📋 Key Information Summary
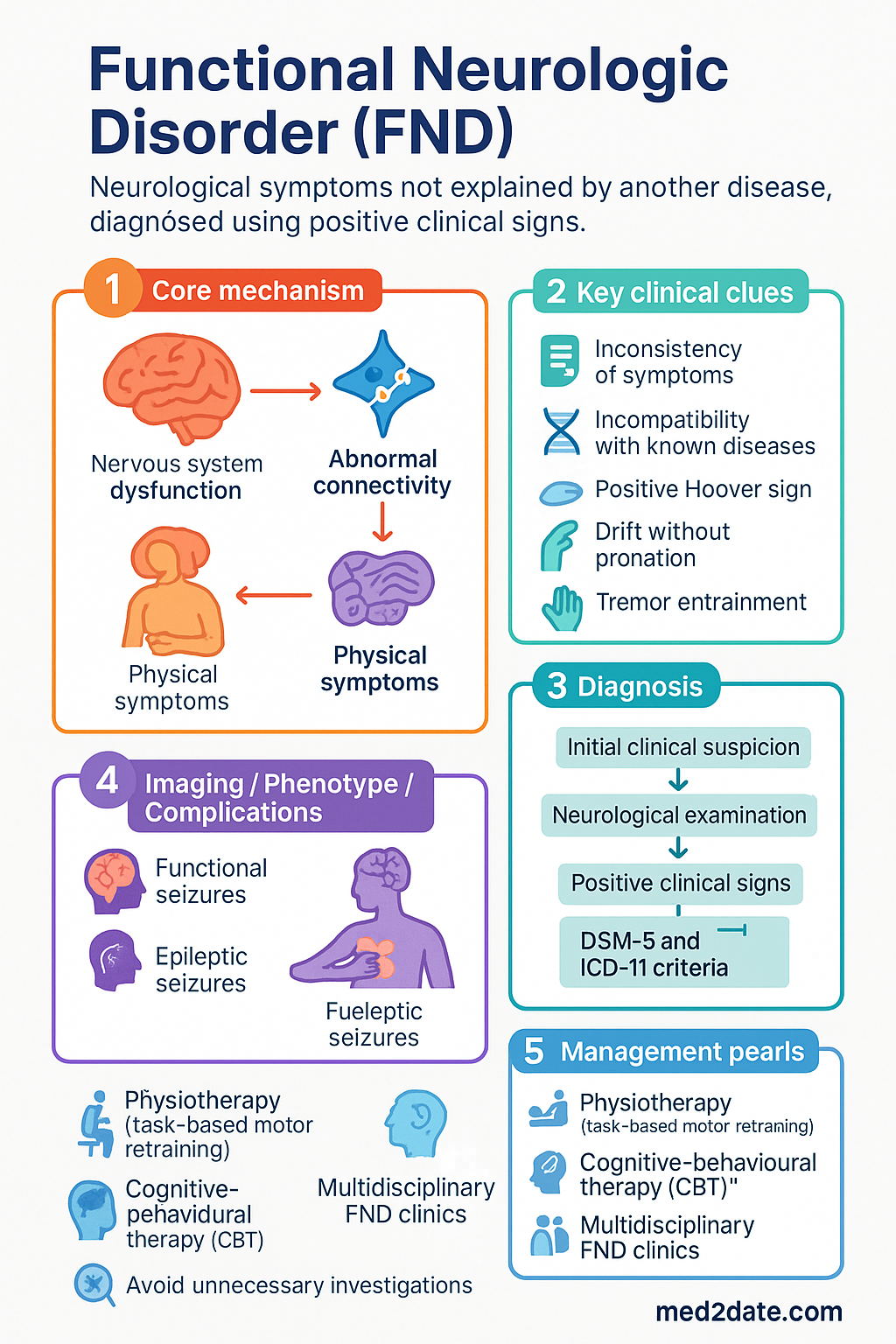
- Functional Neurologic Disorder (FND) is a genuine neurological condition characteruated by neurological symptoms not explained by another disease, diagnosed using positive clinical signs — not by exclusion alone.
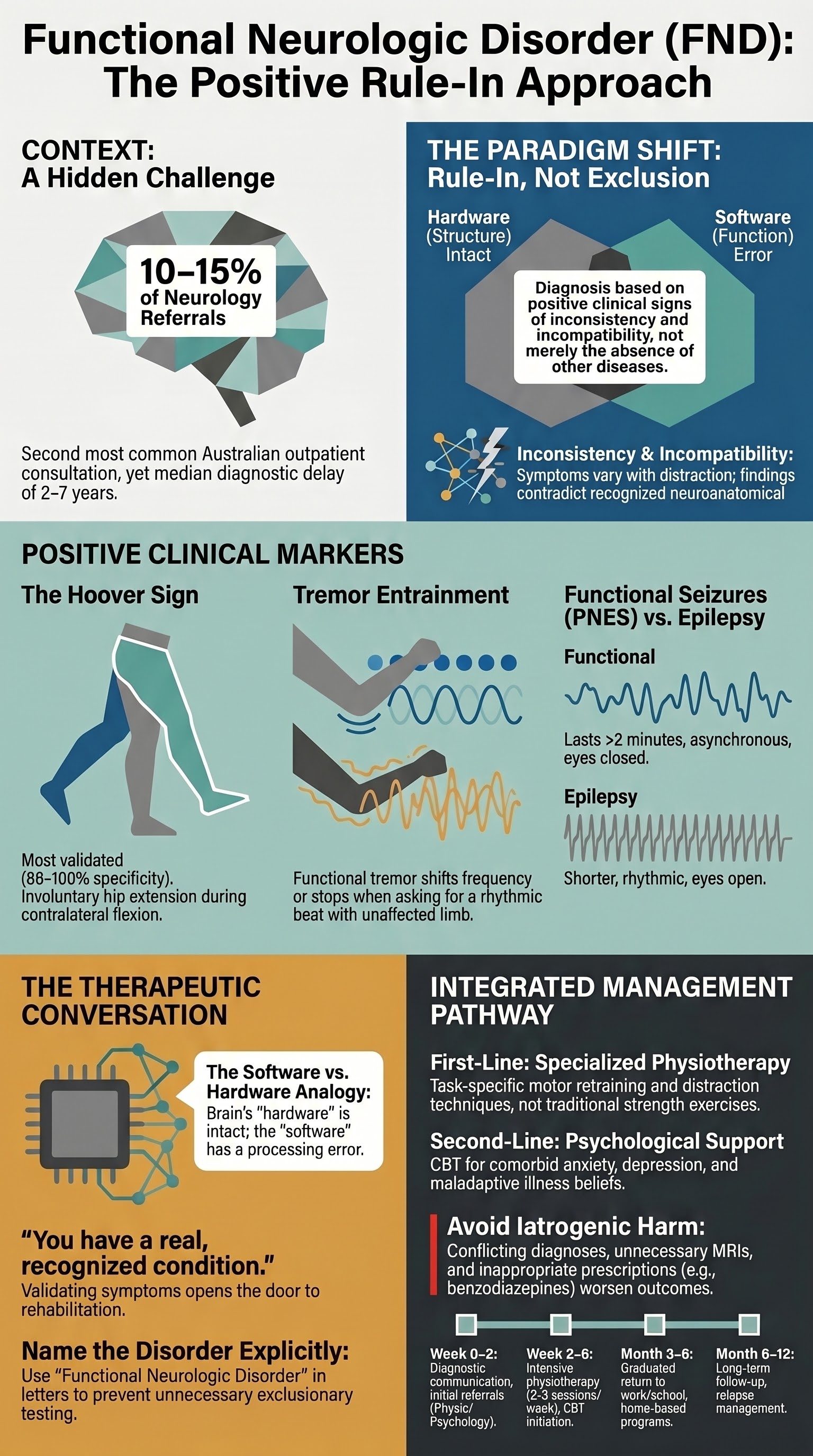
- Prevalence in Australian outpatient neurology clinics is estimated at 10–15% of referrals, making FND the second most common reason for neurological outpatient consultation after headache.
- Use the DSM-5 and ICD-11 criteria: positive signs of inconsistency (variability over time) and incompatibility with recognised neurological disease are required for diagnosis.
- The Hoover sign (involuntary hip extension during contralateral flexion against resistance) is the most widely validated positive sign for functional weakness; perform and document systematically.
- The diagnosis must be communicated as a real, diagnosable condition — never as a diagnosis of exclusion, and never framed as "all in your head" or "medically unexplained."
- Physiotherapy tailored to FND (task-based motor retraining, distraction techniques) is the first-line treatment with the strongest evidence base.
- Psychotherapy — particularly cognitive-behavioural therapy (CBT) — addresses comorbid anxiety, depression, and maladaptive illness beliefs but is not the sole treatment.
- Multidisciplinary FND clinics (available in several Australian tertiary centres) provide integrated neurological, physiotherapy, psychology, and occupational therapy input.
- Avoid iatrogenic harm: unnecessary investigations, conflicting diagnoses, dismissive language, and prolonged medical uncertainty all worsen prognosis.
- Pharmacotherapy has a limited role; treat comorbid mood disorders with SSRIs (e.g., sertraline) and manage associated pain, but no medication treats FND symptoms directly.
- Aboriginal and Torres Strait Islander Australians may experience FND in the context of intergenerational trauma and cultural distress — culturally safe engagement and local community health worker involvement are essential.
- Children and adolescents with FND require family-based approaches and school liaison; prognosis is generally better than in adults when early intervention is provided.
Introduction & Australian Epidemiology
Functional Neurologic Disorder (FND), historically termed conversion disorder or functional neurological symptom disorder, is a condition in which patients experience genuine neurological symptoms — weakness, abnormal movements, gait disturbance, sensory loss, seizure-like episodes, or cognitive difficulties — that are not fully explained by a recognised neurological or medical disease. Crucially, modern understanding frames FND as a disorder of nervous system function rather than structure, diagnosed through the presence of positive clinical signs rather than the absence of organic pathology.
The transition from a purely exclusionary diagnosis to a positive, rule-in approach represents one of the most significant conceptual shifts in neurology over the past two decades. The DSM-5 (2013) and ICD-11 (2022) both now require positive evidence of inconsistency and incompatibility for diagnosis, moving FND away from the problematic "diagnosis of exclusion" paradigm.
Australian Epidemiology
Australian data are consistent with international estimates:
- FND accounts for approximately 10–15% of new referrals to Australian outpatient neurology clinics, placing it as the second most common diagnosis after headache disorders.
- Incidence of functional seizures (psychogenic non-epileptic seizures, PNES) in Australian epilepsy monitoring units is 20–30% of patients referred for refractory "epilepsy."
- The Australian Institute of Health and Welfare (AIHW) reports significant healthcare utilisation by FND patients — multiple ED presentations, repeated investigations, and serial specialist referrals — prior to correct diagnosis, with a median diagnostic delay of 2–7 years.
- FND is more common in women (2:1 to 3:1 ratio overall), though functional motor disorder in men is increasingly recognised, particularly in older populations.
- Paediatric FND accounts for a significant proportion of referrals to Australian tertiary paediatric neurology services, with peak incidence in early adolescence (10–14 years) and a female predominance.
Recognizing FND — Positive Signs and Rule-In Approach
The diagnosis of FND rests on positive clinical signs that demonstrate inconsistency and incompatibility with recognised neurological disease. A thorough neurological examination remains the cornerstone of diagnosis — advanced imaging and neurophysiology are supportive but cannot replace clinical assessment.
DSM-5 Diagnostic Criteria (Functional Neurological Symptom Disorder)
- One or more symptoms of altered voluntary motor or sensory function.
- Clinical findings provide positive evidence of incompatibility between the symptom and recognised neurological or medical conditions.
- The symptom or deficit is not better explained by another medical or mental disorder.
- The symptom or deficit causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation.
ICD-11 Classification
In the ICD-11, FND is classified under 6B60 — Functional neurological symptom disorder, with subdivisions for presentations with weakness (6B60.0), movement disorder (6B60.1), seizure-like episodes (6B60.2), sensory disturbance (6B60.3), and mixed presentations (6B60.Y). This classification explicitly places FND within neurology, not psychiatry.
Positive Clinical Signs for Functional Weakness
| Sign | Technique | Positive Result | Evidence Level |
|---|---|---|---|
| Hoover sign | Ask the patient to flex the weak hip against resistance. Then, without telling them, test extension of the contralateral (normal) hip against resistance. | Involuntary hip extension of the weak leg is generated ("positive Hoover") — demonstrates that full voluntary power is physiologically possible. | High — sensitivity 63–100%, specificity 86–100% |
| Drift without pronation | Ask the patient to hold both arms outstretched with eyes closed for 20–30 seconds. | Functional arm drift tends to move without pronation and may show non-organic trajectory patterns (e.g., wild flapping, slow wandering). | Moderate |
| Dragging gait | Observe gait. Ask patient to walk normally, then on heels, then on toes. | A leg dragged behind like a "dead weight," often with trunk sway disproportionate to weakness. Contrasts with the circumduction pattern of a true UMN hemiparesis. | Moderate — high specificity when classical pattern present |
| Tremor entrainment | Ask the patient to perform rhythmic tapping with the unaffected limb at a specified frequency. | Functional tremor shifts to match the entrainment frequency, stops, or dramatically changes character — organic tremors do not entrain. | High — one of the most reliable signs for functional movement disorder |
| Knee-drop test | Patient supine, legs flexed at hip and knee. Ask patient to let both legs fall to one side. | The "weak" leg falls faster and with less control than the "strong" leg — this contradicts genuine pyramidal weakness where tone differences would be expected. | Moderate |
| Tubular (non-dermatomal) sensory loss | Map the boundaries of sensory loss. Test with cotton wool and pinprick across a limb circumferentially. | Sensory loss that stops sharply at a geometric boundary (e.g., the wrist all the way around the limb) rather than following dermatomal or peripheral nerve distribution. | High specificity |
Positive Signs for Functional Seizures (PNES)
| Feature | Functional Seizures (PNES) | Epileptic Seizures |
|---|---|---|
| Duration | Usually >2 minutes, often prolonged (minutes to hours) | Typically <2 minutes (tonic-clonic) |
| Eyes | Often closed during event; resistance to eye opening | Usually open during and after event |
| Movements | Asynchronous, thrashing, side-to-side head movement, pelvic thrusting, waxing/waning intensity | Rhythmic, synchronous, stereotyped |
| Postictal state | Rapid recovery, often with minimal confusion; tearfulness or distress | Prolonged confusion, Todd's paresis, drowsiness |
| EEG during event | Normal background rhythm preserved (video-EEG gold standard) | Ictal epileptiform discharges |
Inconsistency and Incompatibility — The Two Pillars
Symptoms vary in a way that organic disease does not explain — e.g., leg weakness that resolves when distracted, tremor that changes frequency between tasks, or Hoover sign positive on one day but not another.
Clinical findings do not correspond to recognised neuroanatomical or neurophysiological patterns — e.g., give-way weakness, non-dermatomal sensory loss, or seizure-like events without EEG correlate.
Investigations — When and How
FND is a clinical diagnosis. Investigations are used to exclude dangerous mimics — not to "prove" FND. The clinician must avoid the trap of endless investigation, which reinforces diagnostic uncertainty and worsens outcomes.
Communicating the Diagnosis
How the diagnosis of FND is communicated is one of the most critical steps in management. Poor communication is a major cause of treatment failure, persistent disability, and patient disengagement. Research from Australian and international centres demonstrates that the diagnostic conversation itself can be therapeutic — when done well, it shifts the patient's explanatory model and opens the door to rehabilitation.
Principles of Effective Communication
Language to Use and Language to Avoid
| ✔ Use This Language | ✘ Avoid This Language |
|---|---|
| "You have a functional neurological disorder — a real and recognised condition." | "Your tests are all normal, so there's nothing wrong." |
| "The problem is in how the brain is functioning — not in damage to the brain itself." | "It's all in your head." |
| "Your symptoms are real and can improve with targeted treatment." | "It's psychosomatic" or "You're imagining it." |
| "I found positive signs on examination that explain your symptoms." | "We couldn't find anything serious." |
| "This is common — I see this regularly in my practice." | "I've never seen anything like this before." |
| "Physiotherapy specifically designed for functional symptoms can help you regain function." | "You need to see a psychiatrist." |
Management Pathways
FND management is fundamentally multidisciplinary. There is no single "drug cure" for FND — treatment centres on targeted physiotherapy, psychological therapy for comorbidities and illness beliefs, occupational therapy, and the avoidance of iatrogenic harm. Australian tertiary FND clinics provide integrated care models, but the majority of FND management occurs in primary care and community settings.
First-Line: Physiotherapy for FND
Physiotherapy has the strongest evidence base for functional motor symptoms. It should be delivered by a physiotherapist with training or experience in FND — general neurological physiotherapy techniques (e.g., standard stroke rehabilitation exercises) are not appropriate and may worsen symptoms.
- Task-specific motor retraining: Focus on automatic and semi-automatic movements (e.g., walking while talking, reaching for objects with distraction) rather than isolated muscle strengthening.
- Distraction techniques: Encourage the patient to focus attention on a task while performing a movement — this exploits the hallmark of FND (symptoms improve when attention is diverted).
- Motor relearning hierarchy: Start with movements the patient can perform in clinic, progressively increase complexity, and transition from clinic to home and community settings.
- Avoid excessive focus on impairment: Do not repeatedly test the "weak" limb in isolation — this reinforces symptom-focused attention. Shift to functional, goal-based activities.
- Frequency: Intensive blocks of physiotherapy (2–3 sessions per week for 4–6 weeks) are more effective than sporadic sessions. Consider telehealth physiotherapy follow-up for rural and remote Australian patients.
Second-Line: Psychotherapy
Psychotherapy addresses comorbid conditions (anxiety, depression, PTSD) and maladaptive illness beliefs, but is not a substitute for physiotherapy in motor presentations. It should be framed as part of the multidisciplinary approach, not as a suggestion that the symptoms are "psychological."
Pharmacotherapy — Limited Role
No medication has been shown to treat the core symptoms of FND. Pharmacotherapy is reserved for comorbid conditions:
Multidisciplinary FND Clinics in Australia
Several Australian tertiary centres have established dedicated FND clinics providing integrated neurological, physiotherapy, psychology, and occupational therapy services:
- Neurology / Movement Disorder Clinics: Royal Melbourne Hospital, Royal Prince Alfred Hospital (Sydney), Royal Brisbane and Women's Hospital, Royal Adelaide Hospital, Alfred Hospital (Melbourne).
- Epilepsy Monitoring Units (for PNES): Comprehensive video-EEG services at most tertiary hospitals for definitive functional seizure diagnosis.
- Paediatric FND Services: The Royal Children's Hospital (Melbourne), Children's Hospital at Westmead (Sydney), Queensland Children's Hospital — these offer multidisciplinary assessment with family-centred models.
- Telehealth FND services: Increasing availability through state-funded neurology telehealth networks, particularly important for patients in regional and remote Australia.
Avoiding Iatrogenic Harm
- Conflicting diagnoses: One clinician says "it's functional," another says "it might be MS." Inconsistent messaging from the medical team undermines the diagnosis and delays recovery.
- Unnecessary investigations: Repeated MRIs, lumbar punctures, and EMGs in the absence of new clinical findings reinforce the patient's belief that something serious has been missed.
- Inappropriate prescriptions: Continuing antiepileptics after a confirmed diagnosis of PNES; prescribing opioids for functional pain; escalating benzodiazepines for functional seizures.
- Dismissive communication: Telling patients "there's nothing wrong" or "it's stress" without providing a positive diagnosis framework.
- Prolonged diagnostic uncertainty: Refusing to name the diagnosis because the clinician is uncomfortable with FND. A named, explained diagnosis — even if it requires a difficult conversation — is always better than indefinite uncertainty.
Monitoring and Follow-Up
Special Populations
Paediatrics
Pregnancy
Elderly
Renal Impairment
Hepatic Impairment
Immunocompromised
📚 References
- 1. Espay AJ, Aybek S, Carson A, et al. Current concepts in diagnosis and treatment of functional neurological disorders. JAMA Neurol. 2018;75(9):1132–1141.
- 2. Stone J, Carson A, Duncan R, et al. Symptoms 'unexplained by organic disease' in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain. 2009;132(10):2878–2888.
- 3. Carson A, Stone J, Hibberd C, et al. Disability, distress, and unemployment in neurology outpatients with symptoms 'unexplained by organic disease.' J Neurol Neurosurg Psychiatry. 2011;82(7):810–813.
- 4. Goldstein LH, Robinson EJ, Mellers JDC, et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial. Lancet Psychiatry. 2020;7(6):491–505.
- 5. Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: a systematic review. J Psychosom Res. 2015;79(6):555–563.
- 6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: APA; 2013.
- 7. World Health Organization. International Classification of Diseases 11th Revision (ICD-11). Geneva: WHO; 2022.
- 8. Stone J, Carson A, Hallett M. Explanation as treatment for functional neurological disorders. Handb Clin Neurol. 2016;139:543–553.
- 9. Edwards MJ, Adams RA, Brown H, Pareés I, Friston KJ. A Bayesian account of "hysteria." Brain. 2012;135(11):3495–3512.
- 10. Ludwig L, Pasman JA, Nicholson T, et al. Stressful life events and maltreatment in conversion (functional neurological) disorder: systematic review and meta-analysis of case-control studies. Lancet Psychiatry. 2018;5(4):307–320.
- 11. Australian Institute of Health and Welfare. Burden of Disease in Aboriginal and Torres Strait Islander Australians. AIHW; 2022.
- 12. Kyle C, Sheldrick R, Aybek S, et al. How can we explain functional neurological disorder? The role of causal beliefs in symptom perception and treatment-seeking. J Psychosom Res. 2023;171:111382.
- 13. Nicholson TR, Stone J, Kanaan RA. Conversion disorder: a problematic diagnosis. J Neurol Neurosurg Psychiatry. 2011;82(11):1267–1273.
- 14. LaFrance WC Jr, Baker GA, Duncan R, Goldstein LH, Reuber M. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach. Epilepsia. 2013;54(11):2005–2018.