📋 Key Information Summary
- Peripheral neuropathy affects approximately 2–8% of the Australian adult population; diabetic sensorimotor polyneuropathy is the most common cause encountered in primary care.
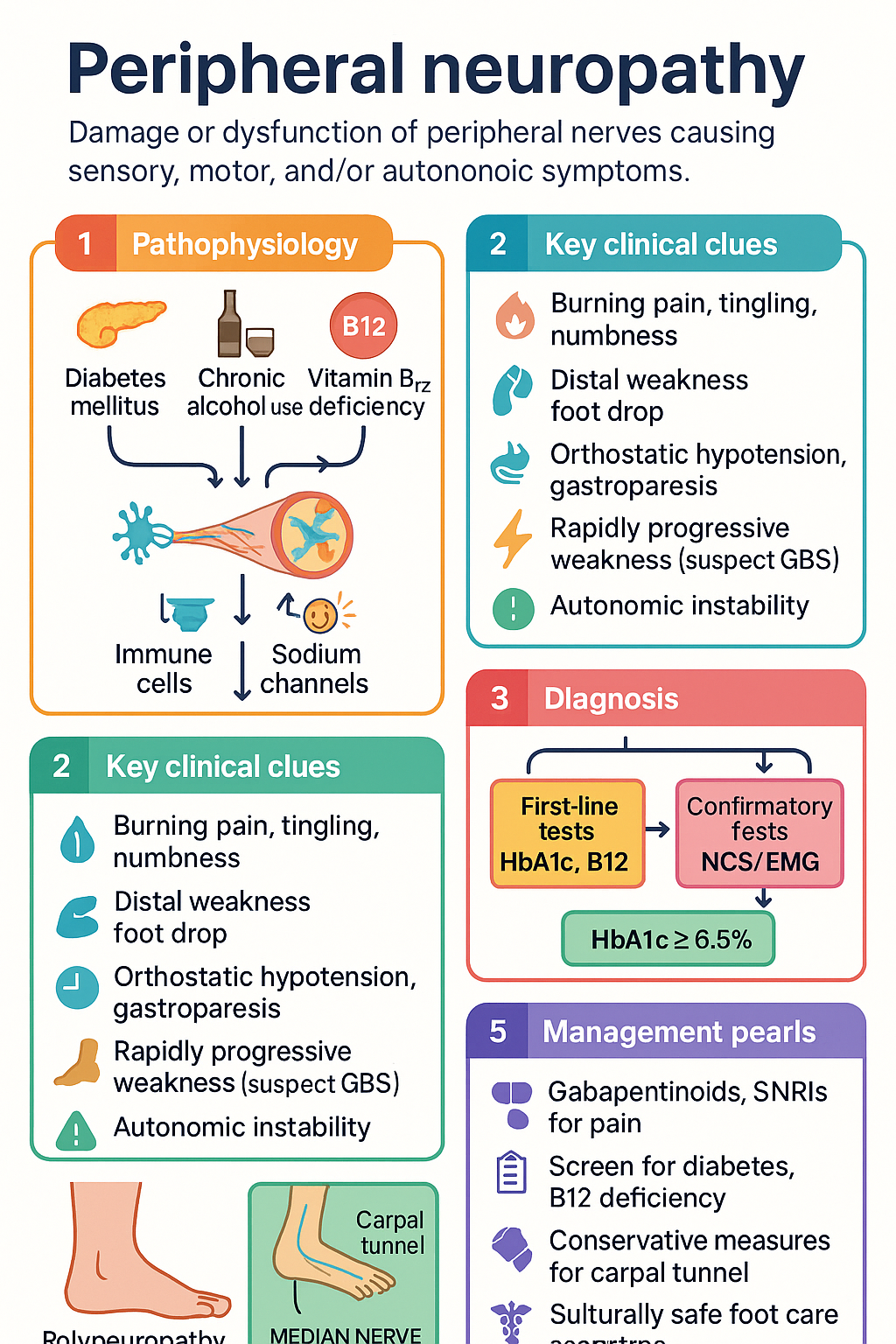
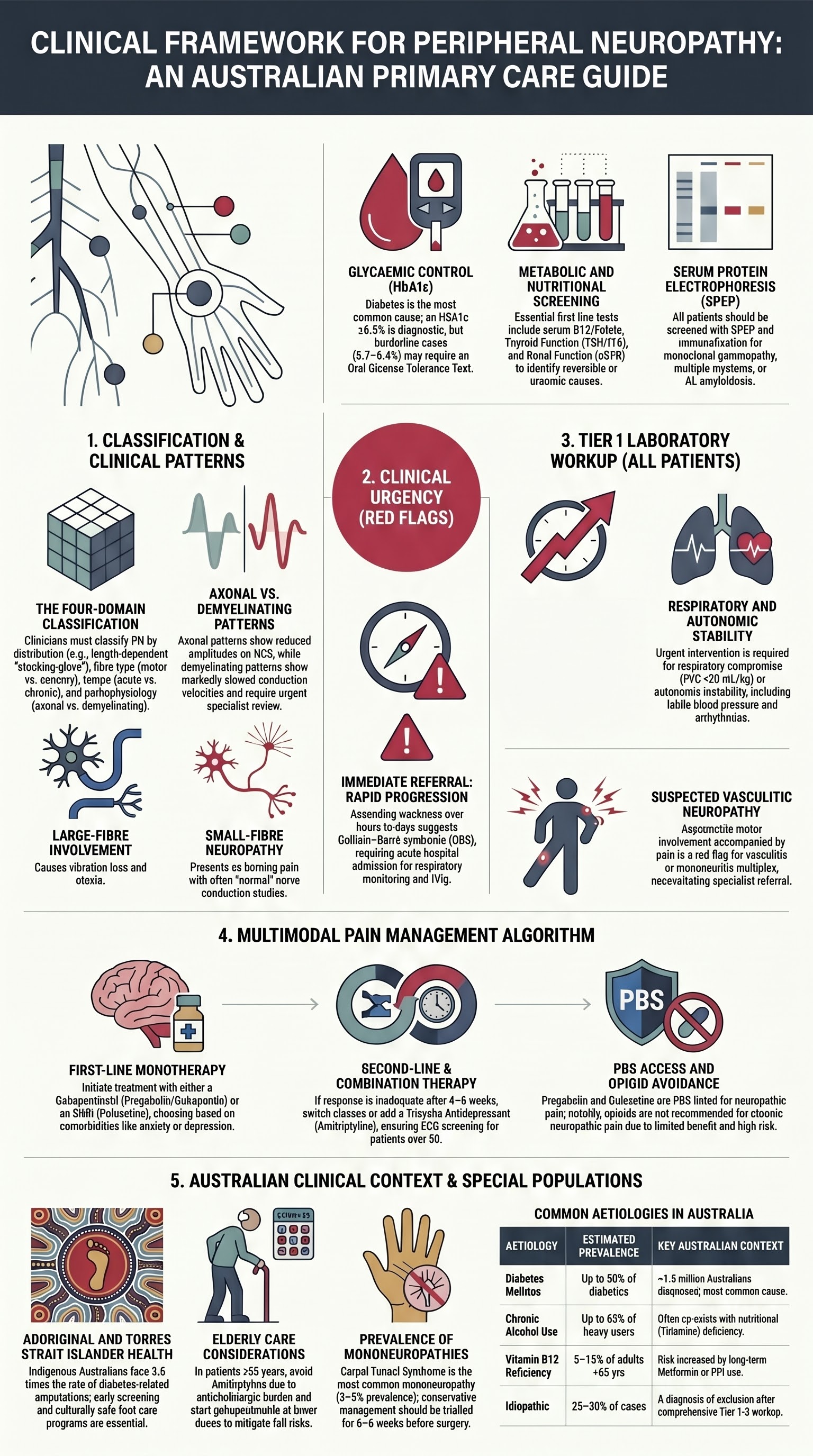
- Classify neuropathy by distribution (length-dependent vs multifocal vs focal), fibre type (motor, sensory, autonomic), tempo (acute, subacute, chronic), and pattern (axonal vs demyelinating) to guide investigations and management.
- Red flags requiring urgent referral: rapidly progressive weakness over days to weeks (suspect GBS), respiratory compromise, asymmetric motor involvement, autonomic instability, or suspected vasculitic neuropathy.
- Initial workup should include HbA1c/fasting glucose, serum B12 and folate, serum protein electrophoresis (SPEP), thyroid function, renal function (eGFR), full blood count, liver function tests, and autoimmune screening (ANA, anti-MAG, ANCA where indicated).
- Nerve conduction studies (NCS) and electromyography (EMG) are the gold standard for confirming peripheral neuropathy, distinguishing axonal from demyelinating patterns, and identifying focal compressive lesions (MBS item 11005).
- First-line analgesics for painful diabetic neuropathy are gabapentinoids (pregabalin, gabapentin) and SNRIs (duloxetine); both are PBS-listed for this indication in Australia.
- Tricyclic antidepressants (amitriptyline, nortriptyline) are effective second-line agents but carry significant anticholinergic burden — use with caution in patients aged >65 years and those with cardiac conduction abnormalities.
- Topical capsaicin 8% patch (Qutenza®) and lignocaine 5% patches are useful adjuncts for localised neuropathic pain; capsaicin requires PBS Authority approval for refractory cases.
- Carpal tunnel syndrome is the most common mononeuropathy; confirm with NCS/EMG before surgical referral. Conservative measures (splinting, ergonomic modification) should be trialled for at least 6–8 weeks before considering carpal tunnel release.
- Always screen for treatable aetiologies — particularly diabetes, B12 deficiency, hypothyroidism, and alcohol-related neuropathy — before attributing neuropathy to idiopathic causes.
- Assess for fall risk, foot ulceration, and autonomic symptoms (orthostatic hypotension, gastroparesis, erectile dysfunction) as these significantly affect morbidity in chronic peripheral neuropathy.
- Aboriginal and Torres Strait Islander Australians have higher rates of diabetes-related neuropathy; culturally safe foot care programmes and early screening are essential to reduce amputation rates.
Introduction & Australian Epidemiology
Peripheral neuropathy refers to damage or dysfunction of one or more peripheral nerves, producing sensory, motor, and/or autonomic symptoms. It represents one of the most common neurological presentations in Australian primary care and is a leading cause of morbidity, falls, foot ulceration, and impaired quality of life.
The prevalence of peripheral neuropathy in the general Australian population is estimated at 2–8%, rising sharply with age and the presence of diabetes mellitus. Diabetic peripheral neuropathy (DPN) affects up to 50% of individuals with type 2 diabetes during their lifetime, making it the most common cause in Australia. The Australian Institute of Health and Welfare (AIHW) reports that diabetes-related peripheral complications, including neuropathy, contribute significantly to the burden of preventable hospitalisations and lower-limb amputations, particularly among Aboriginal and Torres Strait Islander peoples.
Other common aetiologies encountered in Australian practice include chronic alcohol-related neuropathy, vitamin B12 deficiency (particularly in older adults and those on long-term metformin or proton pump inhibitors), chemotherapy-induced peripheral neuropathy (CIPN), chronic inflammatory demyelinating polyneuropathy (CIDP), and hereditary neuropathies such as Charcot–Marie–Tooth disease.
Early recognition, appropriate classification, and identification of reversible causes are the cornerstones of effective management. This guideline provides a structured approach to evaluation, investigation, and evidence-based management of peripheral neuropathy within the Australian healthcare context.
| Aetiology | Estimated Prevalence | Key Australian Context |
|---|---|---|
| Diabetes mellitus (type 1 & 2) | Up to 50% of people with diabetes | Most common cause; ~1.3 million Australians with diagnosed diabetes (NDSS 2023) |
| Chronic alcohol use | Up to 65% with heavy use | Often co-exists with nutritional deficiency |
| Vitamin B12 deficiency | 5–15% of adults >65 years | Risk increased with metformin and PPI use |
| Chemotherapy-induced (CIPN) | 30–70% depending on agent | Platinum agents, taxanes, vinca alkaloids most implicated |
| Chronic inflammatory demyelinating polyneuropathy (CIDP) | 1–9 per 100,000 | Treatable — IVIg PBS-listed for CIDP |
| Charcot–Marie–Tooth disease | ~1 in 2,500 | Most common inherited neuropathy; genetic testing available |
| Idiopathic | Up to 25–30% of cases | Diagnosis of exclusion after comprehensive workup |
Evaluation & Classification
A systematic approach to classifying peripheral neuropathy is essential for narrowing the differential diagnosis and guiding investigations. Classification should address four domains: distribution, fibre type involvement, tempo, and underlying pathophysiology.
Distribution Pattern
| Pattern | Description | Common Causes |
|---|---|---|
| Length-dependent (distal symmetric) | Symptoms begin in the feet and progress proximally in a "stocking-glove" distribution; hands involved once symptoms reach mid-calf level | Diabetes, alcohol, B12 deficiency, idiopathic, CIPN |
| Multifocal (mononeuritis multiplex) | Asymmetric involvement of individual peripheral nerves, often at separate anatomical sites; may become confluent over time | Vasculitis (e.g. PAN, EGPA), sarcoidosis, diabetes, HIV, leprosy |
| Focal (single nerve) | Isolated involvement of a single nerve with clear anatomical localisation | Compression (CTS, ulnar, peroneal), trauma, nerve infarction |
| Proximal and distal (generalised) | Diffuse involvement from outset with prominent proximal weakness | GBS, CIDP, paraneoplastic, critical illness polyneuropathy |
Fibre Type Involvement
- Large-fibre sensory: Vibration and proprioception loss, sensory ataxia, reduced reflexes, positive Romberg sign. Patients report numbness, unsteadiness, and difficulty with fine motor tasks.
- Small-fibre sensory: Burning pain, tingling, allodynia, and temperature sensation loss with preserved reflexes and normal NCS. Diagnosed clinically or with skin punch biopsy (intraepidermal nerve fibre density). Small-fibre neuropathy is increasingly recognised as a cause of burning feet with "normal" nerve conduction studies.
- Motor: Weakness, cramping, fasciculations, muscle wasting, and reduced or absent reflexes. Suggests anterior horn cell, motor root, plexus, or motor-predominant nerve pathology.
- Autonomic: Orthostatic hypotension, gastroparesis, bladder dysfunction, erectile dysfunction, gustatory sweating, resting tachycardia. Consider diabetic autonomic neuropathy, amyloidosis, or autoimmune autonomic ganglionopathy.
Tempo of Onset
- Acute (days to <4 weeks): Guillain–Barré syndrome (GBS), vasculitis, toxins, porphyria, diphtheria. Requires urgent hospital assessment.
- Subacute (4–8 weeks): CIDP, paraneoplastic, nutritional deficiency, toxic exposures, vasculitis.
- Chronic (>8 weeks): Diabetic neuropathy, hereditary neuropathies, chronic alcohol use, idiopathic. Most common pattern in general practice.
- Rapidly progressive ascending weakness over hours to days (suspect GBS) — admit acutely for respiratory monitoring and IVIg
- Respiratory compromise (forced vital capacity <20 mL/kg or declining FVC) — ICU transfer
- Asymmetric motor involvement with pain (suspect vasculitis or mononeuritis multiplex)
- Autonomic instability: labile blood pressure, cardiac arrhythmias, urinary retention
- Prominent proximal weakness with areflexia (suspect GBS, CIDP, or critical illness polyneuropathy)
- New-onset neuropathy in a patient with known malignancy (suspect paraneoplastic)
- Saddle anaesthesia with bladder/bowel dysfunction (consider cauda equina — not peripheral neuropathy, but an important differential)
Pathophysiology: Axonal vs Demyelinating
| Feature | Axonal | Demyelinating |
|---|---|---|
| NCS pattern | Reduced amplitudes, normal/mildly slowed conduction velocities | Markedly slowed conduction velocities, prolonged distal motor latencies, conduction block, temporal dispersion |
| Common causes | Diabetes, alcohol, B12 deficiency, toxins | GBS (AIDP), CIDP, anti-MAG neuropathy, CMT1 |
| Prognosis | Slow recovery (months to years); may be irreversible | Often treatable with immunotherapy; good prognosis if identified early |
| Key investigation | NCS/EMG, skin biopsy (small fibre) | NCS/EMG, CSF (elevated protein in GBS/CIDP), nerve biopsy rarely needed |
Initial Laboratory Workup
A structured tiered approach to investigation ensures that common, treatable causes are identified efficiently before progressing to specialist testing.
Tier 1 — First-Line Investigations (All Patients)
These tests should be ordered for every patient presenting with suspected peripheral neuropathy in primary care:
Tier 2 — Second-Line Investigations (Directed by Clinical Suspicion)
Tier 3 — Specialist Investigations
Clinical Presentation & Diagnostic Criteria
Symptoms
The clinical presentation of peripheral neuropathy depends on the fibre types affected and the distribution of nerve involvement. Patients commonly present with a combination of positive and negative symptoms:
- Positive sensory symptoms: Burning, tingling, "pins and needles," electric-shock sensations, allodynia (pain from non-painful stimuli), hyperalgesia. Often worse at night, disrupting sleep.
- Negative sensory symptoms: Numbness, "dead" feeling in feet, loss of temperature sensation, reduced proprioception leading to unsteadiness.
- Motor symptoms: Distal weakness (foot drop, difficulty rising from a chair), muscle wasting, cramps, fasciculations.
- Autonomic symptoms: Orthostatic dizziness, resting tachycardia, gastroparesis (early satiety, nausea), constipation or diarrhoea, erectile dysfunction, urinary retention, gustatory sweating, dry eyes/mouth.
Examination Findings
A focused neurological examination should assess:
- Sensation: Light touch (cotton wool), pinprick, vibration (128 Hz tuning fork on medial malleolus and great toe), proprioception (great toe), temperature (cold tuning fork or thermal roller).
- Reflexes: Ankle jerbs are typically the first to be lost in length-dependent neuropathy. Symmetrically absent ankle jerbs with preserved knee jerbs is a classic early finding.
- Motor: Great toe extension (L5 — extensor hallucis longus), foot dorsiflexion, toe walking, heel walking. Assess for interosseous wasting and pes cavus in chronic/hereditary cases.
- Gait and balance: Romberg test, tandem gait (heel-to-toe walking). Sensory ataxia worsens when visual input is removed.
- Autonomic: Lying and standing blood pressure (orthostatic drop ≥20 mmHg systolic or ≥10 mmHg diastolic), resting heart rate.
- Foot examination: Calluses, ulcers, Charcot deformity (rocker-bottom foot), dry/cracked skin, fungal infections. Monofilament testing (10 g Semmes–Weinstein) for diabetic screening — loss of sensation at ≥1 site indicates at-risk foot (MBS item 2401 for annual diabetic foot check).
Diagnostic Criteria for Common Presentations
Management of Painful Neuropathy
Painful peripheral neuropathy significantly impairs quality of life, sleep, mood, and functional capacity. Management should be multimodal, combining pharmacotherapy with non-pharmacological strategies and addressing comorbid sleep disturbance and mood disorders. The goal is ≥50% reduction in pain score (NRS/VAS) or meaningful improvement in function, with regular reassessment at 4–6 week intervals.
Pharmacological Management — Treatment Algorithm
First-Line Agents
Second-Line Agents
Topical Therapies
Sleep and Mood Considerations
- Sleep: Non-pharmacological measures include sleep hygiene education, cognitive behavioural therapy for insomnia (CBT-I), and avoiding daytime napping. Pregabalin and amitriptyline may improve sleep through their sedating properties. Avoid benzodiazepines and Z-drugs long-term.
- Depression/Anxiety: Duloxetine is the preferred agent when comorbid depression exists. Consider psychology referral (MBS items 80110/80115 for Mental Health Treatment Plan). Safety-net for suicidal ideation with regular follow-up.
- Exercise: Moderate-intensity aerobic exercise (≥150 minutes/week) improves neuropathic pain severity, mood, and cardiovascular fitness. Refer to exercise physiologist where available.
- Alcohol cessation: Essential in alcohol-related neuropathy; refer to addiction medicine or local alcohol and drug service. Thiamine replacement (100 mg PO BD) in addition to addressing nutrition.
Non-Pharmacological Approaches
- Transcutaneous electrical nerve stimulation (TENS): May provide short-term relief; minimal side effects. Available OTC. PBS not applicable.
- Physiotherapy and balance training: Reduces fall risk; important in sensory ataxia and large-fibre neuropathy. Physiotherapy referral (MBS item 10950–10970).
- Occupational therapy: Footwear assessment, orthotics, assistive devices, and home safety modifications.
- Foot care education: Daily foot inspection, appropriate footwear, avoid walking barefoot, regular podiatry review (MBS item 10950 for diabetic foot care).
Mononeuropathies
Focal mononeuropathies are common in clinical practice and are most frequently caused by compression or entrapment at anatomical sites of vulnerability. The three most frequently encountered mononeuropathies in Australian primary care are carpal tunnel syndrome (median nerve), ulnar neuropathy at the elbow, and peroneal neuropathy at the fibular head.
Carpal Tunnel Syndrome (Median Neuropathy at the Wrist)
| Feature | Details |
|---|---|
| Epidemiology | Most common entrapment neuropathy; prevalence 3–5% of the Australian adult population. More common in women (3:1), age 40–60 years. Bilateral in up to 50%. |
| Risk factors | Repetitive wrist flexion/extension, vibration tool use, pregnancy, obesity, diabetes, hypothyroidism, rheumatoid arthritis, wrist fracture (history), haemodialysis, hereditary neuropathy with liability to pressure palsies (HNPP). |
| Symptoms | Numbness, tingling, and pain in the median nerve distribution (thumb, index, middle, and radial half of ring finger). Symptoms typically nocturnal, often waking the patient; relieved by shaking/flicking the wrist ("flick sign"). May radiate proximally to the forearm and shoulder. |
| Examination | Tinel sign (percussion over carpal tunnel), Phalen manoeuvre (forced wrist flexion for 60 seconds), thenar wasting (late finding), reduced two-point discrimination in median nerve distribution. Sensitivity of provocative tests is moderate (50–70%); confirm with NCS. |
| NCS confirmation | Prolonged distal motor latency of median nerve (>4.2 ms) and/or reduced sensory conduction velocity across the carpal tunnel compared to ulnar nerve. MBS item 11005. Severity grading guides management. |
Carpal Tunnel — Conservative Management
- Wrist splinting: Neutral-position wrist splint worn at night for ≥6 weeks. Most effective for mild-to-moderate symptoms. Available OTC (~$20–40). First-line for pregnancy-related CTS.
- Ergonomic modification: Avoid sustained wrist flexion/extension; ergonomic keyboard/mouse; work station assessment (refer to occupational therapist).
- Corticosteroid injection: Methylprednisolone 40 mg or triamcinolone 20 mg injected into the carpal tunnel (MBS item 18350). Provides short-to-medium term relief (6–12 weeks). May be repeated once. Does not alter long-term course. Useful as a bridge to surgery or diagnostic trial.
- Treat underlying causes: Thyroid function, glycaemic control, weight management, rheumatological disease management.
Carpal Tunnel — When to Refer for Surgery
- Failure of conservative management (splinting ± injection) after ≥6–8 weeks
- Severe NCS findings (absent sensory responses, prolonged motor latency >6.5 ms)
- Thenar wasting or significant motor weakness (inability to oppose thumb)
- Persistent numbness or constant symptoms (not just nocturnal)
- Patient preference for definitive treatment
Carpal tunnel release (open or endoscopic) has a success rate of >90%. Endoscopic release may allow earlier return to work. Performed by hand surgeon, orthopaedic surgeon, or plastic surgeon. MBS item 49824.
Ulnar Neuropathy at the Elbow (Cubital Tunnel Syndrome)
| Feature | Details |
|---|---|
| Epidemiology | Second most common entrapment neuropathy. More common in men. Associated with prolonged elbow flexion, resting elbow on hard surfaces, cubitus valgus (post-fracture), rheumatoid arthritis. |
| Symptoms | Tingling and numbness in the ring and little fingers (ulnar 1½ fingers), medial forearm. May experience medial elbow pain. Worsened by elbow flexion (e.g. phone use, driving). Wasting of intrinsic hand muscles (interossei, hypothenar muscles) in advanced cases — grip weakness, difficulty with fine motor tasks (e.g. opening jars). |
| Examination | Tinel sign at the cubital tunnel, Froment sign (flexion of thumb IP joint during lateral pinch — weakness of adductor pollicis), Wartenberg sign (abducted little finger — weakness of third palmar interosseous), claw hand deformity (MCP extension with IP flexion of ring and little fingers in severe cases). Test sensation over dorsal ulnar hand (dorsal cutaneous branch — spared if entrapment is at Guyon canal). |
| Diagnosis | NCS showing slowing of ulnar nerve conduction across the elbow (<50 m/s or >10 m/s drop from above to below elbow). MBS item 11005. |
Ulnar Neuropathy — Conservative Management
- Activity modification: Avoid prolonged elbow flexion (>90°), avoid leaning on elbow, avoid holding phone to ear — use speakerphone or headset. Pad elbow when resting on desks.
- Elbow splinting: Night-time elbow extension splint (maintain at 45° flexion) for 6–12 weeks. May improve mild-to-moderate symptoms.
- Physiotherapy: Nerve gliding exercises (ulnar nerve glide technique), strengthening of affected muscles, ergonomic advice.
Ulnar Neuropathy — When to Refer for Surgery
- Failure of conservative management after 3 months
- Intrinsic hand muscle wasting or weakness on examination
- Severe NCS findings (absent responses, marked slowing)
- Progressive symptoms despite activity modification
Surgical options include simple decompression, anterior transposition (submuscular or subcutaneous), or medial epicondylectomy. Anterior transposition is preferred for subluxating ulnar nerve or severe cases. MBS item 49826. Prognosis depends on severity at the time of surgery — motor recovery is less predictable if significant wasting is present.
Peroneal Neuropathy at the Fibular Head (Common Peroneal Nerve)
| Feature | Details |
|---|---|
| Epidemiology | Most common lower limb mononeuropathy. Risk factors: significant weight loss (loss of protective perineural fat), prolonged bed rest/immobilisation, leg crossing, kneeling, plaster cast application, bariatric surgery, lithotomy position during surgery. |
| Symptoms | Foot drop (difficulty dorsiflexing the foot) and ankle eversion weakness. Numbness over the dorsum of the foot and lateral leg. High-stepping gait to compensate. Patients may report tripping or scuffing the foot while walking. |
| Examination | Weakness of ankle dorsiflexion (tibialis anterior — L4/L5), great toe dorsiflexion (extensor hallucis longus), ankle eversion (peronei — L5/S1). Ankle inversion is preserved (tibial nerve — S1). Reduced sensation over the lateral leg and dorsum of the foot. Reflexes are typically preserved (ankle jerk innervated by tibial nerve). Tinel sign at the fibular head. |
| Diagnosis | NCS showing reduced amplitude or absent superficial peroneal sensory response and/or prolonged distal motor latency or reduced CMAP amplitude of the peroneal nerve. Motor conduction across the fibular head shows localised slowing. MBS item 11005. |
Peroneal Neuropathy — Conservative Management
- Address the cause: Avoid leg crossing, avoid kneeling, pad the fibular head when sitting (e.g. wheelchair users), change positions frequently.
- Ankle-foot orthosis (AFO): A lightweight AFO or foot-drop splint maintains the foot in a neutral position, improving gait and preventing falls. Prescribed by rehabilitation physician or orthotist. MBS item 10950–10970 (physiotherapy) and MBS item 19500 (orthotic prescription).
- Physiotherapy: Strengthening of dorsiflexors and evertors, gait retraining, balance exercises. Referral to physiotherapist or exercise physiologist.
- Monitoring: Most compression peroneal neuropathies recover spontaneously over 3–6 months with conservative management. Serial NCS at 3-month intervals to track recovery if no clinical improvement.
Peroneal Neuropathy — When to Refer for Surgery
- No clinical improvement after 3–4 months of conservative management
- Identifiable compressive mass (e.g. ganglion cyst, tumour) requiring excision
- Complete foot drop with absent motor responses on NCS after 3 months
- Traumatic nerve injury (laceration, fracture) — early surgical exploration
Surgical decompression of the common peroneal nerve at the fibular head may be performed by a peripheral nerve surgeon. MBS item 49824. Functional electrical stimulation (FES) devices for foot drop may be considered as an alternative to AFO in selected patients.
| Mononeuropathy | Nerve Root | Key Clinical Test | Conservative Tx Duration | Surgery Indication |
|---|---|---|---|---|
| Carpal tunnel | Median (C6–T1) | Phalen, Tinel, thenar strength | 6–8 weeks | Failure conservative Rx, motor weakness, severe NCS |
| Ulnar at elbow | Ulnar (C8–T1) | Froment, interosseous wasting | 3 months | Muscle wasting, severe NCS, progressive symptoms |
| Peroneal at fibular head | Common peroneal (L4–S1) | Foot drop, eversion weakness, Tinel at fib head | 3–4 months | No recovery at 4 months, identifiable mass, trauma |
Monitoring
Regular monitoring is essential to assess treatment efficacy, detect disease progression, manage side effects, and reduce complications such as falls and foot ulceration.
Monitoring Schedule
Complications to Monitor
- Falls: Peripheral neuropathy is an independent risk factor for falls. Use the Timed Up and Go (TUG) test or Physiological Profile Assessment (PPA). Refer to falls prevention programme if TUG >12 seconds.
- Foot ulceration: Annual monofilament testing in diabetic patients (MBS item 2401). High-risk feet: podiatry review every 3 months, appropriate footwear, daily self-inspection education.
- Charcot neuroarthropathy: Acute hot, swollen, red foot in a patient with peripheral neuropathy — consider Charcot until proven otherwise. Urgent plain X-ray and MRI. Refer to endocrinology/orthopaedics. RHDAustralia guidelines apply for management.
- Autonomic neuropathy: Orthostatic hypotension, resting tachycardia, gastroparesis, erectile dysfunction. Annual screening in diabetic patients. Assess lying and standing blood pressure at each visit.
Special Populations
Pregnancy
Paediatrics
Elderly (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Watson JC, Dyck PJB. Peripheral neuropathy: a practical approach to diagnosis and symptom management. Mayo Clin Proc. 2015;90(7):940–951. doi:10.1016/j.mayocp.2015.05.004
- 2. Callaghan BC, Price RS, Feldman EL. Diagnostic and therapeutic advances in the assessment and treatment of diabetic peripheral neuropathy. JAMA. 2015;314(10):1054–1055. doi:10.1001/jama.2015.9079
- 3. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
- 4. Pop-Busui R, Boulton AJM, Feldman EL, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136–154. doi:10.2337/dc16-2042
- 5. Australian Institute of Health and Welfare (AIHW). Diabetes: Australian Facts. Canberra: AIHW; 2023. Cat. no. CVD 83.
- 6. Joint Task Force of the EFNS and the PNS. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force. J Peripher Nerv Syst. 2021;26(3):251–263.
- 7. National Health and Medical Research Council (NHMRC). National Evidence-Based Guideline for Prevention, Identification and Management of Foot Complications in Diabetes. Melbourne: NHMRC; 2011.
- 8. Royal Australian College of General Practitioners (RACGP). Management of Type 2 Diabetes: A Handbook for General Practice. Melbourne: RACGP; 2020.
- 9. Dworkin RH, O'Connor AB, Kent J, et al. Interventional management of neuropathic pain: NeuPSIG recommendations. Pain. 2013;154(11):2249–2261. doi:10.1016/j.pain.2013.06.004
- 10. Burns J, Ouvrier R, Estilow T, et al. Validation of the Charcot–Marie–Tooth disease pediatric scale as an outcome measure of disability. Ann Neurol. 2012;71(5):642–652. doi:10.1002/ana.23572
- 11. Traub R, Xiao J, Leung E, et al. Australian burden of disease study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018. Aust N Z J Public Health. 2023;47(2):100028.
- 12. RHDAustralia (Remote Area Health Corps). Standard Treatment Manual for Primary Health Care. 6th ed. Darwin: RHDAustralia; 2022.
- 13. Padua L, Coraci D, Erra C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(12):1273–1284. doi:10.1016/S1474-4422(16)30231-9
- 14. Pharmaceutial Benefits Advisory Committee (PBAC). PBS Schedule. Canberra: Department of Health and Aged Care; 2024.