📋 Key Information Summary
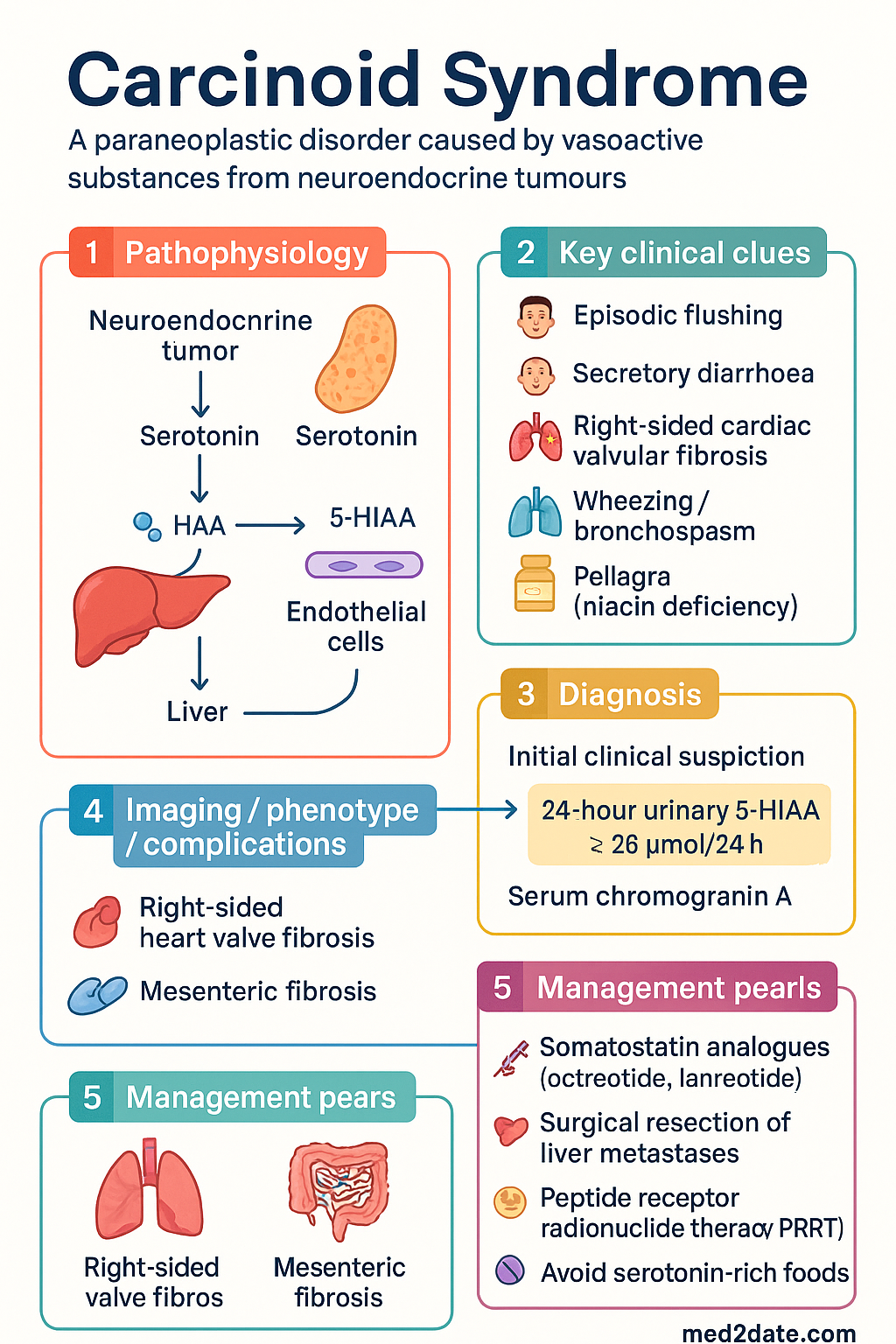
- Definition: Carcinoid syndrome is a paraneoplastic disorder caused by vasoactive substances — predominantly serotonin — released by neuroendocrine tumours (NETs), usually metastatic small-bowel (midgut) carcinoid tumours with hepatic metastases.
- Epidemiology: Age-standardised incidence of gastroenteropancreatic NETs in Australia is approximately 5–7 per 100 000 per year; carcinoid syndrome complicates ~20–30 % of midgut NETs with liver metastases.
- Classic triad: Episodic flushing (face, neck, trunk), secretory diarrhoea (often profuse), and right-sided cardiac valvular fibrosis (carcinoid heart disease).
- Diagnosis: 24-hour urinary 5-HIAA (≥ 26 µmol/24 h in adults) remains the biochemical gold standard; serum chromogranin A supports diagnosis. Imaging with 68Ga-DOTATATE PET/CT (MBS item 61505 — Authority Required) is the preferred staging modality in Australia.
- First-line symptom control: Somatostatin analogue (SSA) therapy — octreotide LAR 20 mg IM monthly or lanreotide Autogel 120 mg SC 28-dayly — controls flushing and diarrhoea in ~70 % of patients.
- Surgical cure: Hepatic resection or cytoreductive surgery should be considered in patients with resectable liver metastases, as symptom control and survival benefit are well established.
- Peptide receptor radionuclide therapy (PRRT): 177Lu-DOTATATE (Lutathera®) is PBS-listed (Authority Required) for progressive, somatostatin receptor–positive midgut NETs and improves progression-free survival.
- Carcinoid heart disease: Echocardiography is mandatory at diagnosis; right-sided valvular fibrosis (tricuspid regurgitation, pulmonary stenosis) occurs in up to 50 % of patients with longstanding syndrome.
- Carcinoid crisis prevention: IV octreotide 250–500 µg bolus pre-procedure/anaesthesia is essential to prevent life-threatening carcinoid crisis; avoid catecholamine-releasing agents.
- Dietary modification: Avoid serotonin-rich foods (bananas, avocados, tomatoes, walnuts, plums) to reduce 5-HIAA production and diarrhoea severity.
- Palliative symptom agents: Loperamide for breakthrough diarrhoea (PBS General Benefit); telotristat ethyl (Xermelo®) for refractory diarrhoea on SSA (not yet PBS-listed in Australia).
- Multidisciplinary care: All patients require NET multidisciplinary team (MDT) review at a specialised centre (e.g., Royal North Shore Hospital Sydney, Peter MacCallum Cancer Centre Melbourne).
- 5-year survival: Localised midgut NET 90–95 %; distant metastatic disease with carcinoid syndrome 50–60 %; carcinoid heart disease significantly worsens prognosis.
Introduction & Australian Epidemiology
Carcinoid syndrome is a paraneoplastic condition caused by the systemic release of vasoactive amines — most notably serotonin (5-hydroxytryptamine, 5-HT) — from well-differentiated neuroendocrine tumours (NETs). In Australia, gastroenteropancreatic NETs are the second most common gastrointestinal malignancy after colorectal cancer, with an age-standardised incidence of approximately 5–7 per 100 000 per year. The syndrome itself develops in roughly 20–30 % of patients with midgut (small-bowel) NETs that have metastasised to the liver, where vasoactive substances bypass first-pass hepatic metabolism.
Historically termed "carcinoid" (from the German karzinoide, meaning carcinoma-like), these tumours are now classified under the umbrella of gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs) by the WHO 2019 classification. The hallmark symptoms — episodic flushing, secretory diarrhoea, and right-sided cardiac valvular fibrosis — result from the direct pharmacological effects of serotonin, histamine, tachykinins, and prostaglandins on the cardiovascular, gastrointestinal, and pulmonary systems.
Australian data from the Australasian Gastro-Intestinal Trials Group (AGITG) and Cancer Council registries indicate that the median age at diagnosis is 55–65 years, with a slight female predominance. The small intestine (ileum) is the primary site in ~40 % of cases, followed by the appendix, lung, and rectum. Approximately 60–70 % of patients present with metastatic disease at diagnosis, underscoring the importance of early biochemical and imaging screening.
Management has evolved considerably with the introduction of somatostatin analogues, peptide receptor radionuclide therapy (PRRT), and targeted agents, shifting the paradigm from purely palliative symptom control toward disease modification. All patients should be managed through a specialised NET MDT in accordance with the eviQ NET protocols endorsed by Cancer Institute NSW.
Pathophysiology & Tumour Sites
Carcinoid tumours arise from enterochromaffin (EC) cells of the diffuse neuroendocrine system. The pathophysiology of carcinoid syndrome is primarily driven by the overproduction and systemic release of serotonin and other vasoactive mediators.
Serotonin Pathway
Tryptophan is hydroxylated to 5-hydroxytryptophan (5-HTP) by tryptophan hydroxylase, then decarboxylated to serotonin (5-HT) by aromatic L-amino acid decarboxylase. Serotonin is metabolised by monoamine oxidase (MAO) in the liver and lungs to 5-hydroxyindoleacetic acid (5-HIAA), which is renally excreted. In patients with hepatic metastases, serotonin enters the systemic circulation directly, bypassing hepatic first-pass metabolism and causing the clinical syndrome.
Other Vasoactive Substances
- Histamine: Contributes to flushing and gastric acid hypersecretion.
- Tachykinins (substance P, neurokinin A): Mediate bronchospasm and flushing.
- Prostaglandins: Contribute to diarrhoea and flushing.
- Kallikrein: Generates bradykinin, which causes vasodilation and flushing.
Primary Tumour Sites & Syndromic Associations
| Primary Site | % of All NETs | Syndrome Association | Venous Drainage |
|---|---|---|---|
| Small bowel (ileum) | ~40 % | Carcinoid syndrome (most common cause) | Portal → hepatic (syndrome requires liver metastases) |
| Appendix | ~25 % | Rarely causes syndrome | Portal |
| Lung (bronchial) | ~25 % | Carcinoid syndrome WITHOUT liver mets (drains to systemic circulation) | Pulmonary → systemic |
| Rectum | ~5 % | Rarely causes syndrome | Portal (inferior rectal → systemic, but small tumours) |
| Pancreas | ~3 % | Functioning syndromes (insulinoma, gastrinoma); non-functioning common | Portal |
Carcinoid Heart Disease (Hedinger Syndrome)
Chronic serotonin exposure causes fibrosis of the right-sided cardiac valves (tricuspid and pulmonary), leading to tricuspid regurgitation and/or pulmonary stenosis. Left-sided valve involvement is uncommon because serotonin is metabolised during pulmonary transit. Up to 50 % of patients with longstanding carcinoid syndrome develop echocardiographic evidence of carcinoid heart disease.
Clinical Features (Flushing & Diarrhoea)
Carcinoid syndrome classically presents with a triad of flushing, diarrhoea, and right-sided cardiac valvular disease. Symptoms are often episodic, triggered by alcohol, stress, exercise, tyramine-rich foods, or catecholamines.
Flushing
- Appearance: Episodic, deep red to violaceous erythema of the face, neck, and upper trunk; may last minutes to hours.
- Triggers: Alcohol, emotional stress, spicy foods, certain medications (catecholamines, opioids).
- Mechanism: Primarily mediated by serotonin, bradykinin, histamine, and substance P.
- Mastocytosis differentiation: Carcinoid flushing is typically deeper red/violaceous and lacks urticaria or Darier sign seen in mastocytosis.
Diarrhoea
- Character: Secretory, watery, often profuse (≥ 3–6 bowel motions/day); can be debilitating.
- Mechanism: Serotonin increases gut motility and secretion; prostaglandins and tachykinins contribute.
- Malabsorption: Chronic serotonin excess may cause fibrosis of mesenteric vessels leading to intestinal ischaemia and malabsorption.
Other Clinical Features
| Feature | Mechanism | Frequency |
|---|---|---|
| Flushing | Serotonin, bradykinin, histamine | ~85 % |
| Diarrhoea | Serotonin, prostaglandins | ~75 % |
| Wheezing / bronchospasm | Serotonin, tachykinins | ~20 % |
| Right heart failure | Serotonin-induced valvular fibrosis | ~40–50 % (longstanding) |
| Pellagra (niacin deficiency) | Tryptophan diverted to serotonin → niacin deficiency | ~5 % |
| Mesenteric fibrosis | Serotonin-induced desmoplasia | ~30–40 % |
Investigations (5-HIAA & Imaging)
Biochemical Investigations
Imaging Investigations
Other Investigations
- Transthoracic echocardiography (TTE): Mandatory at diagnosis to screen for carcinoid heart disease. Look for tricuspid valve thickening/restriction, pulmonary valve stenosis, and right heart failure. Repeat annually if syndrome is active.
- Tissue biopsy / histopathology: WHO 2019 grading — G1 (Ki-67 < 3 %), G2 (Ki-67 3–20 %), G3 (Ki-67 > 20 %). Immunohistochemistry: synaptophysin+, chromogranin A+.
- Baseline FBC, LFTs, renal function, HbA1c: To assess comorbidities and guide treatment dosing.
Management (Octreotide & Surgery)
Management of carcinoid syndrome requires a multimodal approach: symptom control with somatostatin analogues, disease-modifying therapy (surgery, PRRT), and treatment of complications (carcinoid heart disease, mesenteric fibrosis). All treatment decisions should be discussed at a NET MDT.
Somatostatin Analogues — First-Line Symptom Control
Surgical & Locoregional Therapy
- Primary tumour resection: Recommended for all resectable midgut NETs, even with distant metastases, to reduce tumour burden and prevent obstruction/mesenteric fibrosis.
- Hepatic resection: Considered for patients with ≤ 3 liver metastases confined to one lobe (or bilobar if surgically feasible). Offers the best long-term symptom-free survival. Performed at specialised hepatobiliary centres.
- Hepatic arterial embolisation (TAE) / chemoembolisation (TACE): For unresectable liver-dominant disease. TACE with doxorubicin or cisplatin can achieve symptom response in 50–80 %. Available at major centres.
- Radiofrequency ablation (RFA) / microwave ablation: For small (< 3 cm), limited-number liver metastases. Can be combined with surgery.
Peptide Receptor Radionuclide Therapy (PRRT)
Carcinoid Crisis Prevention & Perioperative Management
Adjunctive & Supportive Therapies
| Agent | Indication | Dose | PBS |
|---|---|---|---|
| Loperamide | Breakthrough diarrhoea | 2 mg PO after each loose stool (max 16 mg/day) | General Benefit |
| Codeine phosphate | Refractory diarrhoea | 15–30 mg PO QID PRN | General Benefit |
| Telotristat ethyl (Xermelo®) | Refractory diarrhoea on SSA (≥ 4 stools/day despite SSA) | 250 mg PO TDS with food | Not PBS-listed |
| Nicotinamide (niacin) | Pellagra prevention (niacin deficiency) | 100–300 mg PO daily | Not PBS-listed (OTC) |
| Pancrelipase | Malabsorption due to pancreatic insufficiency | 25 000–50 000 lipase units PO with meals | Restricted Benefit |
Treatment Algorithm Summary
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Ramage JK, Ahmed A, Ardill J, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours. Gut. 2012;61(1):1–22.
- 2. Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 trial of 177Lu-DOTATATE for midgut neuroendocrine tumors. N Engl J Med. 2017;376(2):125–135.
- 3. Caplin ME, Pavel M, Ćwikła JB, et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N Engl J Med. 2014;371(3):224–233.
- 4. Rindi G, Klimstra DS, Abedi-Ardekani B, et al. A common classification framework for neuroendocrine neoplasms: an International Agency for Research on Cancer (IARC) and WHO expert consensus proposal. Mod Pathol. 2018;31(12):1770–1786.
- 5. Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2021. Canberra: AIHW; 2021. Available from: www.aihw.gov.au.
- 6. Krug S, Boch M, Daniel HN, et al. Somatostatin analogues in the treatment of neuroendocrine tumours: past, present and future. Int J Mol Sci. 2012;13(10):12750–12768.
- 7. Rinke A, Müller HH, Schade-Brittinger C, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol. 2009;27(28):4656–4663.
- 8. Fox DJ, Khattar RS. Carcinoid heart disease: presentation, diagnosis, and management. Heart. 2004;90(10):1224–1228.
- 9. Sadowski SM, Neychev V, Millo C, et al. Prospective study of 68Ga-DOTATATE PET/CT for detecting gastro-entero-pancreatic neuroendocrine tumours and unknown primary sites. J Clin Oncol. 2016;34(6):588–596.
- 10. Cancer Institute NSW. eviQ — Neuroendocrine tumours of the small intestine. Sydney: Cancer Institute NSW; 2024. Available from: www.eviq.org.au.
- 11. PBS Online. Pharmaceutical Benefits Scheme — Lutathera. Australian Government Department of Health; 2024. Available from: www.pbs.gov.au.
- 12. National Health and Medical Research Council (NHMRC). National Statement on Ethical Conduct in Human Research. Canberra: NHMRC; 2023.