📋 Key Information Summary
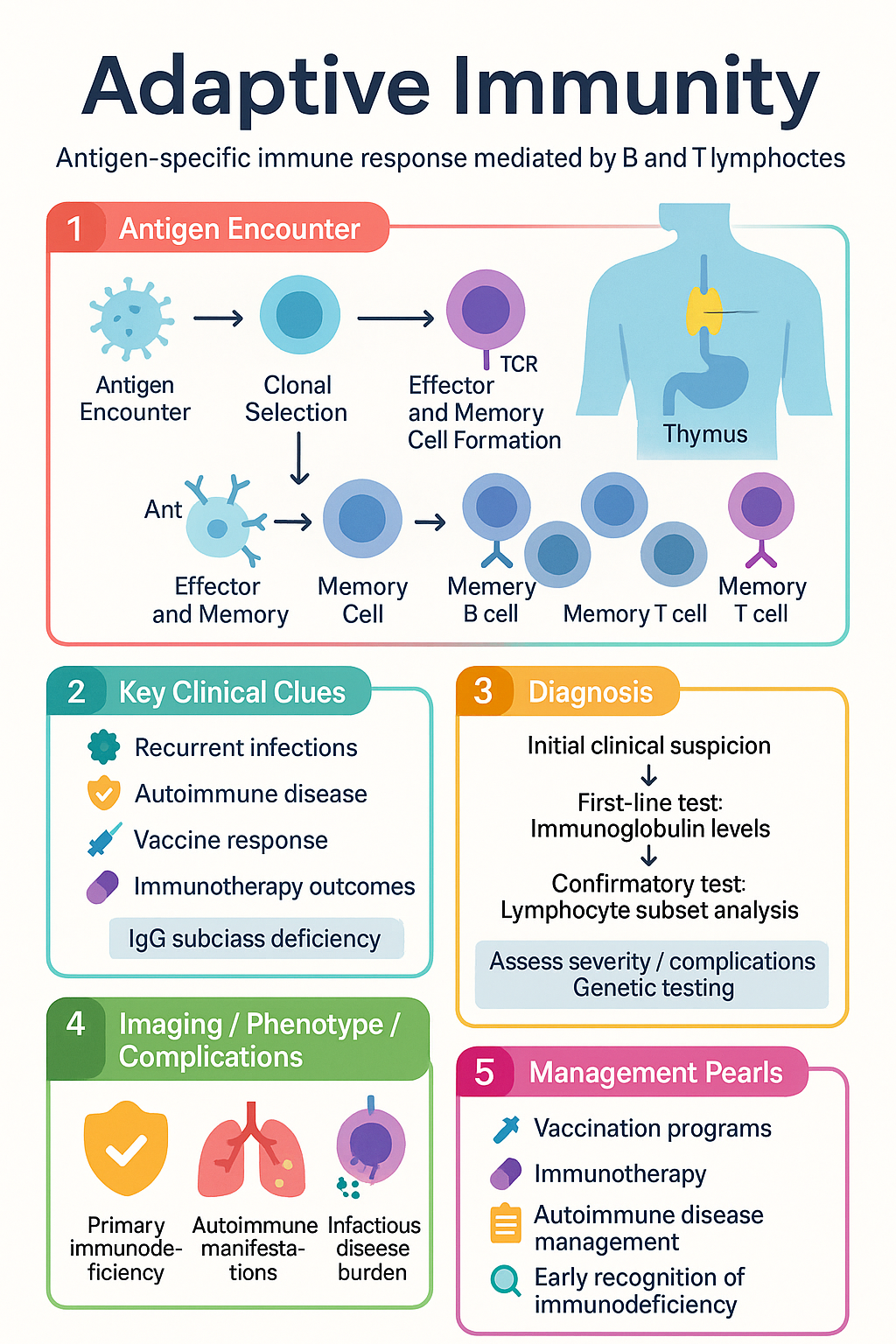
- Adaptive immunity is an antigen-specific, learned immune response mediated by B and T lymphocytes that develops after initial antigen encounter.
- Two major arms: humoral immunity (B-cell–derived antibodies) and cell-mediated immunity (T-cell effector functions).
- Clonal selection ensures each lymphocyte carries a unique antigen receptor; antigen encounter triggers selective proliferation of the reactive clone.
- Immunological memory enables faster, stronger secondary responses on re-exposure — the basis of vaccination.
- Antibody classes (IgG, IgA, IgM, IgE, IgD) have distinct effector functions: neutralisation, opsonisation, complement activation, and mucosal defence.
- CD8⁺ cytotoxic T lymphocytes (CTLs) eliminate virus-infected and tumour cells via perforin/granzyme and Fas–FasL pathways.
- CD4⁺ helper T cells differentiate into functional subsets (Th1, Th2, Th17, Tfh, Treg) that direct the nature of the immune response.
- T-cell activation requires two signals: TCR–MHC peptide interaction (Signal 1) and co-stimulation via CD28–B7 (Signal 2).
- Central tolerance (thymic selection) and peripheral tolerance (Tregs, anergy, deletion) prevent autoimmunity.
- Primary immunodeficiencies affecting adaptive immunity (e.g., X-linked agammaglobulinaemia, severe combined immunodeficiency) present with recurrent, severe, or opportunistic infections.
- Immunological principles underpin clinical vaccination programmes, transplant matching, autoimmune disease management, and immunotherapy in oncology.
- Australian Aboriginal and Torres Strait Islander populations experience disproportionate infectious disease burden; timely vaccination and early immunodeficiency recognition are critical.
Introduction & Australian Context
Adaptive immunity is the antigen-specific arm of the vertebrate immune system, mediated by B and T lymphocytes. Unlike innate immunity — which responds rapidly but non-specifically — adaptive immunity is characterised by exquisite antigen specificity, clonal expansion, immunological memory, and self/non-self discrimination. These features enable the immune system to mount tailored responses against an essentially infinite repertoire of pathogens while maintaining tolerance to host tissues.
In Australia, adaptive immune function is clinically relevant across multiple domains. The National Immunisation Program (NIP) leverages immunological memory to protect against 13+ vaccine-preventable diseases from birth. Autoimmune conditions — including rheumatoid arthritis, type 1 diabetes mellitus, and multiple sclerosis — collectively affect more than 1 million Australians. Primary immunodeficiencies, though individually rare, have an estimated combined prevalence of 1 in 1,200 to 1 in 2,000 Australians, with significant diagnostic delay (median 5–7 years).
Understanding the mechanisms of adaptive immunity is essential for clinicians managing infectious disease, autoimmunity, transplantation, and the expanding field of immuno-oncology. This guideline reviews the key components, effector arms, clonal selection principles, and memory formation that underpin adaptive immune function, with attention to clinical relevance in the Australian healthcare context.
Key Components of Adaptive Immunity
The adaptive immune system comprises specialised cells, molecules, and organised lymphoid tissues that together generate antigen-specific responses.
Lymphocytes
- B lymphocytes (B cells): Derived from haematopoietic stem cells; mature in the bone marrow. Responsible for antibody production, antigen presentation, and cytokine secretion. Surface immunoglobulin (B-cell receptor, BCR) serves as the antigen-specific receptor.
- T lymphocytes (T cells): Derived from bone marrow progenitors; mature in the thymus. Express the T-cell receptor (TCR), which recognises processed antigen fragments presented by major histocompatibility complex (MHC) molecules. Subsets include CD4⁺ helper T cells, CD8⁺ cytotoxic T cells, and regulatory T cells (Tregs).
- Natural killer (NK) cells: While generally classified as innate lymphocytes, a subset of memory NK cells has been identified, blurring the traditional innate/adaptive boundary.
Antigen Receptors & Diversity
Diversity of the BCR and TCR repertoires is generated during lymphocyte development through:
- V(D)J recombination: Somatic rearrangement of variable (V), diversity (D), and joining (J) gene segments, catalysed by RAG-1 and RAG-2 recombinases. This process can theoretically generate >10¹¹ unique receptors.
- Junctional diversity: Random nucleotide addition (N-nucleotides by TdT) and deletion at gene segment junctions further increases receptor variability.
- Somatic hypermutation (B cells only): Point mutations introduced into immunoglobulin variable regions during germinal centre reactions, enabling affinity maturation.
Antigen Presentation
| Feature | MHC Class I | MHC Class II |
|---|---|---|
| Expressed on | All nucleated cells | Professional APCs (dendritic cells, macrophages, B cells) |
| Presents to | CD8⁺ T cells | CD4⁺ T cells |
| Antigen source | Endogenous (intracellular proteins, viral antigens) | Exogenous (phagocytosed extracellular antigens) |
| Processing pathway | Proteasomal degradation → TAP → ER loading | Endosomal/lysosomal degradation → MIIC loading |
| HLA genes (Australia) | HLA-A, HLA-B, HLA-C | HLA-DR, HLA-DP, HLA-DQ |
Lymphoid Tissues
- Primary (central): Bone marrow (B-cell maturation) and thymus (T-cell maturation and selection).
- Secondary (peripheral): Spleen, lymph nodes, mucosa-associated lymphoid tissue (MALT), including Peyer's patches, tonsils, and bronchial-associated lymphoid tissue (BALT). These are the sites of antigen encounter and adaptive response initiation.
Humoral vs Cell-Mediated Immunity
Adaptive immunity is functionally divided into two complementary arms, each targeting distinct categories of pathogen.
Humoral Immunity (Antibody-Mediated)
Humoral immunity is primarily directed against extracellular pathogens and soluble antigens. B cells, upon activation by antigen and T-cell help (T-dependent responses), undergo clonal expansion and differentiate into antibody-secreting plasma cells and long-lived memory B cells.
Immunoglobulin Classes & Clinical Functions
| Isotype | Key Functions | Clinical Relevance |
|---|---|---|
| IgG | Opsonisation, complement activation (classical pathway), neonatal Fc receptor–mediated placental transfer, ADCC | Most abundant serum Ig; four subclasses (IgG1–4). Deficiency predisposes to sinopulmonary infections. Crosses placenta — basis of haemolytic disease of the newborn (anti-D). |
| IgA | Mucosal defence (secretory IgA), neutralisation, immune exclusion | Predominant mucosal Ab. Selective IgA deficiency (~1:500) — most common primary immunodeficiency; often asymptomatic but may cause recurrent GI/respiratory infections. |
| IgM | Pentameric structure; potent complement activation; first Ab in primary response | Elevated in acute infection (IgM serology). Does not cross placenta. Key in ABO blood group incompatibility. |
| IgE | Mast cell and basophil degranulation; anti-helminth defence | Central to type I hypersensitivity (allergic rhinitis, asthma, anaphylaxis). Elevated in atopy and parasitic infection. Target of omalizumab (Xolair®) therapy. |
| IgD | Co-expressed with IgM on naïve B cells; role in B-cell activation unclear | Low serum concentration; limited direct clinical application. |
Cell-Mediated Immunity
Cell-mediated immunity is directed primarily against intracellular pathogens (viruses, intracellular bacteria such as Mycobacterium tuberculosis, and tumour cells) and is the principal mechanism of transplant rejection and contact hypersensitivity.
Key Effector Mechanisms
- CD8⁺ cytotoxic T lymphocytes (CTLs): Recognise intracellular antigen presented on MHC class I. Kill target cells via perforin/granzyme exocytosis (granule exocytosis pathway) and Fas–FasL interaction. Essential for viral clearance and anti-tumour surveillance.
- CD4⁺ Th1 cells: Secrete IFN-γ and TNF-α, activating macrophages to kill phagocytosed intracellular organisms (e.g., M. tuberculosis, Leishmania). IFN-γ upregulates MHC class II and enhances antigen presentation.
- CD4⁺ Th2 cells: Secrete IL-4, IL-5, IL-13. Drive B-cell class switching to IgE, eosinophil activation, and mucus production. Central to helminth defence and allergic disease.
- CD4⁺ Th17 cells: Secrete IL-17A, IL-17F, IL-22. Recruit neutrophils; important in mucosal defence against extracellular bacteria and fungi. Dysregulation linked to psoriasis, ankylosing spondylitis, and inflammatory bowel disease.
- T follicular helper (Tfh) cells: Located in germinal centres; provide critical signals (IL-21, CD40L) for B-cell affinity maturation and class-switch recombination.
- Regulatory T cells (Tregs): CD4⁺CD25⁺FoxP3⁺ cells that suppress immune responses via IL-10, TGF-β secretion, and CTLA-4–mediated inhibition. Essential for peripheral tolerance and prevention of autoimmunity.
Comparison Summary
| Feature | Humoral Immunity | Cell-Mediated Immunity |
|---|---|---|
| Primary effector | B cells → plasma cells → antibodies | T cells (CD4⁺ helper, CD8⁺ cytotoxic) |
| Target | Extracellular pathogens, toxins, free antigens | Intracellular pathogens, tumour cells, transplant antigens |
| Antigen recognition | Native (unprocessed) antigen via BCR | Processed antigen via TCR + MHC |
| Transfer | Passive transfer possible (serum, IVIg) | Passive transfer possible (adoptive cell therapy, donor lymphocyte infusion) |
| Memory | Memory B cells, long-lived plasma cells | Central memory T cells, effector memory T cells, tissue-resident memory T cells |
Clonal Selection & Expansion
The clonal selection theory, proposed by Frank Macfarlane Burnet (Nobel Prize, 1960 — a landmark Australian contribution to immunology), is the central organising principle of adaptive immunity. It holds that each lymphocyte expresses a unique antigen receptor generated somatically before antigen encounter, and that antigen selects and drives the proliferation of only those clones whose receptors bind it.
The Clonal Selection Process
Clonal Anergy & Peripheral Tolerance
Lymphocytes that encounter antigen without adequate co-stimulation enter a state of functional unresponsiveness (clonal anergy) rather than activation. This peripheral tolerance mechanism protects against autoimmunity when self-antigens are encountered outside the thymus. Additional peripheral tolerance mechanisms include:
- Treg-mediated suppression: FoxP3⁺ Tregs inhibit autoreactive T cells via IL-10, TGF-β, CTLA-4, and IL-2 consumption.
- Activation-induced cell death (AICD): Repeated TCR stimulation upregulates Fas and FasL, triggering apoptosis of chronically stimulated lymphocytes.
- Immune checkpoint pathways: PD-1–PD-L1 and CTLA-4–B7 interactions deliver inhibitory signals that limit T-cell activation. These pathways are therapeutically targeted by checkpoint inhibitor immunotherapy in oncology (e.g., pembrolizumab [Keytruda®], nivolumab [Opdivo®] — both PBS-listed for multiple tumour types in Australia).
Immunological Memory
Immunological memory is the hallmark of adaptive immunity — the capacity to mount a faster, stronger, and more effective response upon re-encountering a previously experienced antigen. This property is the immunological basis of vaccination and underpins the success of Australia's National Immunisation Program (NIP).
Primary vs Secondary Immune Response
| Feature | Primary Response | Secondary (Memory) Response |
|---|---|---|
| Lag phase | 5–10 days | 1–3 days |
| Peak response | Lower magnitude | 10–100× greater magnitude |
| Predominant isotype | IgM (then IgG late) | IgG (or IgA, IgE depending on prior class switch) |
| Antibody affinity | Lower (pre-affinity maturation) | Higher (affinity-matured) |
| Responding cells | Naïve lymphocytes | Memory lymphocytes (lower activation threshold, faster proliferation) |
| Duration | Declines relatively rapidly | Sustained high titres; long-lived plasma cells in bone marrow |
Memory B Cells
Memory B cells are generated in germinal centres through somatic hypermutation and affinity-based selection. Key features:
- Express class-switched (IgG, IgA, IgE) and affinity-matured BCRs.
- Lower activation threshold than naïve B cells — respond to lower antigen concentrations.
- Rapidly differentiate into high-affinity antibody-secreting plasma cells upon re-stimulation.
- Long-lived plasma cells reside in bone marrow survival niches and secrete antibody constitutively for decades (e.g., anti-measles IgG persists for life).
Memory T Cells
Memory T cells comprise several functionally distinct subsets:
- Central memory T cells (Tcm): Express CCR7 and CD62L; circulate through secondary lymphoid organs. Proliferate rapidly upon re-stimulation. Sustained by IL-7 and IL-15.
- Effector memory T cells (Tem): Lack CCR7; patrol peripheral tissues. Provide immediate effector function (cytokine secretion, cytotoxicity) at sites of infection.
- Tissue-resident memory T cells (Trm): Permanently reside in barrier tissues (skin, lung, gut mucosa). Express CD69 and CD103. Provide rapid local defence upon pathogen re-encounter — particularly important in respiratory and mucosal immunity.
- Stem cell memory T cells (Tscm): Rare population with self-renewal capacity and the ability to generate all other memory subsets. Under investigation in adoptive cell therapy for cancer.
Clinical Applications of Immunological Memory
Vaccination — The National Immunisation Program (Australia)
Vaccines exploit immunological memory by exposing the host to attenuated, inactivated, or subunit antigens that prime adaptive immunity without causing disease. The Australian NIP provides funded vaccines against 13+ diseases from birth through to adulthood, with schedule catch-up provisions for Aboriginal and Torres Strait Islander children and other high-risk groups.
- Live attenuated vaccines (e.g., MMR, varicella, BCG): Elicit robust, durable humoral and cell-mediated memory. Generally contraindicated in immunocompromised patients and pregnancy.
- Inactivated/killed vaccines (e.g., influenza, hepatitis A): Primarily induce humoral memory; booster doses often required.
- Subunit/conjugate vaccines (e.g., pneumococcal conjugate [PCV13], meningococcal ACWY/B): Target specific antigens; conjugation to carrier protein converts T-independent to T-dependent response, enabling immunological memory and class switching.
- mRNA vaccines (e.g., Comirnaty®, Spikevax® — COVID-19): Encode antigen for endogenous expression; elicit both antibody and T-cell memory. Rapid platform enabling variant-adapted boosters.
Immunodeficiency & Impaired Memory
Defects in adaptive immune memory formation result in susceptibility to recurrent infections. Key examples:
Clinical Applications & Investigations
Assessment of adaptive immune function is relevant in the investigation of recurrent infections, autoimmune disease, transplant immunology, and immunotherapy response monitoring.
Laboratory Assessment of Adaptive Immunity
Therapeutic Targeting of Adaptive Immunity
| Therapy Category | Examples (Australian Brands) | Mechanism | PBS Status |
|---|---|---|---|
| Immunoglobulin replacement | Intragam® P (CSL), Evogam® (CSL), HyQvia® (Takeda) | Pooled human IgG; passive humoral immunity | Authority Required |
| Anti-TNF biologics | Adalimumab (Humira®), Infliximab (Remicade®) | Neutralise TNF-α; suppress Th1-mediated inflammation | Restricted Benefit |
| Anti-IL-4/IL-13 | Dupilumab (Dupixent®) | Blocks Th2 cytokine signalling | Restricted Benefit |
| Immune checkpoint inhibitors | Pembrolizumab (Keytruda®), Nivolumab (Opdivo®) | Block PD-1 → reinvigorate anti-tumour T-cell responses | Restricted Benefit |
| Anti-CD20 (B-cell depletion) | Rituximab (MabThera®) | Depletes CD20⁺ B cells; reduces autoantibody production | Restricted Benefit |
| Calcineurin inhibitors | Ciclosporin (Neoral®), Tacrolimus (Prograf®) | Inhibit calcineurin → block IL-2 transcription → suppress T-cell activation | General Benefit |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of infectious and immune-mediated disease. Understanding the intersection of adaptive immunity with social determinants of health is essential for equitable clinical care.
📚 References
- 1. Murphy K, Weaver C. Janeway's Immunobiology. 10th ed. New York: Garland Science; 2022.
- 2. Abbas AK, Lichtman AH, Pillai S. Cellular and Molecular Immunology. 10th ed. Philadelphia: Elsevier; 2022.
- 3. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health and Aged Care. Updated 2024. Available at: immunisationhandbook.health.gov.au.
- 4. National Health and Medical Research Council (NHMRC). National Immunisation Program Schedule. Australian Government; 2024.
- 5. Tangye SG, Al-Herz W, Bousfiha A, et al. Human inborn errors of immunity: 2022 update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 2022;42(7):1473–1507.
- 6. Slatter MA, Gennery AR. Hematopoietic cell transplantation for primary immunodeficiency. Hematol Oncol Clin North Am. 2023;37(4):743–760.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework. Canberra: AIHW; 2023.
- 8. RHDAustralia (RHD Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Menzies School of Health Research; 2020.
- 9. Farber DL, Netea MG, Radbruch A, Rajewsky K, Zinkernagel RM. Immunological memory: lessons from the past and a look to the future. Nat Rev Immunol. 2016;16(2):124–128.
- 10. Burnet FM. The Clonal Selection Theory of Acquired Immunity. Cambridge: Cambridge University Press; 1959.
- 11. Doherty PC, Zinkernagel RM. A biological role for the major histocompatibility antigens. Lancet. 1975;1(7922):1406–1409.
- 12. Pockley AG, Bhatt DL, Olesen OD. Immunosenescence and its clinical implications. Nat Rev Immunol. 2023;23(8):501–514.
- 13. Australasian Society of Clinical Immunology and Allergy (ASCIA). ASCIA Guidelines for the investigation and management of primary immunodeficiency. Updated 2023.
- 14. World Health Organization (WHO). Immunological basis for immunization series: module overview and general immunology. Geneva: WHO; 2023.