📋 Key Information Summary
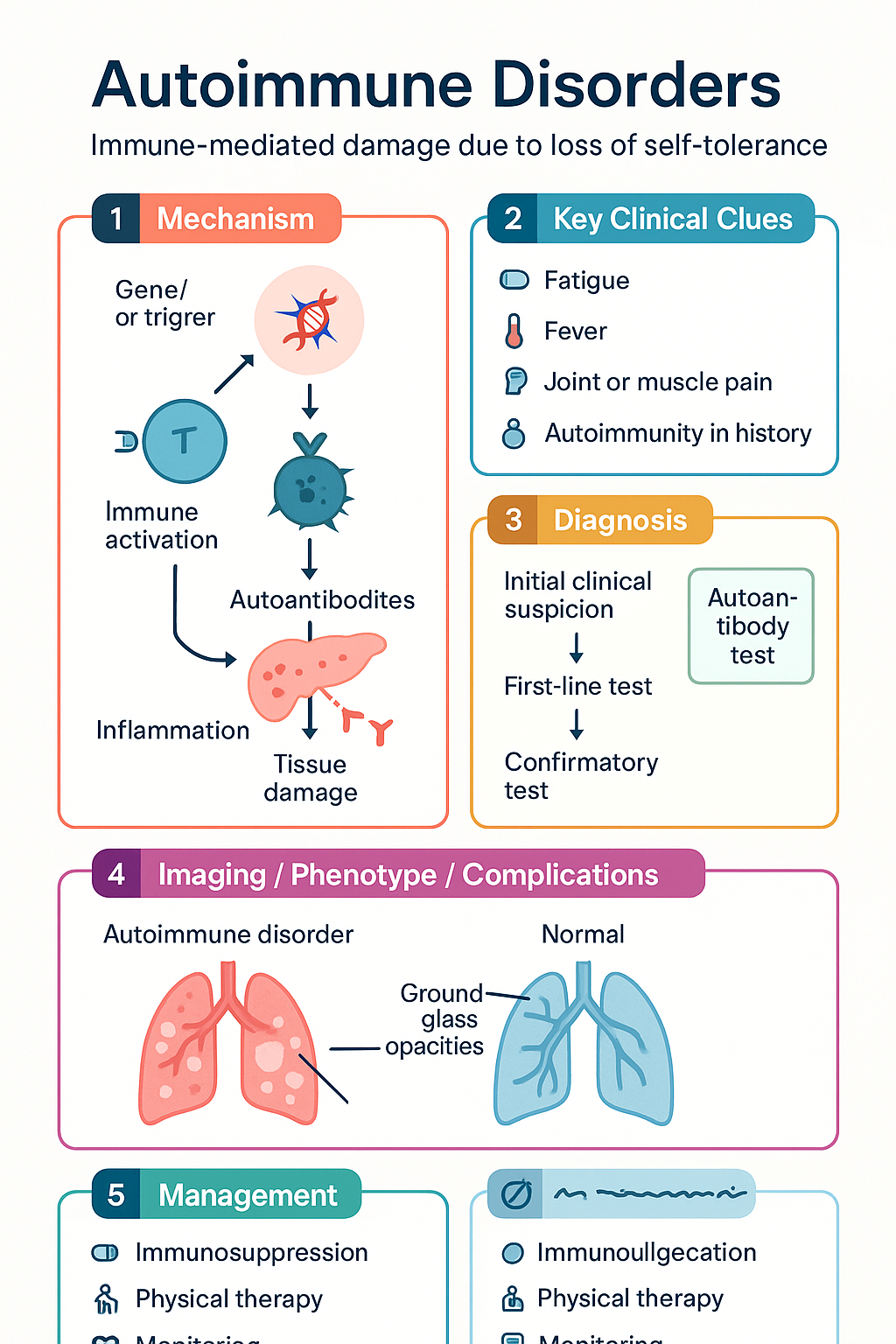
- Autoimmune disorders arise from loss of self-tolerance, leading to immune-mediated damage of specific organs or systemic tissues.
- Broadly classified as organ-specific (e.g., Type 1 diabetes, Hashimoto's thyroiditis) or systemic (e.g., SLE, rheumatoid arthritis).
- Key immunological mechanisms include autoantibody production, immune complex deposition, and T-cell mediated cytotoxicity.
- Diagnosis requires correlation of clinical features with specific autoantibody and inflammatory marker profiles.
- First-line investigations include ANA, RF, anti-CCP, ESR, CRP, and organ-specific antibodies (e.g., anti-TPO, GAD65).
- Treatment is guided by disease type, severity, and organ involvement, using a step-up approach from NSAIDs to DMARDs and biologics.
- Australian PBS restrictions apply to many biologic DMARDs (e.g., adalimumab, rituximab), requiring Authority approval.
- Aboriginal and Torres Strait Islander peoples experience higher prevalence, later diagnosis, and poorer outcomes for many autoimmune conditions.
- Multidisciplinary care involving GPs, rheumatologists, endocrinologists, and allied health is essential for optimal management.
- Key safety alerts include infection risk with immunosuppression and the need for pre-biologic screening (TB, hepatitis B/C).
Introduction & Australian Epidemiology
Autoimmune disorders encompass a diverse group of more than 80 chronic illnesses characterised by a breakdown of immune self-tolerance, leading to inappropriate immune responses against the body's own tissues. In Australia, these conditions represent a significant and growing burden on the healthcare system, affecting approximately 5-8% of the population, with a higher prevalence in women.
The spectrum of disease ranges from isolated organ-specific conditions, such as autoimmune thyroiditis affecting over 1 million Australians, to complex multi-system disorders like systemic lupus erythematosus (SLE). Epidemiological data from the Australian Institute of Health and Welfare (AIHW) indicates that autoimmune diseases are among the leading causes of morbidity in younger and middle-aged adults, particularly impacting workforce participation and quality of life.
While the aetiology is multifactorial, involving genetic susceptibility (e.g., HLA associations), environmental triggers (e.g., infections, smoking), and hormonal factors, the underlying pathogenesis consistently involves dysregulated adaptive immunity. Understanding this classification and pathophysiology is fundamental to guiding rational investigation and targeted therapy in the Australian clinical setting.
Organ-Specific vs Systemic Autoimmune Disorders
A primary clinical classification divides autoimmune disorders based on the pattern of tissue involvement, which directly guides investigation and specialist referral pathways.
| Feature | Organ-Specific | Systemic |
|---|---|---|
| Definition | Immune response targets antigens within a single organ or gland. | Immune response targets antigens widespread in many tissues; inflammation is diffuse. |
| Pathology | Localised destruction or dysfunction of the specific organ. | Widespread inflammation, vasculitis, fibrosis, and immune complex deposition. |
| Australian Examples | • Type 1 Diabetes Mellitus (pancreatic β-cells) • Hashimoto's Thyroiditis & Graves' Disease • Autoimmune Hepatitis • Multiple Sclerosis (CNS myelin) |
• Systemic Lupus Erythematosus (SLE) • Rheumatoid Arthritis (RA) • Sjögren's Syndrome • Systemic Sclerosis (Scleroderma) |
| Typical Antibodies | Organ-specific (e.g., anti-TPO, GAD65, anti-smooth muscle). | Non-organ specific (e.g., ANA, RF, anti-dsDNA, anti-CCP). |
| Primary Specialist | Relevant organ specialist (Endocrinologist, Gastroenterologist, Neurologist). | Rheumatologist (often with other organ specialists). |
Immunological Mechanisms
The tissue damage in autoimmune diseases is mediated by four classical hypersensitivity reaction pathways, often operating concurrently.
Understanding the dominant mechanism helps predict response to therapy. For example, B-cell depleting therapies (e.g., rituximab) are more effective in antibody-driven diseases like RA and ANCA-associated vasculitis.
Investigations
A tiered, clinical-suspicion-driven approach is essential. The following are key investigations available in Australia, with MBS item numbers where commonly billed.
- Antinuclear Antibody (ANA): High sensitivity for SLE (>95%), but low specificity. Positive in many conditions and ~15% of healthy population.
- Extractable Nuclear Antigen (ENA) Panel: Follow-up for positive ANA. Includes anti-Ro (Sjögren's, neonatal lupus), anti-La, anti-Sm (specific for SLE), anti-RNP (mixed connective tissue disease).
- Rheumatoid Factor (RF) & Anti-CCP: Anti-CCP is highly specific (>95%) for Rheumatoid Arthritis.
- Anti-dsDNA: Specific for SLE; titres correlate with disease activity, especially renal involvement.
- ANCA (Anti-neutrophil Cytoplasmic Antibodies): c-ANCA/PR3 for Granulomatosis with polyangiitis (GPA); p-ANCA/MPO for Microscopic polyangiitis (MPA).
Treatment Principles
Management follows a stepwise, treat-to-target approach aiming for remission or low disease activity. Therapy must be individualised based on disease type, severity, comorbidities, and patient preference.
Pharmacological Therapy Pyramid
Key Drug Classes & Australian Considerations
Special Populations
Pregnancy
Paediatrics
ATSI Health Considerations
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Arthritis and other musculoskeletal conditions in Australia. AIHW; 2023.
- 2. Royal Australasian College of Physicians (RACP). Autoimmune Diseases: A National Strategic Plan. 2022.
- 3. Gordon C, et al. The British Society for Rheumatology guideline for the management of systemic lupus erythematosus in adults. Rheumatology. 2018;57(1):e1-e45.
- 4. Smolen JS, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3-18.
- 5. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2024. (Viewed March 2024).
- 6. Pharmaceutical Benefits Scheme (PBS). PBS Schedule. Australian Government Department of Health. Available at: pbs.gov.au. (Accessed 15 March 2024).
- 7. Byron JK, et al. The Australian Lupus Registry and Biobank: ten years of advancing lupus care. Intern Med J. 2021;51(12):2009-2016.
- 8. Eades LE, et al. High prevalence and early onset of chronic comorbidities in Aboriginal and Torres Strait Islander people with systemic lupus erythematosus. Lupus. 2022;31(10):1269-1277.
- 9. Ledingham J, et al. BSR guideline for anti-TNF therapy in rheumatoid arthritis. Rheumatology. 2019;58(6):e3-e42.
- 10. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. 2023 Update. Canberra: NHMRC.