📋 Key Information Summary
- A first unprovoked seizure requires urgent EEG (ideally within 24–48 hours), MRI brain, basic metabolic panel, and assessment of provoking factors (sleep deprivation, alcohol, infection, metabolic derangement).
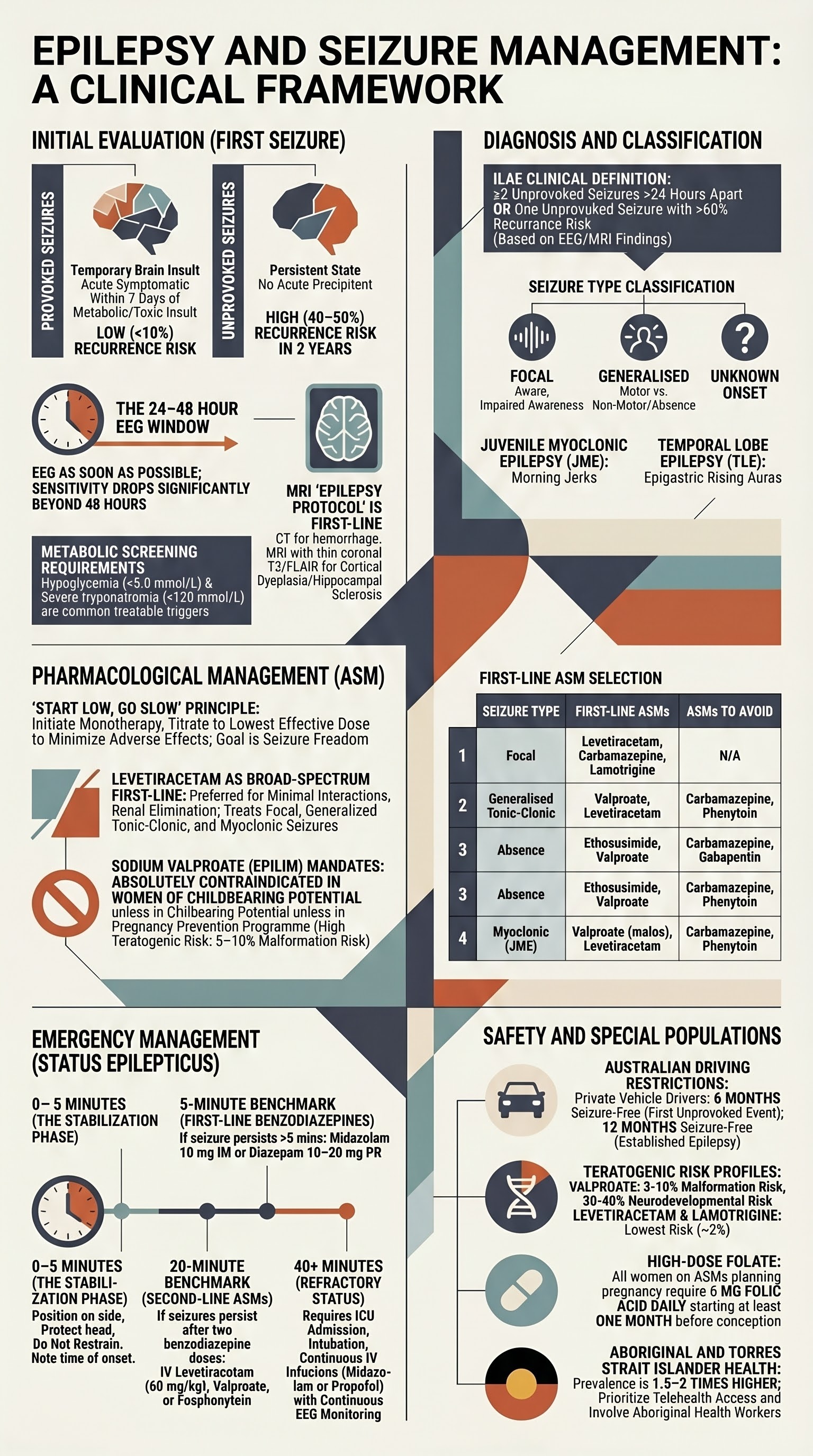
- Epilepsy is diagnosed after ≥2 unprovoked seizures >24 hours apart, or one unprovoked seizure with a high recurrence risk (>60% on EEG with epileptiform discharges).
- Seizure classification follows the ILAE 2017 framework: focal (aware/impaired awareness, motor/non-motor), generalised (tonic-clonic, absence, myoclonic, atonic), and unknown onset.
- Driving restrictions in Australia after a first unprovoked seizure: minimum 6 months seizure-free for private vehicle (varies by state/territory); 12 months for commercial licences per Austroads Assessing Fitness to Drive.
- Antiseizure medication (ASM) should be initiated after a diagnosis of epilepsy, not routinely after a single unprovoked seizure unless EEG or MRI shows high-risk features.
- First-line ASMs by seizure type: focal — levetiracetam (Keppra®), carbamazepine (Tegretol®), lamotrigine (Lamictal®); generalised tonic-clonic — valproate or levetiracetam; absence — ethosuximide or valproate; myoclonic — levetiracetam or valproate.
- Levetiracetam is the most commonly used first-line ASM in Australia due to broad efficacy, minimal drug interactions, and renal (not hepatic) elimination.
- Sodium valproate (Epilim®) is absolutely contraindicated in women of childbearing potential unless enrolled in the Pregnancy Prevention Programme (TGA mandatory) due to high teratogenic risk (neural tube defects, neurodevelopmental effects).
- Status epilepticus (≥5 minutes of continuous seizure or ≥2 discrete seizures without recovery) requires immediate benzodiazepines (midazolam IM pre-hospital; IV diazepam or lorazepam in ED), followed by IV levetiracetam, valproate, or phenytoin if seizures persist beyond 20 minutes.
- All women with epilepsy planning pregnancy should receive high-dose folate (5 mg daily) at least 1 month before conception, and ASM doses may need adjustment due to altered pharmacokinetics in pregnancy.
- Aboriginal and Torres Strait Islander Australians have higher rates of epilepsy and status epilepticus, with barriers including remote access to neurology, delayed EEG availability, and cultural factors affecting medication adherence.
- Referral to a neurologist or epilepsy specialist is recommended for all new diagnoses, refractory epilepsy (failure of 2 appropriate ASMs), suspected genetic or structural epilepsy syndromes, and women of childbearing age.
First Seizure Evaluation
A first seizure presentation is a common reason for emergency department attendance and general practice referral in Australia. The key clinical objectives are to confirm the event was a seizure (versus syncope, psychogenic non-epileptic seizures, or other paroxysmal events), identify provoking factors, assess recurrence risk, and determine whether investigation and treatment thresholds have been met.
Provoked vs Unprovoked Seizures
A provoked (acute symptomatic) seizure occurs in close temporal relationship to an acute systemic, metabolic, or toxic insult, or in the context of an acute brain insult (e.g., stroke, traumatic brain injury, CNS infection). Provoked seizures have a low recurrence risk once the provoking factor is resolved and do not, by themselves, constitute epilepsy.
An unprovoked seizure has no identifiable acute precipitant. Unprovoked seizures carry a recurrence risk of approximately 40–50% within 2 years, increasing to >60% if epileptiform discharges are present on EEG.
| Feature | Provoked (Acute Symptomatic) | Unprovoked |
|---|---|---|
| Timing | Within 7 days of acute insult | No identifiable acute precipitant |
| Common causes | Hypoglycaemia, hyponatraemia, hypocalcaemia, alcohol withdrawal, drug intoxication/withdrawal, CNS infection, acute stroke, traumatic brain injury, eclampsia | Structural lesion (tumour, cortical dysplasia), genetic predisposition, cryptogenic |
| Recurrence risk | Low (<10%) if cause fully corrected | 40–50% within 2 years |
| ASM indication | Treat the underlying cause; ASMs rarely needed long-term | Consider ASM if high recurrence risk or after second unprovoked seizure |
| Driving restriction | Generally 4 weeks if isolated, fully corrected cause | Minimum 6 months seizure-free (private vehicle) |
Metabolic Causes to Exclude
All patients presenting with a first seizure require a basic metabolic screen. Seizures secondary to metabolic derangement are provoked and generally do not require long-term ASM therapy.
EEG Timing
An EEG should be performed as soon as possible after a first unprovoked seizure, ideally within 24–48 hours. Early EEG has higher sensitivity for detecting epileptiform abnormalities (sensitivity increases from ~30% on routine EEG to ~50–70% if performed within 24 hours). In Australia, EEG is accessible in major hospitals; however, outpatient EEG may have wait times of 2–6 weeks in regional areas.
- Routine EEG (MBS Item 11005): 20–30 minute recording; available at most metropolitan hospitals. Can be performed as an inpatient or outpatient.
- Sleep-deprived EEG: Improves yield if routine EEG is normal; patient sleeps only 3–4 hours the night before.
- Prolonged/ambulatory EEG: Consider if clinical suspicion remains high with normal routine EEG.
- Presence of epileptiform discharges on EEG increases 2-year recurrence risk to >60%, supporting early ASM initiation discussion.
Neuroimaging
MRI brain with epilepsy protocol is the recommended first-line neuroimaging for all patients with a first unprovoked seizure, except in clearly provoked seizures where the cause is identified and fully corrected. CT head has a role in the acute setting to exclude haemorrhage, space-occupying lesion, or hydrocephalus but has poor sensitivity for cortical dysplasia, hippocampal sclerosis, and low-grade gliomas.
- CT head (non-contrast) — MBS Item 56001: Perform acutely in ED if focal neurological signs, persistent altered consciousness, anticoagulation, or suspected structural lesion. Available 24/7 at most Australian hospitals.
- MRI brain (epilepsy protocol) — MBS Item 63060/63063: Includes thin coronal T2/FLAIR sequences through the temporal lobes and hippocampi. Requires neurology or neurosurgery referral. Wait times in regional Australia may be 4–8 weeks; urgent inpatient MRI if suspected structural cause.
- In children, MRI under general anaesthesia may be required; this is available at paediatric tertiary centres.
Driving Restrictions
Australian driving restrictions are governed by Austroads Assessing Fitness to Drive (2022 update):
| Scenario | Private Vehicle (Car) | Commercial Licence (Heavy Vehicle, Bus, Taxi) |
|---|---|---|
| Single provoked seizure (fully resolved cause) | Minimum 4 weeks seizure-free | Minimum 6 months seizure-free |
| Single unprovoked seizure | Minimum 6 months seizure-free | Minimum 12 months seizure-free (consider specialist review) |
| Established epilepsy (≥2 unprovoked seizures) | Minimum 12 months seizure-free (or seizure-free with appropriate ASMs) | Generally disqualifying; individual assessment by treating neurologist and licensing authority |
| Seizures only in sleep | 3 years of exclusively nocturnal seizures with no daytime seizures | Generally disqualifying |
State-specific legislation varies. For example, in Victoria, mandatory reporting is required under the Road Safety Act 1986, while in NSW it is governed by the Road Transport Act 2013. GPs should document the driving discussion, provide written patient advice, and notify the licensing authority in writing.
Step-by-Step Approach to First Seizure
Diagnosis of Epilepsy
Epilepsy is a clinical diagnosis based on the ILAE 2014 operational definition: ≥2 unprovoked seizures occurring >24 hours apart, or one unprovoked seizure with a probability of recurrence ≥60% (e.g., epileptiform EEG abnormalities, structural brain lesion on MRI), or diagnosis of an epilepsy syndrome.
ILAE 2017 Seizure Classification
The ILAE 2017 classification replaces the older terms "partial" and "grand mal/petit mal." Seizure type is classified by onset (focal, generalised, unknown) and then by awareness, motor/non-motor features, and evolution.
| Seizure Type | Subtypes | Key Clinical Features | EEG Pattern |
|---|---|---|---|
| Focal aware | Motor (clonic, tonic, automatisms); Non-motor (autonomic, emotional, sensory, cognitive) | Aura only; consciousness preserved; may be mistaken for anxiety, migraines, or TIAs | Focal epileptiform discharges, lateralised rhythmic activity |
| Focal impaired awareness | Motor or non-motor onset; often evolves to bilateral tonic-clonic | Staring, unresponsiveness, automatisms (lip smacking, hand fumbling), post-ictal confusion | Temporal or frontal sharp waves; may show ictal pattern from one hemisphere |
| Generalised motor | Tonic-clonic, tonic, clonic, myoclonic, atonic | Bilateral symmetric involvement from onset; tonic-clonic = most common and dramatic; cyanosis, tongue biting, incontinence, post-ictal drowsiness | Generalised spike-and-wave (3 Hz for absence), polyspike-and-wave (myoclonic), diffuse attenuation (tonic) |
| Generalised non-motor (absence) | Typical, atypical, myoclonic absence, eyelid myoclonia | Brief staring spells (5–30 sec), abrupt onset/offset, no post-ictal confusion; easily provoked by hyperventilation; common in children aged 4–12 | Generalised 3 Hz spike-and-wave (typical); hyperventilation activates |
| Unknown onset | Motor, non-motor, unclassified | When onset cannot be determined clinically or on EEG | Non-localising or insufficient data |
Common Epilepsy Syndromes
Epilepsy syndromes are defined by a cluster of clinical and EEG features including seizure type(s), age of onset, EEG pattern, comorbidities, and prognosis. Syndrome identification guides ASM selection and prognosis counselling.
| Syndrome | Age of Onset | Key Features | First-Line Treatment | Prognosis |
|---|---|---|---|---|
| Childhood absence epilepsy | 4–10 years | Multiple daily absence seizures; 3 Hz spike-and-wave; normal cognition at onset | Ethosuximide (Zarontin®) or valproate | 60–70% remit by adolescence |
| Juvenile myoclonic epilepsy (JME) | 12–25 years | Morning myoclonic jerks, generalised tonic-clonic seizures; photosensitivity; lifelong ASM usually needed | Valproate (males); levetiracetam (females of childbearing age) | Lifelong; >90% seizure-free on ASMs; relapse on withdrawal common |
| Temporal lobe epilepsy (TLE) | Any age (often childhood–young adult) | Focal impaired awareness seizures with automatisms; epigastric rising aura; MRI may show hippocampal sclerosis | Carbamazepine, lamotrigine, or levetiracetam | 60–70% drug-responsive; surgical candidate if refractory |
| Benign epilepsy with centrotemporal spikes (BECTS / Rolandic) | 3–13 years | Focal seizures (hemifacial, oropharyngeal) often nocturnal; centrotemporal spikes on EEG; normal development | Often no ASM needed; carbamazepine or levetiracetam if seizures frequent | Excellent; remits by age 15–16 |
| Lennox-Gastaut syndrome | 2–8 years | Multiple seizure types (tonic, atonic, atypical absence); intellectual disability; slow spike-and-wave on EEG | Valproate, clobazam, rufinamide, lamotrigine | Poor; refractory epilepsy with developmental impairment |
Red Flags for Secondary Causes
When to Refer to Neurology/Epilepsy Specialist
- All patients with a new diagnosis of epilepsy — specialist confirmation and treatment planning (MBS Item 104 for specialist consultation, or MBS Item 99 for telehealth specialist consultation).
- Diagnostic uncertainty — suspected psychogenic non-epileptic seizures (PNES), which account for 20–30% of referrals to Australian epilepsy clinics.
- Refractory epilepsy — failure of ≥2 appropriate, adequately dosed ASMs (approx. 30% of patients); consider video-EEG monitoring and surgical evaluation.
- Women of childbearing age — pre-conception counselling, ASM optimisation, folate planning.
- Suspected epilepsy syndrome requiring specialist confirmation (e.g., JME, Dravet syndrome).
- Status epilepticus or recurrent cluster seizures.
- Consideration of epilepsy surgery — referral to an accredited epilepsy surgical centre (e.g., Royal Melbourne Hospital, Royal Prince Alfred Hospital, Austin Health, Mater Brisbane, Royal Adelaide Hospital).
Antiseizure Medication Initiation
When to Start Antiseizure Medication
ASM initiation is recommended after a confirmed diagnosis of epilepsy (≥2 unprovoked seizures or high recurrence risk after one seizure). The decision is individualised and considers seizure type, epilepsy syndrome, patient preference, comorbidities, reproductive plans, and driving needs.
Drug Selection by Seizure Type
| Seizure Type / Syndrome | First-Line ASMs | Second-Line / Adjunctive ASMs | ASMs to AVOID |
|---|---|---|---|
| Focal seizures (aware or impaired awareness) | Levetiracetam, carbamazepine, lamotrigine, lacosamide | Clobazam, topiramate, zonisamide, oxcarbazepine, perampanel | Sodium valproate in women of childbearing potential |
| Generalised tonic-clonic seizures | Sodium valproate, levetiracetam | Lamotrigine, topiramate, perampanel | Carbamazepine, oxcarbazepine, phenytoin, gabapentin (may worsen myoclonic/absence) |
| Absence seizures | Ethosuximide, sodium valproate | Lamotrigine | Carbamazepine, oxcarbazepine, phenytoin, gabapentin, vigabatrin (may worsen absence) |
| Myoclonic seizures (JME) | Sodium valproate (males), levetiracetam | Clobazam, topiramate, zonisamide, lamotrigine (partial efficacy) | Carbamazepine, oxcarbazepine, phenytoin, gabapentin, pregabalin (exacerbate myoclonus) |
| Atonic / tonic seizures (Lennox-Gastaut) | Sodium valproate, clobazam | Rufinamide, lamotrigine, topiramate, cannabidiol (Epidyolex® — TGA Special Access Scheme) | Carbamazepine, oxcarbazepine |
First-Line Antiseizure Medications — Drug Cards
Titration and Monitoring
- Start low, go slow: All ASMs should be initiated at a low dose and titrated gradually to minimise adverse effects and identify the lowest effective dose.
- Baseline investigations before starting ASM: FBC, LFTs, renal function, electrolytes. For carbamazepine/phenytoin: consider HLA testing. For valproate: pregnancy test in women of childbearing age; weight; counselling re: teratogenicity.
- Therapeutic drug monitoring (TDM): Not routinely needed for levetiracetam or lamotrigine. Indicated for: phenytoin (narrow therapeutic index: 10–20 mg/L), carbamazepine (4–12 mg/L), valproate (50–100 mg/L), and when non-adherence, toxicity, drug interactions, pregnancy, or renal/hepatic changes alter pharmacokinetics.
- Follow-up: Review at 4–6 weeks after initiation, then 3-monthly until stable, then 6–12-monthly. Assess seizure frequency, adverse effects, driving status, mood/cognition, and adherence at every visit.
- When to switch or add: If seizures persist at maximum tolerated monotherapy dose, consider switching to an alternative appropriate ASM (preferred) or adding a second ASM if seizures are close to controlled and the patient is tolerating treatment.
Emergency Seizure Management
Acute Generalised Convulsive Seizure
Most generalised tonic-clonic seizures are self-limiting (duration 1–3 minutes). Immediate management focuses on airway protection, injury prevention, and monitoring. Pharmacological intervention is required if the seizure persists >5 minutes.
Status Epilepticus — Definition
Pre-Hospital Algorithm (0–5 minutes)
Emergency Department Algorithm (5–30 minutes)
IV Levetiracetam 60 mg/kg (max 4500 mg) over 15 min — preferred (safest profile) OR
IV Sodium valproate 40 mg/kg (max 3000 mg) over 5–10 min — avoid in women of childbearing age, hepatic disease, suspected metabolic disorder OR
IV Fosphenytoin 20 mg PE/kg at max 150 mg PE/min — risk of hypotension, arrhythmia; cardiac monitoring required. Contraindicated with suspected cardiac conduction abnormality.
Midazolam infusion 0.2 mg/kg bolus, then 0.05–2 mg/kg/hr OR
Propofol 2 mg/kg bolus, then 2–10 mg/kg/hr (caution: propofol infusion syndrome if >48 hrs or >5 mg/kg/hr) OR
Thiopentone 3–5 mg/kg bolus, then 3–5 mg/kg/hr
Continuous EEG monitoring is essential. Aim for burst suppression or seizure cessation on EEG.
Post-Status Epilepticus Management
- Admit to HDU/ICU for at least 24 hours monitoring.
- Continuous EEG monitoring if available — NCSE may persist without clinical signs in 15–20% of cases.
- Identify and treat precipitant: infection, metabolic derangement, ASM non-adherence, alcohol withdrawal, intracranial pathology.
- Review and optimise ASM regimen. MRI brain when clinically stable.
- Referral to neurology/epileptology for all patients with status epilepticus.
Seizure First Aid — Patient Education
Women with Epilepsy
Epilepsy management in women requires particular attention to hormonal interactions, contraception efficacy, teratogenic risk, pregnancy planning, and breastfeeding. Up to 50% of pregnancies in women with epilepsy are unplanned, making proactive counselling at every consultation essential.
Contraception and ASM Interactions
Enzyme-inducing ASMs reduce the efficacy of hormonal contraception, increasing unintended pregnancy risk. Non-enzyme-inducing ASMs have no clinically significant interaction with contraception.
| ASM | Effect on Contraception | Recommended Contraception |
|---|---|---|
| Levetiracetam, valproate, ethosuximide, gabapentin, pregabalin, lacosamide, zonisamide, clobazam | No significant interaction | Standard contraceptive options including combined oral contraceptive pill, progestogen-only pill, implant, IUD, depot |
| Carbamazepine, phenytoin, phenobarbitone, oxcarbazepine, eslicarbazepine | Reduced efficacy of hormonal contraception (COC, POP, implant, depot) | Levonorgestrel IUD (Mirena®) — most reliable; or copper IUD; if using COC, use ≥50 µg ethinyloestradiol with continuous use (no pill-free week); or double-dose progestogen; barrier methods as adjunct |
| Lamotrigine + COC | COC reduces lamotrigine levels by ~50% (risk of breakthrough seizures); lamotrigine does not affect COC efficacy | Monitor lamotrigine levels when starting/stopping COC. Consider IUD or progestogen-only alternatives. If COC used, consider increasing lamotrigine dose during active pill phase. |
| Topiramate >200 mg/day | Reduces COC efficacy | IUD, barrier methods, or alternative non-hormonal methods |
Pregnancy Planning and Teratogenic Risk
Teratogenic Risk by ASM
| ASM | Major Congenital Malformation Risk | Neurodevelopmental Risk | Pregnancy Recommendation |
|---|---|---|---|
| Valproate | 5–10% (dose-dependent; >1500 mg/day highest risk) | 30–40% risk of ASD, IQ reduction 7–10 points | CONTRAINDICATED in pregnancy. Switch to alternative ASM before conception if possible. |
| Phenobarbitone | 6–7% | Increased risk of cognitive effects | Avoid if possible; use lowest effective dose |
| Phenytoin | ~6% | Some evidence of neurodevelopmental risk | Avoid if possible; switch to levetiracetam or lamotrigine |
| Carbamazepine | ~4.5% (neural tube defect risk ~0.5–1%) | Limited evidence of neurodevelopmental risk at low doses | Acceptable if needed; lowest effective dose; folic acid 5 mg/day |
| Lamotrigine | ~2–3% | No evidence of neurodevelopmental harm | Preferred ASM in pregnancy. Monitor levels — clearance increases 50–100% by third trimester. |
| Levetiracetam | ~2% | No evidence of neurodevelopmental harm | Preferred ASM in pregnancy. Minimal protein binding; no teratogenic signal in large registries. |
Folate Supplementation
Pre-Conception Checklist
- Review ASM regimen — switch from valproate to levetiracetam or lamotrigine where possible, ideally ≥3 months before conception.
- Commence folic acid 5 mg daily — at least 1 month before conception.
- Optimise seizure control — seizure freedom before pregnancy reduces perinatal risk more than ASM changes.
- Document baseline ASM levels (especially lamotrigine) for comparison during pregnancy.
- Ensure effective contraception during transition to pregnancy-safe ASM regimen.
- Counsel regarding: seizure risk during pregnancy (~25–30% may have increased seizure frequency, often due to non-adherence or pharmacokinetic changes); risks of seizures vs risks of ASM; management during labour and delivery.
- Referral to maternal-fetal medicine or combined obstetric-epilepsy clinic at tertiary centre.
Antenatal Monitoring
- Lamotrigine and levetiracetam levels: Check at baseline pre-pregnancy, then monthly during pregnancy and at 2-weekly intervals from 28 weeks. Dose may need to be increased 50–100% to maintain pre-pregnancy levels. Check levels again at 2–4 weeks postpartum (levels fall rapidly; dose reduction needed to avoid toxicity).
- Obstetric ultrasound: Detailed morphology scan at 18–20 weeks (fetal anomaly screening — particularly neural tube defects for those on valproate or carbamazepine historically).
- Fetal monitoring: Low threshold for fetal monitoring if seizure occurs in pregnancy; CTG monitoring during labour if seizure occurs in third trimester.
Labour, Delivery, and Postnatal
- Continue ASMs throughout labour (oral or via NG if vomiting). Consider IV preparation if prolonged labour and oral intake impaired (levetiracetam IV, valproate IV available; carbamazepine has no IV formulation).
- Seizures during labour: IV lorazepam 4 mg or diazepam 10 mg.
- Vitamin K 1 mg IM for the neonate (standard) — ASMs that induce enzymes may reduce neonatal vitamin K-dependent clotting factors.
- Breastfeeding is encouraged for all ASMs. Levetiracetam, lamotrigine, and carbamazepine are compatible. Monitor infant for drowsiness, poor feeding, or rash.
- Postnatal dose adjustments: lamotrigine dose may need rapid reduction post-delivery; monitor levels at 2 and 6 weeks postpartum.
- Psychosocial support: screen for postnatal depression (higher risk in women with epilepsy); ensure safe infant care practices (bathing supervision, avoid co-sleeping if uncontrolled seizures).
Catamenial Epilepsy
Seizure exacerbation in relation to the menstrual cycle occurs in approximately 10–40% of women with epilepsy. Two patterns are recognised: perimenstrual (catamenial type 1 — seizure clustering around menses due to declining progesterone and oestrogen ratio) and periovulatory (catamenial type 2 — seizure clustering around ovulation due to oestrogen surge). Management options include: clobazam 10–20 mg/day for 10–14 days perimenstrually ("luteal-phase rescue"); hormonal strategies (levonorgestrel IUD, combined oral contraceptive pill); or ASM dose adjustment guided by specialist.
Special Populations
Paediatric Epilepsy
Elderly Patients (≥65 years)
Renal Impairment
Hepatic Impairment
Immunocompromised Patients
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander Australians experience a higher burden of epilepsy, status epilepticus, and epilepsy-related mortality compared to non-Indigenous Australians. Contributing factors include higher rates of traumatic brain injury, CNS infections (particularly in remote communities), perinatal complications, substance use (including petrol sniffing-related brain injury in some communities), and limited access to neurological services. Culturally safe, trauma-informed care is essential.
📚 References
- 1. Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy (ILAE) and the Bureau for Epilepsy. Epilepsia. 2017;58(4):522–530.
- 2. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482.
- 3. Australasian Chapter of Sexual Health Medicine, RACP. Epilepsy guidelines for Australian clinical practice. Epilepsy Society of Australia; 2023.
- 4. Austroads. Assessing Fitness to Drive. 4th ed. Sydney: Austroads; 2022. Available from: austroads.com.au.
- 5. Brodie MJ, Zuberi SM, Scheffer IE, et al. The 2017 ILAE classification of seizure types and the epilepsies: what do clinicians need to know? Epileptic Disord. 2018;20(2):77–85.
- 6. Glauser T, Shinnar S, Gloss D, et al. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults. Neurology. 2016;86(20):1936–1947.
- 7. Tomson T, Battino D, Bonizzoni E, et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: a prospective cohort study of the EURAP registry. Lancet Neurol. 2018;17(6):530–538.
- 8. Meador KJ, Baker GA, Browning N, et al. Fetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD study). Lancet Neurol. 2013;12(3):244–252.
- 9. Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG). Antiepileptic medication use during pregnancy. Clinical Guideline C-Obs 51. Melbourne: RANZCOG; 2023.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework: Epilepsy and neurological conditions. Canberra: AIHW; 2023.
- 11. Beghi E, Giussani G, Sander JW. The natural history and prognosis of epilepsy. Epileptic Disord. 2015;17(3):243–253.
- 12. Scheffer IE, Berkovic S, Capovilla G, et al. ILAE classification of the epilepsies: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):512–521.
- 13. Medicines and Healthcare Products Regulatory Agency (MHRA). Valproate Pregnancy Prevention Programme: toolkit for healthcare professionals. London: MHRA; 2023.
- 14. Panayiotopoulos CP. A Clinical Guide to Epileptic Syndromes and Their Treatment. 2nd ed. London: Springer; 2010.
- 15. Harden CL, Pennell PB, Koppel BS, et al. Practice parameter update: management issues for women with epilepsy — focus on pregnancy. Neurology. 2009;73(2):126–132.