📋 Key Information Summary
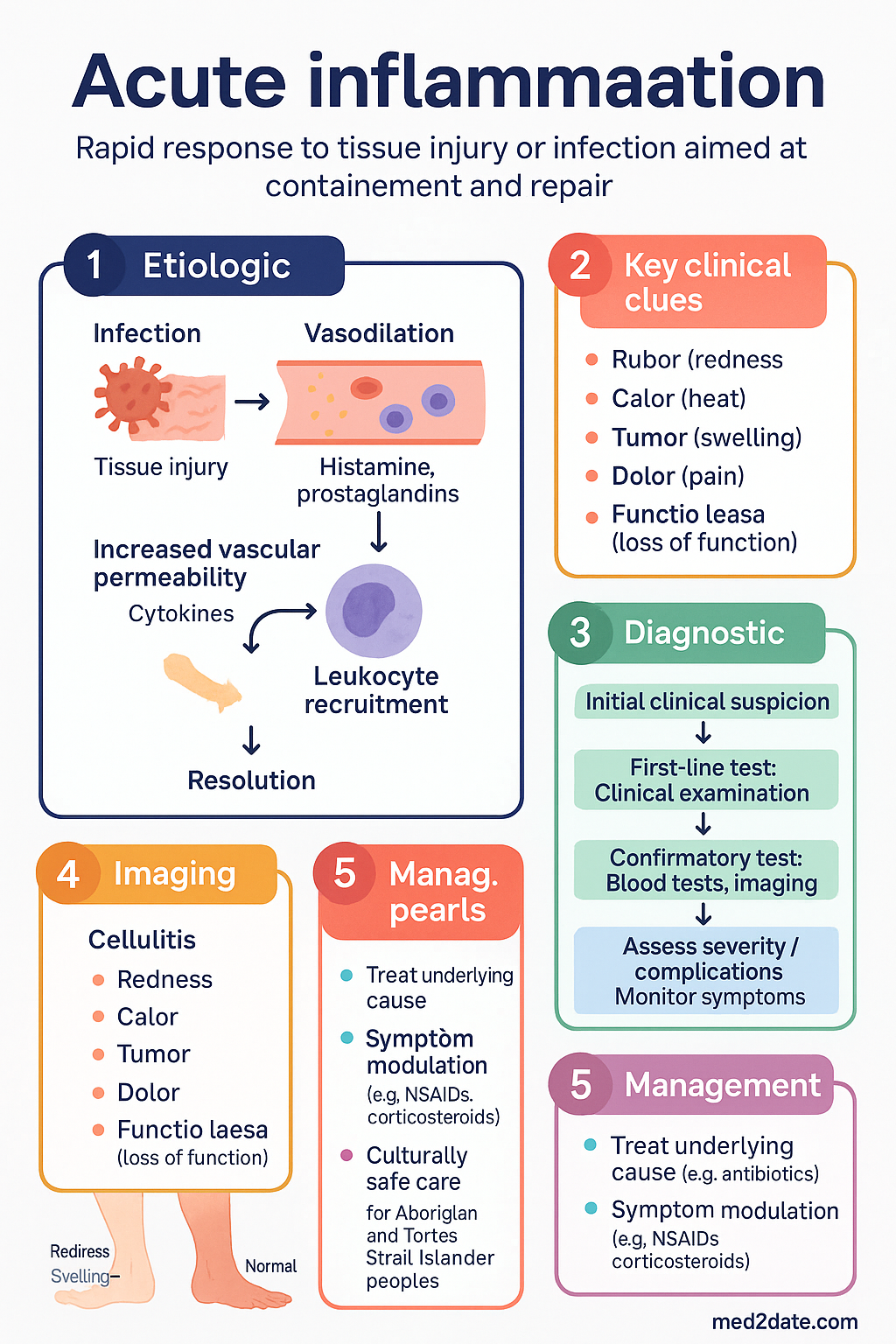
- Acute inflammation is a rapid, stereotyped response to tissue injury or infection, aimed at containing the insult and initiating repair.
- The cardinal signs are rubor (redness), calor (heat), tumor (swelling), dolor (pain), and functio laesa (loss of function).
- Vascular changes begin with transient vasoconstriction followed by sustained vasodilation, increasing blood flow to the area.
- Increased vascular permeability leads to the exudation of protein-rich fluid into the extravascular space, causing oedema.
- Neutrophils are the hallmark leukocyte of acute inflammation, undergoing a sequence of margination, rolling, adhesion, and transmigration (diapedesis).
- Chemical mediators (e.g., histamine, prostaglandins, complement, cytokines) orchestrate the vascular and cellular events.
- Resolution involves clearance of stimuli, neutrophil apoptosis, macrophage-mediated efferocytosis, and tissue restoration.
- Outcomes include complete resolution, healing by fibrosis, abscess formation, or progression to chronic inflammation.
- In Australia, acute inflammatory conditions (e.g., appendicitis, cellulitis, pneumonia) are common reasons for hospital admission and primary care presentation.
- Management focuses on treating the underlying cause (e.g., antibiotics for infection) and modulating symptoms (e.g., NSAIDs, corticosteroids).
- Aboriginal and Torres Strait Islander peoples experience a higher burden of infectious and inflammatory diseases, requiring culturally safe and accessible care.
Introduction & Australian Epidemiology
Acute inflammation is the immediate, early response to tissue injury, whether caused by infection, trauma, toxins, or immune reactions. It is a critical, non-specific defence mechanism designed to localise and eliminate the injurious agent, remove damaged tissue, and create an environment conducive to healing. This process is characterised by exudate formation—accumulation of fluid, proteins, and leukocytes in the affected tissue.
In the Australian context, acute inflammatory conditions represent a significant component of clinical practice across primary, secondary, and tertiary care. Common presentations include:
- Infectious causes: Community-acquired pneumonia, cellulitis, urinary tract infections, and acute gastroenteritis are leading causes of emergency department presentations and hospital admissions.
- Surgical emergencies: Acute appendicitis and cholecystitis are frequent causes of emergency surgery.
- Trauma: Wound healing following injury or surgery involves a carefully orchestrated acute inflammatory phase.
- Immune-mediated: Acute exacerbations of asthma, allergic reactions (e.g., anaphylaxis), and acute flares of autoimmune conditions.
According to the Australian Institute of Health and Welfare (AIHW), diseases of the respiratory system and injury are among the top reasons for hospitalisation, both fundamentally involving acute inflammatory pathways. Furthermore, antimicrobial resistance (AMR) patterns in Australia, such as high rates of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) in remote communities, directly impact the management of infectious causes of inflammation.
Vascular Changes
The vascular response is the earliest phase of acute inflammation, occurring within seconds to minutes. It is primarily mediated by chemical mediators like histamine acting on arteriolar smooth muscle.
1. Vasodilation
This follows a brief period of vasoconstriction. Arteriolar dilation leads to increased blood flow (hyperaemia), causing the cardinal signs of redness (rubor) and heat (calor). The increased hydrostatic pressure contributes to fluid extravasation.
2. Increased Vascular Permeability
This is the dominant cause of the inflammatory exudate. Mediators cause endothelial cell contraction (via actin-myosin), widening intercellular gaps. This allows protein-rich fluid (exudate) to leak into the extravascular space, leading to oedema (tumor). The increased interstitial pressure and specific mediators (e.g., bradykinin) stimulate nerve endings, causing pain (dolor).
Cellular Events
The cellular phase involves the recruitment of leukocytes, predominantly neutrophils, to the site of injury. This sequence is directed by chemical signals.
1. Leukocyte Extravasation
- Margination & Rolling: Neutrophils move to the vessel periphery and loosely interact with selectin molecules on activated endothelium, causing them to roll along the wall.
- Adhesion: Chemokines activate integrins on neutrophils, allowing firm adhesion to endothelial ligands (e.g., ICAM-1).
- Transmigration (Diapedesis): Neutrophils squeeze between endothelial cells, guided by PECAM-1, into the interstitial tissue.
- Chemotaxis: Neutrophils migrate towards the chemical gradient of the injury site (e.g., bacterial products, complement fragments like C5a, cytokines like IL-8).
2. Phagocytosis & Degranulation
Upon arrival, neutrophils recognise and engulf (phagocytose) pathogens or debris, aided by opsonins (e.g., IgG, C3b). They then release reactive oxygen species (ROS) and proteolytic enzymes from their granules to destroy the material.
Chemical Mediators
A complex network of mediators derived from plasma or cells coordinates the inflammatory response. They have overlapping functions and often amplify each other.
| Mediator | Primary Source | Key Actions |
|---|---|---|
| Histamine | Mast cells, basophils, platelets | Immediate, transient vasodilation and increased permeability. |
| Serotonin (5-HT) | Platelets | Vasoconstriction or dilation, platelet aggregation. |
| Prostaglandins (PGs) | Most cells (via COX enzymes) | Vasodilation, pain (sensitise pain receptors), fever. |
| Leukotrienes (LTs) | Leukocytes (via LOX enzyme) | Sustained vasoconstriction, increased permeability, chemotaxis. |
| Complement (C3a, C5a) | Plasma (liver synthesis) | Chemotaxis (C5a), opsonisation (C3b), mast cell degranulation (C3a, C5a). |
| Cytokines (TNF-α, IL-1) | Macrophages, endothelial cells | Systemic effects (fever, acute phase proteins), endothelial activation. |
Pharmacological Targeting: Understanding these mediators guides therapy. Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen inhibit cyclooxygenase (COX), reducing prostaglandin synthesis. Corticosteroids (e.g., prednisolone) inhibit phospholipase A2, reducing production of both prostaglandins and leukotrienes. Antihistamines block histamine receptors.
Resolution & Outcomes
The outcome of acute inflammation is determined by the balance between the injurious agent and the host's ability to mount an appropriate response.
1. Resolution
This is the ideal outcome: complete restoration of normal tissue structure and function. Key steps include:
- Cessation of the inflammatory stimulus.
- Neutrophil apoptosis and cessation of recruitment.
- Efferocytosis: Macrophages clear apoptotic neutrophils and debris, switching to an anti-inflammatory, pro-repair phenotype.
- Drainage of oedema fluid via lymphatics.
- Parenchymal cell regeneration (if the stromal framework remains intact).
2. Other Potential Outcomes
- Healing by Fibrosis (Scarring): Occurs when substantial tissue destruction prevents full regeneration. Common in abscesses or large wounds.
- Abscess Formation: A localised collection of pus walled off by fibrous tissue. Common in bacterial infections (e.g., S. aureus).
- Progression to Chronic Inflammation: If the stimulus persists or the response is dysregulated.
Aboriginal and Torres Strait Islander Health Considerations
Acute inflammatory conditions, particularly those caused by infection, disproportionately affect Aboriginal and Torres Strait Islander peoples. This is due to a complex interplay of social determinants of health, higher prevalence of risk factors (e.g., rheumatic heart disease, diabetes), and barriers to accessing timely healthcare.
📚 References
- 1. Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease. 10th ed. Philadelphia: Elsevier; 2021. Chapter 3: Acute and Chronic Inflammation.
- 2. Australian Institute of Health and Welfare (AIHW). Admitted patient care 2021–22: All diagnoses. Canberra: AIHW; 2023.
- 3. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th ed. East Melbourne: RACGP; 2024.
- 4. Australian Commission on Safety and Quality in Health Care (ACSQHC). Antimicrobial Use and Resistance in Australia (AURA) 2023. Sydney: ACSQHC; 2023.
- 5. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Menzies School of Health Research; 2020.
- 6. Therapeutic Guidelines Limited. eTG complete [Internet]. Melbourne: TGL; 2024. (Used for clinical reference, not cited as a primary source in this guideline).
- 7. Serhan CN, Levy BD. Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators. J Clin Invest. 2018;128(7):2657-2669.
- 8. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and control of infection in healthcare. Canberra: NHMRC; 2019.
- 9. Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603-661.
- 10. Australian Bureau of Statistics (ABS). National Aboriginal and Torres Strait Islander Health Survey. Canberra: ABS; 2022.