis) and restlessness or agitation.
- Acute cluster attacks respond best to high-flow oxygen (100% at 12–15 L/min via non-rebreather mask for 15–20 minutes) and/or subcutaneous sumatriptan 6 mg.
- Verapamil is the first-line prophylactic agent for cluster headache; start at 80 mg TDS and titrate upward with mandatory ECG monitoring at each dose escalation.
- Transitional corticosteroids (prednisolone 1 mg/kg/day, tapered over 2–3 weeks) bridge the gap while verapamil is being titrated to therapeutic doses.
- Paroxysmal hemicrania and hemicrania continua are defined by their dramatic and absolute response to indomethacin — this is both diagnostic and therapeutic.
- SUNCT and SUNA are rare trigeminal autonomic cephalalgias with very brief (1–600 seconds) attacks; lamotrigine is first-line preventive therapy; referral to a headache specialist is mandatory.
- Always exclude secondary causes with urgent neuroimaging when red flags are present — new-onset headache after age 50, thunderclap onset, focal neurological signs, systemic symptoms, or papilloedema.
- Assess headache-related disability using validated tools (HIT-6, MIDAS) and screen for medication overuse at every review.
- Aboriginal and Torres Strait Islander populations experience higher headache burden with reduced access to specialist services; culturally safe care and telehealth pathways are essential.
Introduction & Australian Epidemiology
Primary headaches are neurological disorders in which the headache itself is the disease, not a symptom of an underlying condition. The International Classification of Headache Disorders, 3rd edition (ICHD-3) provides the standard diagnostic framework. The three major groups of primary headache — tension-type headache, migraine, and the trigeminal autonomic cephalalgias (TACs) — account for the vast majority of presentations in Australian primary care.
In Australia, headache disorders are among the most common reasons for general practice consultation. The Australian Institute of Health and Welfare (AIHW) reports that approximately 4.9 million Australians live with chronic headache, and headache-related productivity losses exceed $35 billion annually. Tension-type headache affects an estimated 40–70% of the adult population, while cluster headache has a lifetime prevalence of approximately 0.1–0.2%. The rarer TACs — paroxysmal hemicrania, SUNCT, SUNA, and hemicrania continua — are frequently misdiagnosed, often years after onset.
This guideline addresses tension-type headache, cluster headache, and the other trigeminal autonomic cephalalgias. Migraine is covered in a separate dedicated article.
Pathophysiology of Primary Headaches
Understanding the distinct pathophysiology of each primary headache type guides rational therapy and explains why treatments are not interchangeable.
Tension-Type Headache
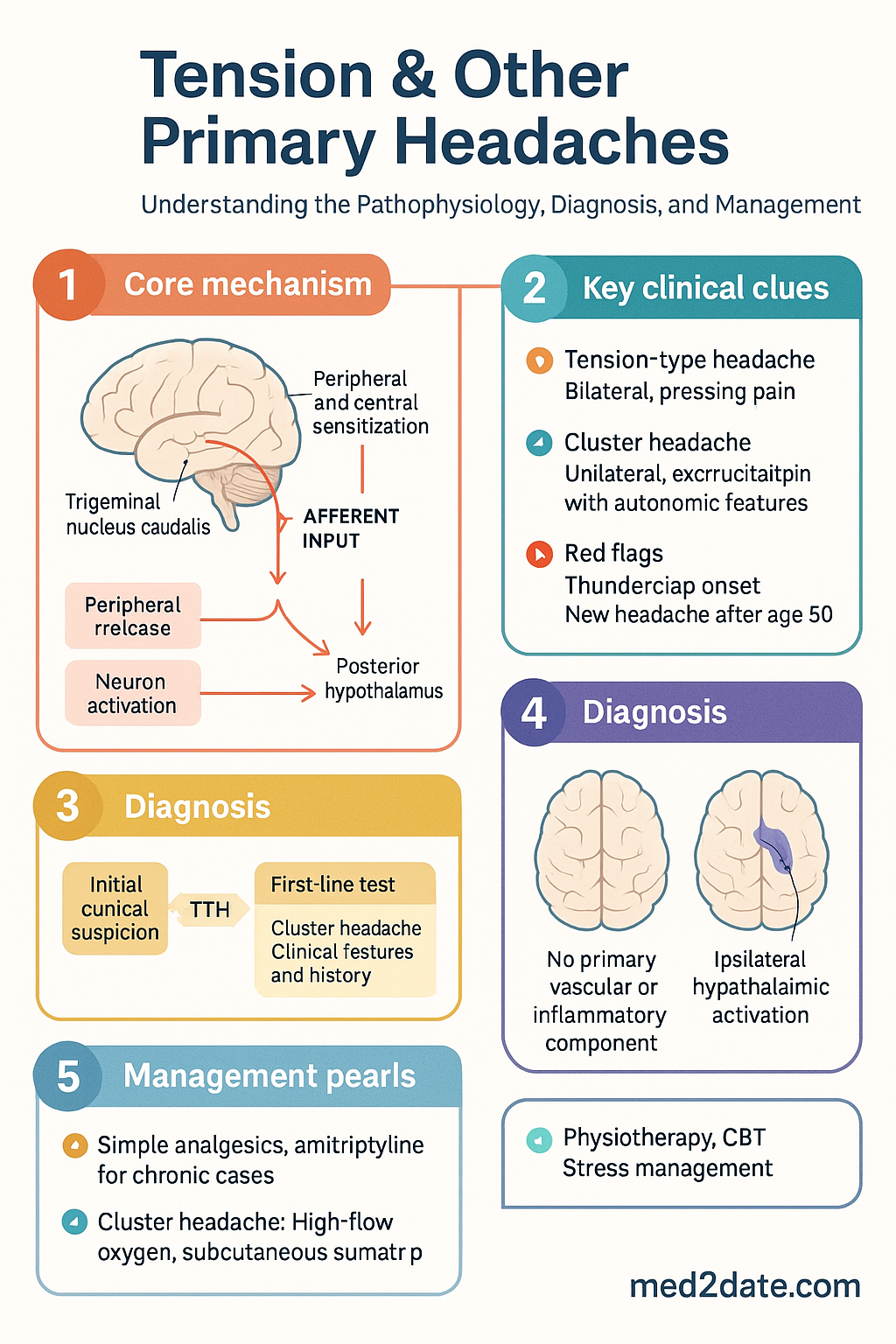
The pathophysiology of TTH involves a combination of peripheral and central sensitisation. In episodic TTH, peripheral mechanisms predominate — increased pericranial myofascial tenderness due to sustained muscle contraction, stress, and poor posture. In chronic TTH, central sensitisation of second-order neurons in the trigeminal nucleus caudalis becomes the dominant mechanism, lowering pain thresholds and converting innocuous input into pain. There is no evidence of a primary vascular or inflammatory component, distinguishing TTH from migraine and cluster headache.
Cluster Headache & Trigeminal Autonomic Cephalalgias
The TACs share a common pathophysiological pathway involving activation of the trigeminal-autonomic reflex. Trigeminal afferents (predominantly the ophthalmic division, V1) project to the trigeminal nucleus caudalis, which connects to the superior salivatory nucleus, producing parasympathetic autonomic features (lacrimation, rhinorrhoea, conjunctival injection). In cluster headache, the posterior hypothalamus (the "pain clock") plays a pivotal role, explaining the striking circadian and circannual periodicity. Functional imaging studies demonstrate ipsilateral hypothalamic activation during attacks. Paroxysmal hemicrania and hemicrania continua appear to involve similar circuitry, though the exact anatomical substrates differ.
Tension-Type Headache
Diagnostic Criteria (ICHD-3)
Tension-type headache is classified into three subtypes based on attack frequency. All subtypes share the following core features:
| Feature | Requirement |
|---|---|
| Duration | 30 minutes to 7 days |
| Character | Pressing or tightening (non-pulsating) |
| Location | Bilateral (frontal, temporal, occipital, or generalised) |
| Intensity | Mild to moderate (not preventing daily activities) |
| Aggravation | Not aggravated by routine physical activity |
| Nausea/Vomiting | Absent (nausea only = exclusion criterion) |
| Photo-/Phonophobia | Only one may be present (never both) |
Non-Pharmacologic Management
Non-pharmacologic strategies are foundational in TTH management, particularly for frequent episodic and chronic subtypes. They reduce headache frequency by 30–50% and are free of adverse effects.
- Physiotherapy: Cervical and thoracic spinal mobilisation, postural correction, and targeted stretching of the cervical flexors, upper trapezius, and suboccipital muscles. Referral to a physiotherapist experienced in headache management is recommended (Medicare Chronic Disease Management items available under GP Management Plan).
- Cognitive-behavioural therapy (CBT): Stress management, relaxation training (progressive muscle relaxation, diaphragmatic breathing), and biofeedback. Evidence supports CBT as equivalent to pharmacotherapy for chronic TTH prevention.
- Exercise: Regular aerobic exercise (≥150 minutes/week of moderate-intensity activity) reduces headache frequency. Exercise releases endorphins and reduces pericranial muscle tension.
- Ergonomic assessment: Correction of workstation setup, screen positioning, and avoidance of sustained static postures (particularly relevant for office workers and students).
- Sleep hygiene: Regular sleep–wake cycle, avoidance of excessive caffeine (≤200 mg/day), and treatment of comorbid insomnia or sleep-disordered breathing.
Acute Pharmacotherapy — Simple Analgesics
Simple analgesics are the mainstay of acute TTH treatment. They should be taken at the onset of headache for maximum effect and limited to ≤15 days/month to prevent medication-overuse headache.
Chronic Tension-Type Headache — Prophylactic Protocols
When headache frequency reaches ≥15 days/month, or when acute analgesic overuse is developing, prophylactic therapy should be initiated alongside non-pharmacologic strategies.
Other agents with evidence in chronic TTH include mirtazapine (15–30 mg nocte, useful when coexistent insomnia or depression), and topiramate (off-label, specialist use). The combination of amitriptyline with a non-pharmacologic program (CBT + physiotherapy) is superior to either strategy alone.
Cluster Headache
Clinical Features (ICHD-3 Code 3.1)
Cluster headache is among the most severe pain conditions known to medicine. It predominantly affects males (male-to-female ratio approximately 3:1), typically begins between ages 20 and 40, and is characterised by recurrent, stereotyped bouts (clusters) of attacks.
| Feature | Cluster Headache |
|---|---|
| Pain quality | Stabbing, drilling, excruciating (often described as "like a hot poker in the eye") |
| Location | Strictly unilateral — orbital, supraorbital, or temporal (side usually fixed within a cluster period) |
| Intensity | Severe to very severe; patients are restless, pace, rock, or bang their head |
| Duration | 15–180 minutes (mean 60–90 minutes) |
| Frequency | 1 every other day to 8 per day; often nocturnal (attacks wake patient from sleep) |
| Autonomic features | Ipsilateral lacrimation, conjunctival injection, nasal congestion, rhinorrhoea, eyelid oedema, facial sweating, miosis, ptosis (Horner syndrome) |
| Behaviour | Restlessness and agitation (distinguishes from migraine, where patients prefer to lie still) |
Acute Therapy — Oxygen
Acute Therapy — Triptans
Oral triptans are generally not recommended for cluster headache due to slow onset of action (attacks are too short). However, oral sumatriptan 100 mg may be useful as an adjunct when attacks are longer in duration. Intranasal sumatriptan 20 mg is another option but inferior to the SC and zolmitriptan nasal formulations.
Prophylaxis — Verapamil
Transitional (Bridge) Therapy — Corticosteroids
Corticosteroids provide rapid suppression of cluster attacks within 24–72 hours. They serve as a bridge while verapamil is being titrated to therapeutic doses (a process that takes 4–6 weeks).
Greater occipital nerve (GON) injection — An alternative or adjunct to systemic corticosteroids. Injection of bupivacaine (0.5%, 2–3 mL) combined with triamcinolone (40 mg) at the ipsilateral greater occipital nerve provides relief in approximately 60% of patients. Duration of effect is 4–8 weeks. This procedure can be performed in primary care by an experienced GP or in a headache clinic.
Other Preventive Agents
When verapamil alone is insufficient or not tolerated:
- Lithium carbonate (250–750 mg/day, target serum level 0.4–0.8 mmol/L): Second-line, particularly for chronic cluster headache. Requires renal and thyroid monitoring.
- Melatonin (10–20 mg nocte): May be useful as adjunctive therapy, particularly for nocturnal attacks. Minimal side effects. Available without prescription.
- Galcanezumab (Emgality® 300 mg SC monthly): TGA-approved for episodic cluster headache in Australia. Monoclonal anti-CGRP antibody. PBS listing: Authority Required (Specialist). Reserved for patients intolerant or refractory to verapamil.
- Greater occipital nerve blocks: Repeated monthly during cluster periods as a non-systemic adjunct.
Other Trigeminal Autonomic Cephalalgias
The trigeminal autonomic cephalalgias (TACs) are a group of primary headache disorders characterised by unilateral trigeminal distribution pain with ipsilateral cranial autonomic features. While cluster headache is the most common TAC, several rarer entities are frequently misdiagnosed, often for years. Accurate diagnosis is critical because treatment differs fundamentally from cluster headache and migraine.
| Feature | Paroxysmal Hemicrania | SUNCT / SUNA | Hemicrania Continua |
|---|---|---|---|
| ICHD-3 code | 3.2 | 3.3 / 3.4 | 3.5 |
| Pain severity | Severe, excruciating | Moderate to severe | Moderate baseline with severe exacerbations |
| Location | Unilateral — orbital, supraorbital, temporal | Unilateral — orbital/periorbital/temporal | Unilateral — frontotemporal |
| Attack duration | 2–30 minutes | 1–600 seconds (SUNCT); variable (SUNA) | Continuous (≥3 months), with fluctuations |
| Frequency | ≥5/day (>half the time) | ≥5/day (SUNCT); ≥1/day typical (SUNA) | Continuous, with superimposed attacks |
| Autonomic features | Prominent — lacrimation, rhinorrhoea, conjunctival injection, ptosis, miosis | SUNCT: ≥2 autonomic features. SUNA: limited (e.g., only lacrimation or conjunctival injection) | Present — ipsilateral lacrimation, conjunctival injection, nasal congestion, restlessness |
| Behaviour | Restlessness/agitation during attacks | No restlessness (brief attacks) | Mild restlessness during exacerbations |
| Indomethacin response | Absolute — diagnostic and therapeutic | No response | Absolute — diagnostic and therapeutic |
| Sex predominance | F > M (2:1) | M > F (SUNCT); equal (SUNA) | F > M |
Paroxysmal Hemicrania — Indomethacin Trial
Paroxysmal hemicrania (PH) is defined by its absolute and complete response to therapeutic doses of indomethacin. The indomethacin trial is therefore both diagnostic and therapeutic — if a patient with suspected PH does not respond to indomethacin, the diagnosis should be reconsidered.
SUNCT and SUNA
SUNCT (Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing) and SUNA (with Autonomic features) are the rarest and most challenging TACs to treat. Attacks are extremely brief (1–600 seconds) but may cluster into "jabs and jolts" occurring hundreds of times per day.
- SUNCT requires both conjunctival injection AND tearing; SUNA may feature only one autonomic sign.
- First-line preventive: Lamotrigine (start 25 mg/day, titrate to 100–200 mg/day over 4–6 weeks).
- Second-line preventives: Carbamazepine (200–800 mg/day), topiramate (50–200 mg/day), gabapentin (900–2400 mg/day).
- Acute treatment: IV lidocaine (1–2 mg/kg/hour, specialist setting only) may break prolonged exacerbations.
- Non-pharmacologic: Greater occipital nerve blocks may provide temporary relief. Occipital nerve stimulation is under investigation.
Hemicrania Continua
Hemicrania continua (HC) is a continuous, strictly unilateral headache with superimposed exacerbations and ipsilateral autonomic features. It responds absolutely to indomethacin, similar to paroxysmal hemicrania. Distinguish from chronic migraine and new daily persistent headache by the unilateral nature and autonomic features.
- Continuous unilateral headache for ≥3 months with fluctuations.
- Complete response to indomethacin at standard doses (75–150 mg/day).
- If indomethacin cannot be tolerated long-term, melatonin (9–12 mg/day), topiramate, or celecoxib may provide partial relief, but no other agent reliably reproduces the indomethacin effect.
Referral Indications
Investigations & Red-Flag Exclusion
The diagnosis of all primary headaches is clinical. Neuroimaging is indicated only when red flags are present or the diagnosis is atypical.
Headache Disability & Severity Assessment
Headache-related disability guides treatment intensity and monitors response. Use validated tools at baseline and every 3–6 months:
| Tool | Application | Scoring |
|---|---|---|
| HIT-6 (Headache Impact Test) | All primary headaches; 6-item questionnaire | 36–49: little impact; 50–55: some; 56–59: substantial; ≥60: severe impact |
| MIDAS (Migraine Disability Assessment) | Primarily migraine/TTH; measures days lost from work, household, social activities | 0–5: minimal; 6–10: mild; 11–20: moderate; ≥21: severe disability |
| Headache diary | All headaches; tracks frequency, severity, acute medication use, triggers | Essential for detecting medication overuse and monitoring prophylactic response |
Monitoring & Medication-Overuse Prevention
Follow-Up Schedule
Medication-Overuse Headache (MOH) Prevention
MOH is the most common complication of primary headache management. Prevention is always preferable to treatment.
- Simple analgesics (paracetamol, aspirin, NSAIDs): ≥15 days/month for >3 months
- Triptans: ≥10 days/month for >3 months
- Combination analgesics, opioids, or ergotamines: ≥10 days/month for >3 months
Management: Complete withdrawal of the overused agent. Explain that headache will worsen for 2–4 weeks before improving. Bridge with naproxen 500 mg BD or prednisolone taper. Initiate prophylaxis (amitriptyline) simultaneously. Follow up weekly during withdrawal.
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a higher burden of headache disorders compared to the non-Indigenous population, driven by higher rates of comorbidities (cardiovascular disease, diabetes, renal disease), psychosocial stressors, and reduced access to specialist neurological services. Culturally safe, person-centred care is essential.
Quick Reference — Acute Treatment Summary
📚 References
- 1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
- 2. Bendtsen L, Sacco S, Ashina M, et al. Guideline on the use of medication in tension-type headache: a European headache federation position paper. J Headache Pain. 2022;23(1):80.
- 3. Robbins MS, Starling AJ, Pringsheim TM, Becker WJ, Schwedt TJ. Treatment of cluster headache: the American Headache Society evidence-based guidelines. Headache. 2016;56(7):1093–1106.
- 4. May A, Schwedt TJ, Magis D, Pozo-Rosich P, Evers S, Wang SJ. Cluster headache. Nat Rev Dis Primers. 2018;4:18006.
- 5. Goadsby PJ, Cohen AS, Matharu MS. Trigeminal autonomic cephalalgias: diagnosis and treatment. Curr Neurol Neurosci Rep. 2007;7(2):117–125.
- 6. Cohen AS, Matharu MS, Goadsby PJ. Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) or cranial autonomic features (SUNA) — a prospective clinical study of SUNCT and SUNA. Brain. 2006;129(Pt 10):2746–2760.
- 7. Antonaci F, Sjaastad O. Chronic paroxysmal hemicrania (CPH): a review of the clinical manifestations. Headache. 1989;29(10):648–656.
- 8. Newman LC, Lipton RB, Solomon S. Hemicrania continua: ten new cases and a review of the literature. Neurology. 1994;44(11):2111–2114.
- 9. Australian Institute of Health and Welfare (AIHW). Headache and migraine in Australia. Cat. no. PHE 326. Canberra: AIHW; 2023.
- 10. Royal Australian College of General Practitioners (RACGP). Management of headache in primary care. Melbourne: RACGP; 2023.
- 11. Obermann M, Holle D. Cluster headache: from pathophysiology to new treatments. Curr Pain Headache Rep. 2023;27(4):57–67.
- 12. Mitsikostas DD, Ashina M, Craven A, et al. European Headache Federation consensus on technical investigation for primary headache disorders. J Headache Pain. 2016;17:5.
- 13. Bendtsen L, Jensen R. Tension-type headache — the most common, but also the most neglected, headache disorder. Curr Opin Neurol. 2006;19(3):305–309.
- 14. Paemeleire K, Bhatt DK, Ahn AH, et al. Pathophysiology of trigeminal autonomic cephalalgias — a comprehensive review. Lancet Neurol. 2019;18(8):784–796.
- 15. National Aboriginal Community Controlled Health Organisation (NACCHO). Providing culturally safe health care for Aboriginal and Torres Strait Islander peoples. Canberra: NACCHO; 2022.