📋 Key Information Summary
- Concussion is a clinical syndrome of transient neurological dysfunction caused by biomechanical forces, with normal structural neuroimaging (CT/MRI).
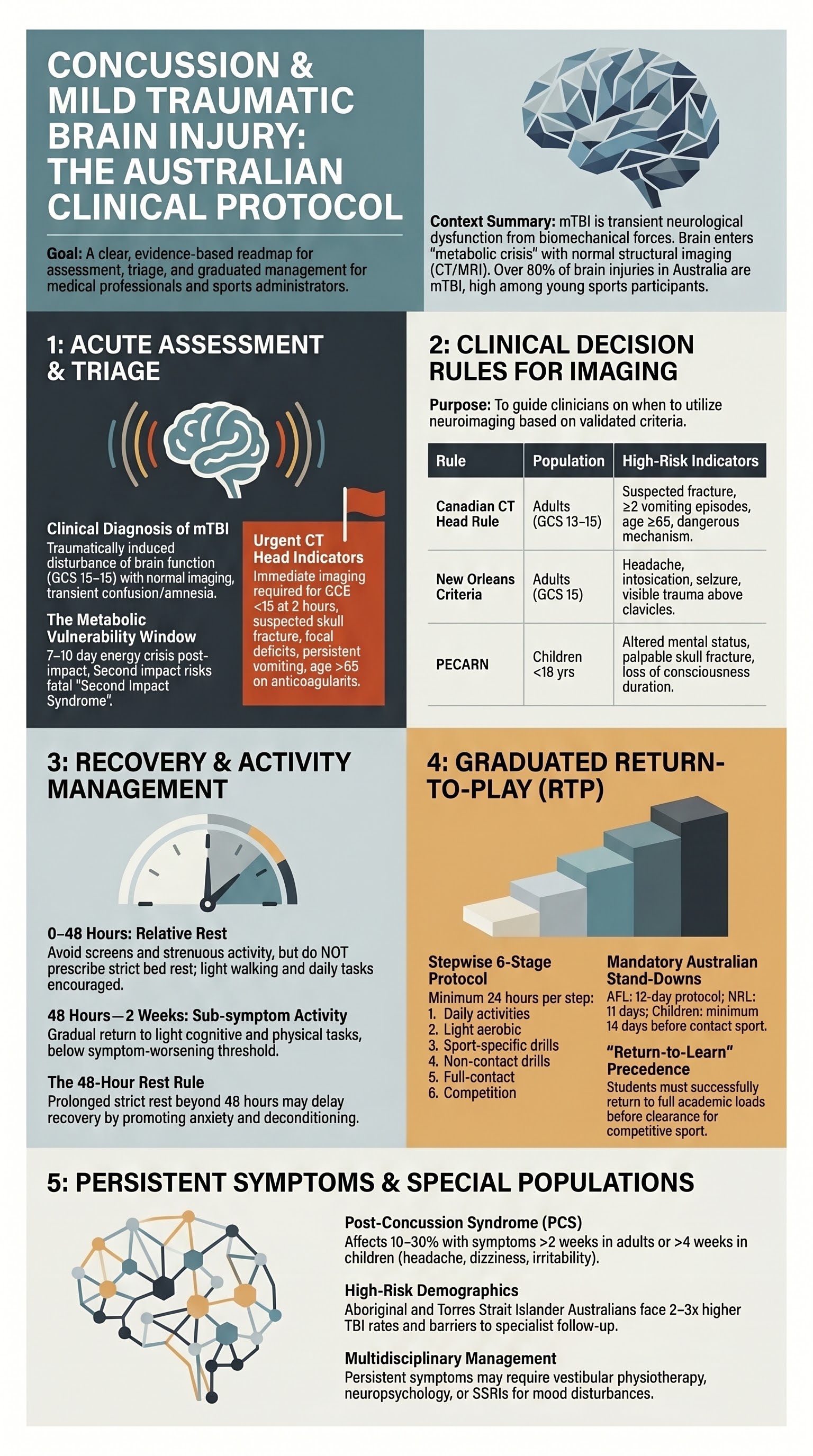
- Mild TBI accounts for >80% of traumatic brain injury presentations in Australian emergency departments, with sport-related concussion a major contributor in children and young adults.
- Red flags for urgent CT head include: GCS <15 at 2 hours post-injury, suspected skull fracture, focal neurological deficits, persistent vomiting, coagulopathy, and age >65 years on anticoagulants.
- Use the Canadian CT Head Rule or New Orleans Criteria to guide imaging decisions in adults presenting within 24 hours of injury with GCS 13–15.
- Cognitive and physical rest for 24–48 hours is recommended after concussion; prolonged strict rest beyond 48 hours is NOT advised and may delay recovery.
- Graduated return-to-play (RTP) and return-to-learn (RTL) protocols require stepwise progression, with each step taking a minimum of 24 hours, and the athlete/student must be symptom-free before advancing.
- Post-concussion syndrome (symptoms lasting >2–4 weeks) affects 10–30% of patients; common symptoms include headache, dizziness, cognitive difficulties, irritability, and sleep disturbance.
- Multidisciplinary management of persistent symptoms includes physiotherapy (vestibular/oculomotor rehabilitation), neuropsychology, and graduated aerobic exercise therapy.
- Children and adolescents have longer recovery times (typically 2–4 weeks) and should follow the 2023 Amsterdam EHR+ consensus paediatric RTP guidelines.
- Patients on anticoagulants or antiplatelets with head injury require a lower threshold for CT and extended observation, even with minor mechanism of injury.
- Aboriginal and Torres Strait Islander Australians face higher rates of TBI from assault and road trauma, compounded by barriers to specialist follow-up in remote communities.
- Any patient with suspected concussion should NOT return to contact sport on the same day; mandatory stand-down periods apply under Australian sporting codes (e.g., AFL 12-day protocol).
Introduction & Australian Epidemiology
Concussion, often termed mild traumatic brain injury (mTBI), is defined as a traumatically induced transient disturbance of brain function involving biomechanical forces that results in rapid onset of short-lived neurological impairment. Structural neuroimaging (CT, MRI) is characteristically normal. The diagnosis remains fundamentally clinical, relying on symptom assessment, cognitive testing, and neurological examination.
In Australia, TBI accounts for approximately 150,000 emergency department presentations annually, with mild TBI (GCS 13–15) comprising over 80% of cases. The Australian Institute of Health and Welfare (AIHW) reports that falls, transport accidents, and assaults are the leading causes, with sport-related concussion an increasingly recognised public health issue. Children aged 5–14 years and young adults aged 15–24 years carry the highest incidence of concussion.
The economic burden is significant: direct healthcare costs for TBI in Australia exceed $8.6 billion per annum (AIHW, 2023). Indigenous Australians experience TBI at rates 2–3 times higher than the non-Indigenous population, driven by higher rates of interpersonal assault and road trauma in regional and remote areas.
This guideline addresses the acute assessment, imaging decisions, post-concussion symptom management, and return-to-activity protocols for adults and children with concussion and mTBI in the Australian clinical context.

Pathophysiology
Concussion involves a complex cascade of neurometabolic events following biomechanical force to the brain. The key pathophysiological processes include:
- Primary injury: Rotational and acceleration–deceleration forces cause diffuse neuronal depolarisation and axonal strain, particularly affecting the corpus callosum and brainstem.
- Metabolic crisis: An indiscriminate release of potassium (K⁺) and glutamate triggers an energy-intensive ionic pump restoration process, increasing glucose demand while cerebral blood flow is transiently reduced.
- Mitochondrial dysfunction: Impaired oxidative phosphorylation creates a transient "energy crisis" lasting days to weeks.
- Neuroinflammation: Microglial activation and cytokine release may perpetuate symptoms in a subset of patients, contributing to post-concussion syndrome.
- Vulnerability window: The brain is metabolically vulnerable to repeat injury for 7–10 days; a second impact during this period risks severe cerebral oedema and death ("second impact syndrome").
Clinical Presentation & Diagnostic Criteria
Diagnostic Criteria (CDC/WHO Definition)
Concussion is diagnosed when ALL of the following are met:
- Mechanism: an injury biomechanical force (blow to the head, face, neck, or elsewhere with impulsive force transmitted to the head).
- Acute clinical signs: one or more of the following — confusion/disorientation, loss of consciousness (LOC) lasting ≤30 minutes, post-traumatic amnesia (PTA) lasting ≤24 hours, or other transient neurological abnormality.
- GCS 13–15 at presentation (GCS 13–14 may represent mild TBI with intracranial pathology and requires closer monitoring).
- Normal structural neuroimaging (when performed).
Common Presenting Symptoms
| Domain | Symptoms |
|---|---|
| Somatic | Headache, nausea/vomiting, dizziness, visual disturbance, photosensitivity, phonosensitivity |
| Cognitive | "Fogginess," difficulty concentrating, feeling slowed down, memory impairment, word-finding difficulty |
| Emotional | Irritability, sadness, anxiety, emotional lability |
| Sleep | Drowsiness, difficulty initiating sleep, sleeping more or less than usual |
| Vestibular/ocular | Balance impairment, saccadic dysfunction, convergence insufficiency |
Standardised Assessment Tools
- Sport Concussion Assessment Tool 6 (SCAT6): The gold-standard sideline and clinical assessment tool for patients aged 13 years and older. Includes symptom evaluation, cognitive screening (orientation, immediate memory, concentration), neurological screen, and delayed recall.
- Child SCAT6: Modified for children aged 5–12 years with age-appropriate cognitive tasks and parent symptom reporting.
- Glasgow Coma Scale (GCS): Used in emergency triage; GCS 13–15 is classified as mild TBI.
- Standardised Assessment of Concussion (SAC): Brief cognitive screen suitable for sideline use.
Initial Assessment — Red Flags, Rest, and Return-to-Activity Guidance
Red Flags Requiring Urgent Imaging and Neurosurgical Referral
- GCS <15 at 2 hours post-injury
- Suspected open or depressed skull fracture
- Signs of basal skull fracture (CSF otorrhoea/rhinorrhoea, Battle sign, raccoon eyes)
- Focal neurological deficit (asymmetry, new weakness, dysphasia)
- Post-traumatic seizure
- More than one episode of vomiting since injury
- Anticoagulant or antiplatelet use (warfarin, DOACs, clopidogrel, aspirin)
- Age ≥65 years with any loss of consciousness or amnesia
- Dangerous mechanism: pedestrian vs. motor vehicle, ejected from vehicle, fall >1 metre or >5 stairs
- Amnesia before impact (retrograde amnesia >30 minutes)
CT Head Decision Rules
| Rule | Population | Key Criteria | Sensitivity for Neurosurgical Lesion |
|---|---|---|---|
| Canadian CT Head Rule | Adults, GCS 13–15, within 24 hrs | GCS <15 at 2 hrs, suspected skull fracture, ≥2 vomiting episodes, age ≥65, dangerous mechanism, amnesia >30 min | ~100% |
| New Orleans Criteria | Adults, GCS 15, within 24 hrs | Headache, vomiting, age >60, drug/alcohol intoxication, seizure, traumatic amnesia, visible trauma above clavicles | ~99% |
| PECARN (Paediatric) | Children <18 years | Stratified by age (<2 and ≥2); includes GCS, altered mental status, loss of consciousness, skull fracture signs, vomiting, headache severity, mechanism | ~97–99% |
Cognitive and Physical Rest Recommendations
Return-to-Play (RTP) Protocol — Graduated 6-Step
Based on the Consensus Statement on Concussion in Sport (Berlin 2016 / Amsterdam 2023) and adopted by the AFL, NRL, Rugby Australia, and Football Australia. Each step requires a minimum of 24 hours. If symptoms recur, return to the previous step.
| Step | Activity | Objective |
|---|---|---|
| Step 1 | Symptom-limited daily activities | Gradual return to routine activities (school, work) with accommodations |
| Step 2 | Light aerobic exercise (walking, stationary cycling) | Increase heart rate; no resistance training or sport-specific activity |
| Step 3 | Sport-specific exercise (running drills) | Add movement; no head-impact activities |
| Step 4 | Non-contact training drills | Increase complexity, coordination, and cognitive load |
| Step 5 | Full-contact practice (after medical clearance) | Restore confidence and assess functional tolerance |
| Step 6 | Return to competition | Full participation with no restrictions |
Return-to-Learn (RTL) / Return-to-Work Protocol
Cognitive demands are often more provocative of symptoms than physical activity, particularly in students. A graduated return should include:
- Stage 1 (Days 1–3): No formal academic work; brief, voluntary cognitive tasks at home (conversation, listening to music). Limit screen time to tolerance.
- Stage 2: Light school attendance (partial days) with accommodations: extra time, reduced workload, no exams, preferential seating away from noise/light.
- Stage 3: Near-full attendance; phased introduction of exams and assessments with extensions.
- Stage 4: Full academic schedule without accommodations.
- Workplace return follows similar principles: reduced hours, decreased screen time, phased increase in duties, occupational health and safety assessment.
Post-Concussion Symptoms — Assessment and Management
Post-Concussion Syndrome Definition
Post-concussion syndrome (PCS) is defined as the persistence of concussion-related symptoms beyond the expected recovery window — generally >2 weeks in adults and >4 weeks in children/adolescents. Prevalence varies from 10–30% depending on definition, patient demographics, and injury characteristics.
Common Post-Concussion Symptoms and Management
Headache
Headache is the most common persistent symptom (up to 90%). Types include tension-type, migraine-like, cervicogenic, and medication-overhead headache.
- Acute analgesia: Paracetamol (Panadol®) 1 g PO QID PRN (max 4 g/day). Avoid routine use of NSAIDs in the first 48 hours due to bleeding risk, though short-term use may follow if CT is clear and no coagulopathy.
- Migraine-like headaches: Consider amitriptyline 10–25 mg PO nocte, titrate to 50–75 mg. PBS: Authority Required for neuropathic pain. Nerve blocks (greater occipital nerve) by specialist if refractory.
- Cervicogenic headache: Physiotherapy with cervical spine assessment, manual therapy, and postural correction.
- Avoid: Triptans and opioids acutely; regular use of simple analgesia >15 days/month (medication-overuse headache risk).
Mood Changes — Anxiety, Depression, Irritability
Emotional dysregulation is reported in 30–50% of patients with persistent symptoms and is often multifactorial (neurobiological, psychosocial, pain-related).
- Reassurance and psychoeducation: validate the patient's experience; explain that mood symptoms are a recognised part of the concussion recovery trajectory.
- Psychological support: cognitive behavioural therapy (CBT) is first-line for anxiety and depression post-concussion. Referral to a clinical psychologist experienced in brain injury is recommended.
- Pharmacotherapy if symptoms are moderate–severe or persistent beyond 4 weeks:
- Depression: Sertraline 50 mg PO mane, titrate to 100–200 mg. PBS: General Benefit.
- Anxiety: SSRIs (sertraline or escitalopram) preferred. Avoid benzodiazepines — risk of cognitive impairment, dependence, and impaired neurorecovery.
- Irritability/agitation: Low-dose amitriptyline or SSRIs; specialist referral if behavioural disturbance.
Sleep Disturbance
Sleep-wake disruption affects 30–70% of concussion patients. Both insomnia and hypersomnia may occur.
- Sleep hygiene education: consistent wake time, limit caffeine after midday, screen-free period 1 hour before bed, dim lighting in the evening.
- Pharmacological options (if persistent beyond 2–4 weeks):
- Melatonin (Circadin®) 2 mg PO modified-release 1–2 hours before bedtime. PBS: Authority Required (≥55 years); otherwise private prescription.
- Amitriptyline 10–25 mg PO nocte (dual benefit for headache and sleep).
- Mirtazapine 15 mg PO nocte if concurrent depression with insomnia.
- Avoid: Zolpidem, zopiclone (cognitive side effects, falls risk), antihistamines (diphenhydramine — confusion in elderly).
- Refer to sleep medicine specialist if suspected obstructive sleep apnoea (common in post-TBI) or persistent circadian rhythm disruption.
Dizziness and Vestibular Symptoms
Cognitive Difficulties
- Formal neuropsychological assessment if cognitive complaints persist beyond 4–6 weeks, with objective baseline data available where possible.
- Graduated aerobic exercise therapy has the strongest evidence base for improving cognitive symptoms (Leddy et al., 2018).
- Occupational therapy for functional cognitive strategies: memory aids, task management, energy conservation.
- Avoid: Routine use of stimulant medications (methylphenidate) for cognitive symptoms unless prescribed by a specialist with TBI experience.
Multidisciplinary Referral Pathway
| Specialist | Indication |
|---|---|
| Sports/Exercise Physician | Complex concussion, RTP decision-making, recurrent concussion |
| Neurologist | Persistent headache syndromes, seizure, diagnostic uncertainty |
| Neuropsychologist | Objective cognitive assessment, medicolegal, return-to-work planning |
| Vestibular Physiotherapist | Persistent dizziness, BPPV, balance impairment |
| Psychiatrist / Clinical Psychologist | Severe mood disturbance, pre-existing psychiatric comorbidity, suicidal ideation |
| Ophthalmologist / Neuro-ophthalmologist | Persistent visual symptoms, convergence insufficiency, suspected structural pathology |
| Neurosurgeon | Intracranial haemorrhage, depressed skull fracture, neurological deterioration |
Investigations
Most concussion/mTBI investigations are aimed at excluding intracranial pathology rather than confirming concussion. Routine blood work is not required in isolated concussion with normal neurological examination.
Risk Stratification
Prognostic Factors for Delayed Recovery
| Factor | Impact on Recovery |
|---|---|
| Prior concussion history (≥2) | Increased risk of prolonged symptoms and cumulative neurological effects |
| Pre-existing migraine | More severe headaches, longer duration |
| Mental health conditions (anxiety, depression, PTSD) | Worse outcomes; bidirectional relationship with post-concussion mood symptoms |
| Age >55 years | Slower neurorecovery; higher risk of subdural haematoma |
| Female sex | Longer symptom duration in sport-related concussion (multifactorial) |
| Learning disability / ADHD | May require more academic accommodations; baseline comparison essential |
| High initial symptom burden (PCSS >30) | Strongest predictor of prolonged recovery |
Pharmacotherapy — Symptom Management
Pharmacotherapy plays a supportive role in managing post-concussion symptoms. There is no medication proven to accelerate neurorecovery. Treatment is symptom-targeted.
Monitoring
Acute Monitoring (First 24–48 Hours)
- Patients discharged from ED with head injury advice sheet: monitor for worsening headache, repeated vomiting, confusion, drowsiness, seizure, unequal pupils, or limb weakness. Return to ED if any develop.
- For patients on anticoagulants/antiplatelets: minimum 4-hour ED observation with repeat GCS and neurological assessment before discharge.
- Sleep: patients may sleep normally. No need for hourly waking unless specifically directed by the treating clinician for high-risk features not meeting CT criteria.
Subacute Monitoring (1–4 Weeks)
- GP review at 1–2 weeks post-injury: symptom assessment, review of RTP/RTL progress, reassurance, and identification of red flags for referral.
- Validated symptom scales at each visit: Post-Concussion Symptom Scale (PCSS) or SCAT6 symptom checklist. Track trajectory — symptoms should be improving.
- Mood screening: PHQ-9 and GAD-7 at 2-week follow-up.
Ongoing Monitoring (>4 Weeks)
- If symptoms persist beyond 4 weeks (adults) or 6 weeks (children): refer to concussion specialist for multidisciplinary assessment.
- Formal neuropsychological testing if cognitive complaints remain.
- Repeat neuroimaging (MRI brain) if new or progressive neurological symptoms, or diagnostic uncertainty.
- For athletes: serial SCAT assessments and gradual RTP monitoring by sports medicine physician.
- Long-term follow-up: patients with multiple concussions require neurological surveillance, discussion of career modification, and assessment for cumulative cognitive effects.
Special Populations
Paediatric
Elderly (≥65 Years)
Renal Impairment
Hepatic Impairment
Immunocompromised
Pregnancy
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience traumatic brain injury at 2–3 times the rate of the non-Indigenous population. Assault-related TBI, road trauma, and falls are disproportionately represented. The burden is compounded by delayed presentation, limited access to specialist and allied health services in regional and remote communities, and higher rates of pre-existing comorbidities (e.g., cardiovascular disease, renal disease, substance use disorders) that complicate recovery.
📚 References
- 1. Patricios JS, Schneider KJ, Dvorak J, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport — Amsterdam, October 2022. Br J Sports Med. 2023;57(11):695–711.
- 2. McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport — the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838–847.
- 3. Steyerberg EW, Wiegers E, Sewalt C, et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019;18(10):923–934.
- 4. Australian Institute of Health and Welfare (AIHW). Hospitalised injury in Aboriginal and Torres Strait Islander people 2017–18. Injury research and statistics series no. 132. Cat. no. INJCAT 215. Canberra: AIHW; 2022.
- 5. Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357(9266):1391–1396.
- 6. Haydel MJ, Preston CA, Mills TJ, et al. Indications for computed tomography in patients with minor head injury. N Engl J Med. 2000;343(2):100–105.
- 7. Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160–1170.
- 8. Leddy JJ, Haider MN, Ellis MJ, Willer BS. Exercise is medicine for concussion. Curr Sports Med Rep. 2018;17(8):262–270.
- 9. Schneider KJ, Leddy JJ, Guskiewicz KM, et al. Rest and treatment/rehabilitation following sport-related concussion: a systematic review. Br J Sports Med. 2017;51(12):930–934.
- 10. Lovell MR, Collins MW. Neuropsychological assessment of the college football player. J Head Trauma Rehabil. 1998;13(2):9–26.
- 11. Sport Concussion Assessment Tool 6 (SCAT6). Br J Sports Med. 2023;57(11):722–731.
- 12. Australian Concussion Guidelines for Youth and Community Sport. Australian Government — Department of Health and Aged Care. Canberra; 2024.
- 13. Royal Australian College of General Practitioners (RACGP). Management of mild traumatic brain injury in general practice. East Melbourne: RACGP; 2023.
- 14. Jadavji T, Bhatt S, Engel A, et al. Paediatric mild traumatic brain injury: management and outcome. J Paediatr Child Health. 2022;58(9):1515–1520.
- 15. Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014–1025.